Sleep-Physiology.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How to Take a Sleep History
1/25/2015 How to take a sleep history Joan Santamaria Neurology Service and Multidisciplinary Sleep Disorders Unit Hospital Clínic of Barcelona 1.- Clinical history: Fundamental: the best “sleep test” Examination: helpful, but not always 2.- Investigations : Sleep tests: PSG, Video-PSG, respiratory polygraphy, MSLT, MWT, actimetry 3.- To rush into a sleep test without considering the history is of little use Taking a good sleep history The bed partner is essential By definition, people is unconscious during sleep Parasomnias, PLMs, Snoring, Sleep apnea, Seizures Daytime sleepiness may be neglected by some patients Even in insomnia patients, the bed partner information may be helpful 1 1/25/2015 Three main complaints I cannot sleep as much as I want (insomnia) Excessive daytime sleepiness (hypersomnia) Abnormal behaviors during sleep (parasomnias and other problems…noise, apnea, enuresis, seizures… ) What are the main questions? Nocturnal sleep characteristics Schedule of sleep during the week and week-end or holidays Latency to sleep, number of awakenings and cause (bathroom, pain, nightmare...) Time and type of final awakening (spontaneous/induced) Feel refreshed / tired on awakening? 23 1 4:30 6 8 Nocturnal sleep pattern Sleep onset insomnia 24 1:30 7:30 Delayed sleep phase 24 3 12 Week day Insufficient sleep 24 5:30 1 11 Week end (> 2 hrs additional sleep duration on week ends, high sleep efficiency) 2 1/25/2015 Sleep diary DEFINITION OF INSOMNIA Two key elements Nocturnal sleep: Difficulty in sleeping as much or as deep as one would -

Sleep and Its Disorders: Is the Problem
38 ISSN 0049-6804. «Врачеб. дело». 2017, № 1–2 ОБЗОР ЛИТЕРАТУРЫ 43. Williams G. R., Duncan Bassett J. H. Local control of thyroid hormone action: role of type 2 deiodinase Deiodinases: the balance of thyroid hormone // J. of Endocrinol. – 2011. – Vol. 209. – P. 261–272. 44. Wittmann G., Harney J. W., Singru P. S. et al. Inflammation-inducible type 2 deiodinase expres- sion in the leptomeninges, choroid plexus, and at brain blood vessels in male rodents // Endocri- nology. – 2014. – Vol. 155. – P. 2009–2019. 45. Yu J., Koenig R. J. Induction of type 1 iodothyronine deiodinase to prevent the nonthyroidal illness syndrome in mice // Endocrinol. – 2006. – Vol. 147, N 7. – Р. 3580–3585. СУЧАСНІ УЯВЛЕННЯ ПРО СИНДРОМ НЕТИРЕОЇДНОЇ ПАТОЛОГІЇ В КЛІНІЧНІЙ ПРАКТИЦІ Н. О. Абрамова, Н. В. Пашковська (Чернівці) Будь-які гострі та хронічні захворювання, що втягують у патологічний процес весь організм, можуть викликати порушення обміну тиреоїдних гормонів на фоні відсутності супутньої патології щитоподібної залози, гіпофіза та (або) гіпоталамуса. Такі порушення називають «син- дромом нетиреоїдної патології» (СНТП), або «синдромом низького Т3», і зустрічаються у 70 % госпіталізованих. У даному огляді ми розглянули етіологію, патогенез та частково шляхи корекції синдрому нетиреоїдної патології. Ключові слова: синдром нетиреоїдної патології, синдром низького Т3, порушення обміну тиреоїдних гормонів. CURRENT VIEWS ON NONTHYROIDAL ILLNESS SYNDROME IN CLINICAL PRACTICE (REVIEW) N. O. Abramova, N. V. Pashkovska (Chernivtsi, Ukraine) Higher State Educational Establishment of Ukraine «Bukovinian State Medical University» Any acute and chronic diseases that involve the whole organism into pathological process, can cause violation of thyroid hormones metabolism against a background of absence of concomitant diseases of thyroid gland, pituitary gland or hypothalamus. -

Sleep Epidemiology--A Rapidly Growing Field Jane E
Sleep epidemiology--a rapidly growing field Jane E. Ferrie 1 * , Meena Kumari 2 , Paula Salo 3 , Archana Singh-Manoux 2 4 , Mika Kivimäki 2 3 1 School of Community and Social Medicine University of Bristol , Bristol,GB 2 Department of Epidemiology and Public Health University College of London (UCL) , 1-19 Torrington Place London WC1E 6BT,GB 3 Finnish Institute of Occupational Health Finnish Institute of Occupational Health , Topeliuksenkatu 41A 00250 Helsinki,FI 4 CESP, Centre de recherche en épidémiologie et santé des populations INSERM : U1018 , Université Paris XI - Paris Sud , Hôpital Paul Brousse , Assistance publique - Hôpitaux de Paris (AP-HP) , 16 avenue Paul Vaillant Couturier 94807 Villejuif Cedex, France,FR * Correspondence should be addressed to: Jane Ferrie <[email protected] > MESH Keywords Chronic Disease ; Health Status ; Humans ; Polysomnography ; Sleep ; Sleep Disorders ; epidemiology ; genetics ; Sleep Stages Introduction The human body has adapted to daily changes in dark and light such that it anticipates periods of sleep and activity. Deviations from this circadian rhythm come with functional consequences. Thus, 17 hours of sustained wakefulness in adults leads to a decrease in performance equivalent to a blood alcohol-level of 0.05%;[1 ] the legal level for drink driving in many countries.[2 ] Rats deprived of sleep die after 32 days,[3 ] and, with longer periods of sleep deprivation, this would also be the case in human beings. Indeed, sleep deprivation is a common form of torture.[4 ] Given the readily observable effects of sleep in everyday life, it is not surprising that there has been scholarly interest in sleep since the beginning of recorded history.[5 ] Sleep epidemiology as a subject in its own right has a recognisable history of just over 30 years,[6 ] with the first modern epidemiological studies of sleep disturbances appearing around 1980.[7 ;8 ] Nevertheless, a PubMed search for terms “ sleep/insomnia” and “epidemiology” shows that the cumulative number of papers on the subject over the past 10 years is already about 10,000. -

Sleepiness the Wheel
SLEEPINESS AT THE WHEEL WHITE PAPER SLEEPINESS AT THE WHEEL WHITE PAPER Sleepiness at the Wheel WHITE PAPER PREFACE Improving road safety is a priority of the French Government. Among the various causes of road accidents, one of them is especially common on motorways: lack of alertness, which leads to inattention and sleepiness. Lack of alertness is responsible for one in three collisions resulting in deaths on the motorway network, although it is the safest of all road networks! This phenomenon is not fully grasped by the public. Therefore, it is essential to gain knowledge and raise the publics’ awareness as regards sleepiness at the wheel. In more general terms, sleepiness at the wheel remains underestimated both socially and culturally speaking, which is a major issue for road safety and public health. This white book, put together by the French Motorway Companies (ASFA) and the National Institute of Sleep and Vigilance (INSV), presents the most recent knowledge on the subject at both the French and European levels and provides a number of recommendations. By contributing to a better understanding of sleepiness at the wheel, this work will help promote the implementation of new prevention strategies, to further reduce the number of victims on the road. Our objective is to cut down to less than 2000 the number of deaths per year on French roads by 2020. Manuel VALLS French Minister of Interior ASFA and INSV would like to express their deep thanks to the panel of European sleep experts who author this book. Most of them also participate in the research on traffic accidents associated with sleepiness in their own country and thus have contributed to enrich our knowledge and proposals for preventing from the consequences of sleepiness at the wheel. -

Parasomnias Revisited New Mexico Thoracic Society Sapna Bhatia Md 02/25/17 Objectives
PARASOMNIAS REVISITED NEW MEXICO THORACIC SOCIETY SAPNA BHATIA MD 02/25/17 OBJECTIVES • Appreciate the clinical semiology to help differentiate between REM and NREM parasomnias • Appreciate the ICSD III Classification Scheme for the major parasomnias • Understand management modalities including behavioral and pharmacological for NREM and REM parasomnias • Understand the difference between parasomnias and seizures WHAT ARE PARASOMNIAS? Undesirable motor, or verbal phenomena that arise from sleep or sleep-wake transition PARASOMNIAS: OVERLAPPING STATES REM PARASOMNIAS WAKE NREM PARASOMNIAS REM NREM PARASOMNIAS: DIFFERENTIAL DIAGNOSIS RBD Confusional Arousals Recurrent Isolated Sleep Paralysis Sleepwalking Nightmare Disorder Sleep Terrors WAKE Sleep Related Eating Disorder REM NREM PYSCHOGENIC SEIZURES SPELLS NFLE Dissociative Disorder ICSD II ICSD III REM Parasomnias • RBD • RBD • Recurrent Isolated Sleep • Recurrent Isolated Sleep Paralysis ICSD II VS ICSDParalysis III CLASSIFICATION• Nightmare Disorder • Nightmare Disorder Disorders of arousal • Confusional Arousals • Confusional Arousals (NREM sleep) • Sleepwalking • Sleep Walking • Sleep Terrors • Sleep Terrors • SRED Other Parasomnias • SRED • Sleep Related Dissociative • Sleep Related Dissociative Disorders Disorders • Sleep Enuresis • Sleep Enuresis • Catathrenia SDB • Catathrenia • Exploding Head Syndrome • Exploding Head syndrome • Sleep Related Hallucinations • Sleep Related Hallucinations • Parasomnia, Unspecified • Parasomnia, Unspecified • Parasomnia due to Drug or • Parasomnia -
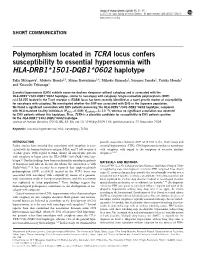
Polymorphism Located in TCRA Locus Confers Susceptibility to Essential Hypersomnia with HLA-DRB1&Ast;1501-DQB1&Ast;0602
Journal of Human Genetics (2010) 55, 63–65 & 2010 The Japan Society of Human Genetics All rights reserved 1434-5161/10 $32.00 www.nature.com/jhg SHORT COMMUNICATION Polymorphism located in TCRA locus confers susceptibility to essential hypersomnia with HLA-DRB1*1501-DQB1*0602 haplotype Taku Miyagawa1, Makoto Honda2,3, Minae Kawashima1,4, Mihoko Shimada1, Susumu Tanaka2, Yutaka Honda3 and Katsushi Tokunaga1 Essential hypersomnia (EHS) exhibits excessive daytime sleepiness without cataplexy and is associated with the HLA-DRB1*1501-DQB1*0602 haplotype, similar to narcolepsy with cataplexy. Single-nucleotide polymorphism (SNP) rs1154155 located in the T-cell receptor a (TCRA) locus has been recently identified as a novel genetic marker of susceptibility for narcolepsy with cataplexy. We investigated whether the SNP was associated with EHS in the Japanese population. We found a significant association with EHS patients possessing the HLA-DRB1*1501-DQB1*0602 haplotype, compared À4 with HLA-matched healthy individuals (Pallele¼0.008; Ppositivity¼5Â10 ), whereas no significant association was observed for EHS patients without this haplotype. Thus, TCRA is a plausible candidate for susceptibility to EHS patients positive for the HLA-DRB1*1501-DQB1*0602 haplotype. Journal of Human Genetics (2010) 55, 63–65; doi:10.1038/jhg.2009.118; published online 20 November 2009 Keywords: essential hypersomnia; HLA; narcolepsy; TCRA INTRODUCTION possible association between SNP rs1154155 in the TCRA locus and Earlier studies have revealed that narcolepsy with cataplexy is asso- essential hypersomnia (EHS), CNS hypersomnia similar to narcolepsy ciated with the human leukocyte antigen (HLA) and T-cell receptor a with cataplexy, with regard to the symptom of excessive daytime (TCRA) genes. -

Sleep Disorders and Sleep Deprivation: an Unmet Public Health Problem
REPORT BRIEF • APRIL 2006 SLEEP DISORDERS AND SLEEP DEPRIVATION: AN UNMET PUBLIC HEALTH PROBLEM It is estimated that 50 to 70 million Americans chronically suffer from a disorder of sleep and wakefulness, hindering daily functioning and adversely affecting their health and longevity. The cumulative effects of sleep loss and sleep disorders represent an under-recognized public health problem and have been associated with a wide range of health consequences including an increased risk of hypertension, diabetes, obesity, depression, heart attack, and stroke. Almost 20 percent of all serious car crash injuries in the general population are associated with driver sleepiness. Hundreds of billions of dollars a year are spent on direct medical costs related to sleep disorders such as doctor visits, hospital services, prescriptions, and over-the-counter medications. Recognizing the health consequences of sleep disorders and sleep deprivation, the American Academy of Sleep Medicine, the National Center on Sleep Disorders Research at the National Institutes of Health, the National Sleep Foundation, and the Sleep Research Society The cumulative requested that the Institute of Medicine review the public health effects of sleep loss significance of sleep, sleep loss, and sleep disorders; examine gaps and sleep disorders in research, education, and training in the public health system and academia; and provide a comprehensive plan for enhancing sleep represent an under- medicine and research. recognized public Sleep Disorders and Sleep Deprivation: An Unmet Public Health health problem and Problem concluded that although scientific opportunities and clinical have been associat- activities in the field are expanding, the available human resources and ed with a wide infrastructural capacity to improve patient care and expand scientific range of health research are insufficient. -

Parasomnias and Antidepressant Therapy: a Review of the Literature
REVIEW ARTICLE published: 12 December 2011 PSYCHIATRY doi: 10.3389/fpsyt.2011.00071 Parasomnias and antidepressant therapy: a review of the literature Lara Kierlin1,2 and Michael R. Littner 1,2* 1 David Geffen School of Medicine at University of California Los Angeles, Los Angeles, CA, USA 2 Pulmonary, Critical Care and Sleep Medicine, VA Greater Los Angeles Healthcare System, Los Angeles, CA, USA Edited by: There exists a varying level of evidence linking the use of antidepressant medication to Ruth Benca, University of the parasomnias, ranging from larger, more comprehensive studies in the area of REM Wisconsin – Madison School of Medicine, USA sleep behavior disorder to primarily case reports in the NREM parasomnias. As such, prac- Reviewed by: tice guidelines are lacking regarding specific direction to the clinician who may be faced Ruth Benca, University of with a patient who has developed a parasomnia that appears to be temporally related to Wisconsin – Madison School of use of an antidepressant. In general, knowledge of the mechanisms of action of the med- Medicine, USA ications, particularly with regard to the impact on sleep architecture, can provide some David Plante, University of Wisconsin, USA guidance. There is a potential for selective serotonin reuptake inhibitors, tricyclic antide- *Correspondence: pressants, and serotonin–norepinephrine reuptake inhibitors to suppress REM, as well Michael R. Littner, 10736 Des Moines as the anticholinergic properties of the individual drugs to further disturb normal sleep Avenue, Porter Ranch, Los Angeles, architecture. CA 91326, USA. e-mail: [email protected] Keywords: parasomnias, REM sleep behavior disorder, non-REM parasomnias, selective serotonin reuptake inhibitors, depression INTRODUCTION and night terrors (Ohayon et al., 1999; Yeh et al., 2009). -
Somnology-Jr-Book.Pdf
1 To Grace Zamudio and Zoe Lee-Chiong. 2 Preface Carpe noctem. Teofilo Lee-Chiong MD Professor of Medicine Division of Sleep Medicine National Jewish Health Denver, Colorado University of Colorado Denver School of Medicine Denver, Colorado Chief Medical Liaison Philips Respironics Murrysville, Pennsylvania 3 Abbreviations AHI Apnea-hypopnea index BPAP Bi-level positive airway pressure CPAP Continuous positive airway pressure CSA Central sleep apnea ECG Electrocardiography EEG Electroencephalography EMG Electromyography EOG Electro-oculography FEV1 Forced expiratory volume in 1 second GABA Gamma-aminobutyric acid N1 NREM stage 1 sleep N2 NREM stage 2 sleep N3 NREM stages 3 (and 4) sleep NREM Non-rapid eye movement O2 Oxygen OSA Obstructive sleep apnea PaCO2 Partial pressure of arterial carbon dioxide PaO2 Partial pressure of arterial oxygen REM Rapid eye movement sleep SaO2 Oxygen saturation SOREMP Sleep onset REM period 4 Table of contents Introduction 15 Neurobiology of sleep 16 Neural systems generating wakefulness 16 Neural systems generating NREM sleep 16 Neural systems generating REM sleep 16 Main neurotransmitters 17 Acetylcholine 17 Adenosine 17 Dopamine 17 Gamma-aminobutyric acid 17 Glutamate 17 Glycine 17 Histamine 18 Hypocretin 18 Melatonin 18 Norepinephrine 18 Serotonin 18 Physiology during sleep 19 Autonomic nervous system 19 Respiratory system 19 Respiratory patterns 19 Cardiovascular system 19 Gastrointestinal system 20 Renal and genito-urinary systems 20 Endocrine system 20 Growth hormone 20 Thyroid stimulating hormone -
Sleep Disorders As Outlined by Outlined As Disorders Sleep of Classification N the Ribe the Features and Symptoms of Each Disorder
CHAPTER © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION 2NOT FOR SALE OR DISTRIBUTION © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FORSleep SALE OR DISTRIBUTION Disorders NOT FOR SALE OR DISTRIBUTION © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION © Agsandrew/Shutterstock © Jones & Bartlett Learning, LLC © Jones & Bartlett Learning, LLC NOT FOR SALE OR DISTRIBUTION NOT FOR SALE OR DISTRIBUTION CHAPTER OUTLINE EEG arousal alveolar hypoventilation paradoxical breathing idiopathic central alveolar History of Sleep Disorders© Jones & Bartlett Learning, LLCmicrognathia © Joneshypoventilation & Bartlett Learning, LLC Classification of Sleep DisordersNOT FOR SALE OR DISTRIBUTIONretrognathia NOTsnoring FOR SALE OR DISTRIBUTION Insomnia apnea–hypopnea primary snoring Sleep-Related Breathing Disorders index (AHI) sleep-related groaning Central Disorders of Hypersomnolence respiratory disturbance catathrenia Circadian Rhythm Sleep–Wake Disorders index (RDI) CPAP therapy Parasomnias respiratory effort–related positional therapy Sleep-Related© Jones Movement & Bartlett Disorders Learning, LLC arousal (RERA)© Jones & Bartletttonsillectomy Learning, LLC OtherNOT Sleep FOR Disorders SALE OR DISTRIBUTION upper-airwayNOT resistance FOR SALEadenoidectomy OR DISTRIBUTION Chapter Summary syndrome bi-level therapy excessive daytime multiple sleep latency LEARNING OBJECTIVES sleepiness (EDS) test (MSLT) sudden infant -

Periodic Limb Movement Disorder: Characteristics
SLEEP SCIENCE : SLEEP , SLEEPINESS , AND SLEEPLESSNESS Kenneth Lichstein, Ph.D. Professor Emeritus Department of Psychology The University of Alabama sleeplessness II a lot can go wrong topics (among 70 sleep disorders) sleep apnea narcolepsy restless legs periodic limb movements disorders we won’t talk about exploding head syndrome sexsomnia sleep-related epilepsy catathrenia if left untreated, sleep apnea is a slow moving terminal illness Pickwickian syndrome (now called obesity-hypoventilation syndrome) obesity, daytime labored breathing, daytime sleepiness ̶ Burwell et al., 1956 10 years later sleep apnea “Nocturnal polygraphic registrations disclosed respiratory pauses…” ̶ Gastaut et al., 1966 invisible sleep apnea science advances by two processes ❑ steady, incremental, systematic research ❑ abrupt, accidental discovery o Between 1956 and 1966, 10s of thousands of PSGs had been performed world wide and no one noticed some people had quit breathing. o Bed partners were not complaining that their partner had quit breathing. when you don’t know what you are looking for, you don’t see the obvious benign snoring and sleep apnea moderate and severe snoring sleep apnea benign snoring I snoring without breath cessation ▪ occurs in 10-15% of population ▪ sleeping on back increases likelihood of snoring ▪ snorer usually has no knowledge of condition ▪ more troublesome to bed partner ▪ at 5-year follow-up, benign snoring (without weight gain) is not a risk factor for sleep apnea physiology ▪ partial airway obstruction ▪ on continuum -

2018 ANNUAL REPORT SHF-Annualreport-0918.Qxp Layout 1 26/9/18 2:54 Pm Page 2
SHF-AnnualReport-0918.qxp_Layout 1 26/9/18 2:54 pm Page 1 2018 ANNUAL REPORT SHF-AnnualReport-0918.qxp_Layout 1 26/9/18 2:54 pm Page 2 Special Reports prepared by the Sleep Health Foundation Wake Up Australia: The Value of million Australian adults, 9% of the adult Sleep Health Foundation national survey. Sleep Health. Healthy Sleep 2004 population, now suffer from sleep disorders. 2017 Oct;3(5):357-361. (4) Appleton SL, Gill TK, Lang CJ, Taylor AW, McEvoy The report was funded by an unrestricted grant The report was commissioned by the Sleep RD, Stocks NP, González-Chica DA, Adams RJ. from the ResMed Foundation Limited who had Health Foundation conducted by Deloitte Access Prevalence and comorbidity of sleep conditions in no part in the direction or findings contained in Economics. Australian adults: 2016 Sleep Health Foundation this report. Subsequent publications: national survey. Sleep Health. 2018 Feb;4(1):13-19. This report commissioned by the Committee of Hillman DR, Lack LC. Public health implications of sleep loss: the community burden. Med J Aust. Sleep Health Australia (pre Sleep Health 2013;199:S7-10. Asleep on the Job: costs of Foundation) and prepared by Access Economics inadequate sleep in Australia in 2004. Sleep and Mental Wellbeing – Subsequent publications: The report, prepared by Deloitte Access exploring the links Economics, investigated the economic Hillman DR, Scott-Murphy A, Antic R, Pezzullo L. The consequences of inadequate sleep in the economic cost of sleep disorders. Sleep 2006; A research report from health promotion 29:299-305. foundation VicHealth and the Sleep Health 2016-17 financial year.