Acid Peptic Diseases in the Pediatric
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Perforated Peptic Ulcer in Khartoum State
ﺑﺴﻢ ﺍﷲ ﺍﻟﺮﲪﻦ ﺍﻟﺮﺣﻴﻢ UNIVERSITY OF KHARTOUM Faculty of Medicine Postgraduate Medical Studies Board Perforated peptic ulcer in Khartoum state By Dr. Al Fatih Mohamed Ahmed Alnajib M.B.B.S (University of Gezira) A thesis Submitted in partial fulfillment for the requirements of the Degree of Clinical MD in Surgery, October, 2002 Supervisor Prof. Mohamed El Makki Ahmed MS, FRCSI, Professor of Surgery ﺑﺴﻢ ﺍﷲ ﺍﻟﺮﲪﻦ ﺍﻟﺮﺣﻴﻢ ﻗﺎﻝ ﺍﷲ ﺗﻌﺎﻟﻰ : } ﻗﺎﻟﻮﺍ ﺳﺒﺤﺎﻧﻚ ﻻ ﻋﻠﻢ ﻟﻨﺎ ﺇﻻ ﻣﺎ ﻋﻠﻤﺘﻨﺎ ﺇﻧﻚ .{ ﺃﻧﺖ ﺍﻟﻌﻠﻴﻢ ﺍﻟﺤﻜﻴﻢ ﺻﺪﻕ ﺍﷲ ﺍﻟﻌﻈﻴﻢ CONTENTS Page Dedication I Acknowledgements II List of abbreviations III English abstract IV V Arabic abstract VI List of tables VIII List of figures CHAPTER ONE 1 Introduction and Literature review Objectives 25 CHAPTER TWO Patients & Methods 26 CHAPTER THREE Results 28 CHAPTER FOUR Discussion 58 Conclusion 65 Recommendations 67 References 68 APPENDIX Questionnaire 69 APACHE II Score 73 Dedications To my parents, teachers, Sisters & brothers ACKNOWLEDGEMENT I will always feel indebted to my supervisor Prof. Mohamed El Makki Ahmed, Professor of surgery, Faculty of Medicine, University of Khartoum, for his kind and meticulous supervision, encouragement, and guidance in this work with great patience from it’s beginning to the final touches. I would also like to express my sincere thanks and gratitude to my colleagues the registrars of surgery and the house officers who help a lot in data collection, their indefatigable efforts and cheerful co-operation are without parallel. Special thanks for all those helped or participated in this work to come to the light, not forgetting to thank Miss. Widad for help in typing and Mr. -

4. Pathology Esophagus and Stomach
Pathology of esophagus and stomach. Pathology of esophagus and stomach. I. Microspecimens: № 176. Acute gastric ulcer. (H.E. stain). Indications: 1. The superficial layer of the ulcer, consisting of leukocytes and erythrocytes. 2. Necrotic masses and tissue debris in the area of the ulcer. 3. Foci of necrosis in the muscular layer of the gastric wall. 4. Leukocyte infiltration in the edges and bottom of the ulcer. A lesion in the gastric wall is observed, which involves the mucosa, the muscularis mucosa and the submucosa; the bottom of the ulcer is presented by necrotic masses with diffuse leukocyte infiltration, which extends into the muscular layer of the gastric wall; blood vessels are dilated, hyperemic; there is no granulation tissue or mature fibrocollagenous tissue. Acute gastric ulcers are located more frequently on the lesser curvature, in the antral and pyloric region, they can also be on the greater curvature. They are usually multiple, more often round in shape, diameter up to 1.0-1.5 cm, the bottom is dark brown due to the accumulation of the hemoglobinogen pigment, hydrochloric hematin. The edges and bottom have a flaccid consistency, they are not hardened, the arrangement of the folds of the adjacent mucosa is not changed. In some cases, the acute ulcer can progress with involvement of the muscular layer of the gastric wall and even the serosa, which can lead to perforation and peritonitis. Deep acute ulcers often look like a funnel, with the base facing the gastric mucosa and the tip facing the serous membrane. Another complication is gastric bleeding. -

Role of Yoga in Acid Peptic Disease: a Review
wjpmr, 2021,7(9), 133 – 136. SJIF Impact Factor: 5.922 WORLD JOURNAL OF PHARMACEUTICAL Review Article Navedita et al. World Journal of Pharmaceutical and Medical Research AND MEDICAL RESEARCH ISSN 2455-3301 www.wjpmr.com Wjpmr ROLE OF YOGA IN ACID PEPTIC DISEASE: A REVIEW *1Dr. Navedita Kumari and 2Dr. Anupam Pathak 1PG Scholar, Dept of Swasthavritta & Yoga, SriGanganagar College of Ayurvedic Science and Hospital, Tanta University, SriGanganagar. 2HOD, Dept of Swasthavritta & Yoga, SriGanganagar College of Ayurvedic Science and Hospital, Tanta University, SriGanganagar. *Corresponding Author: Dr. Navedita Kumari PG Scholar, Dept of Swasthavritta & Yoga, SriGanganagar College of Ayurvedic Science and Hospital, Tanta University, SriGanganagar. Article Received on 15/06/2021 Article Revised on 05/07/2021 Article Accepted on 25/07/2021 ABSTRACT The acid peptic diseases, also known as acid peptic disorders are a collection of diseases involving acid production in the stomach and nearby parts of the gastrointestinal tract. It includes gastroesophageal reflux disease, gastritis, gastric ulcer, duodenal ulcer, esophageal ulcer, Zollinger–Ellison syndrome and Meckel's [1] diverticulum ulcer. Acid peptic disorders are the result of distinctive, but overlapping pathogenic mechanisms [1] leading to either excessive acid secretion or diminished mucosal defense. Acid peptic disease – commonly called APD – includes a number of conditions. All these conditions are the result of damage from acid and peptic activity in gastric secretions. APD occurs when the acid starts irritating the inner cells (mucosal layer) of the stomach. Acid [2] peptic diseases mostly affect the oesophagus, stomach, and duodenum. “Acid peptic disease” is a collective term used to include many conditions such as gastro-esophageal reflux disease (GERD), gastritis, gastric ulcer, duodenal ulcer, esophageal ulcer, Zollinger Ellison Syndrome (ZES) and Meckel‟s diverticular ulcer. -

Peptic Ulcer Disease
\ Lecture Two Peptic ulcer disease 432 Pathology Team Done By: Zaina Alsawah Reviewed By: Mohammed Adel GIT Block Color Index: female notes are in purple. Male notes are in Blue. Red is important. Orange is explanation. 432PathologyTeam LECTURE TWO: Peptic Ulcer Peptic Ulcer Disease Mind Map: Peptic Ulcer Disease Acute Chronic Pathophysiology Morphology Prognosis Locations Pathophysiology Imbalance Acute severe Extreme Gastric Duodenal gastritis stress hyperacidity between agrresive and defensive Musocal Due to factors increased Defenses Morphology acidity + H. Pylori infection Mucus Surface bicarbonate epithelium barrier P a g e | 1 432PathologyTeam LECTURE TWO: Peptic Ulcer Peptic Ulcer Definitions: Ulcer is breach in the mucosa of the alimentary tract extending through muscularis mucosa into submucosa or deeper. erosi on ulcer Chronic ulcers heal by Fibrosis. Erosion is a breach in the epithelium of the mucosa only. They heal by regeneration of mucosal epithelium unless erosion was very deep then it will heal by fibrosis. Types of Ulcer: 1- Acute Peptic Ulcers ( Stress ulcers ): Acutely developing gastric mucosal defects that may appear after severe stress. Pathophysiology: All new terms mentioned in the diagram are explained next page Pathophysiology of acute peptic ulcer Complication of a As a reult of Due to acute severe stress extreme gastritis response hyperacidity Mucosal e.g. Zollinger- inflammation as a Curling's ulcer Stress ulcer Cushing ulcer Ellison response to an syndrome irritant e.g. NSAID or alcohol P a g e | 2 432PathologyTeam -

The Gastrointestinal Tract Frank A
91731_ch13 12/8/06 8:55 PM Page 549 13 The Gastrointestinal Tract Frank A. Mitros Emanuel Rubin THE ESOPHAGUS Bezoars Anatomy THE SMALL INTESTINE Congenital Disorders Anatomy Tracheoesophageal Fistula Congenital Disorders Rings and Webs Atresia and Stenosis Esophageal Diverticula Duplications (Enteric Cysts) Motor Disorders Meckel Diverticulum Achalasia Malrotation Scleroderma Meconium Ileus Hiatal Hernia Infections of the Small Intestine Esophagitis Bacterial Diarrhea Reflux Esophagitis Viral Gastroenteritis Barrett Esophagus Intestinal Tuberculosis Eosinophilic Esophagitis Intestinal Fungi Infective Esophagitis Parasites Chemical Esophagitis Vascular Diseases of the Small Intestine Esophagitis of Systemic Illness Acute Intestinal Ischemia Iatrogenic Cancer of Esophagitis Chronic Intestinal Ischemia Esophageal Varices Malabsorption Lacerations and Perforations Luminal-Phase Malabsorption Neoplasms of the Esophagus Intestinal-Phase Malabsorption Benign tumors Laboratory Evaluation Carcinoma Lactase Deficiency Adenocarcinoma Celiac Disease THE STOMACH Whipple Disease Anatomy AbetalipoproteinemiaHypogammaglobulinemia Congenital Disorders Congenital Lymphangiectasia Pyloric Stenosis Tropical Sprue Diaphragmatic Hernia Radiation Enteritis Rare Abnormalities Mechanical Obstruction Gastritis Neoplasms Acute Hemorrhagic Gastritis Benign Tumors Chronic Gastritis Malignant Tumors MénétrierDisease Pneumatosis Cystoides Intestinalis Peptic Ulcer Disease THE LARGE INTESTINE Benign Neoplasms Anatomy Stromal Tumors Congenital Disorders Epithelial Polyps -

Path GI – Liver – Gallbladder Paragraph Style
Path GI – Liver – Gallbladder Paragraph Style Esophagus Congenital Hemorrhage Esophagitis Tumors Fistula Mallory‐Weiss GERD Sqaumous Cell Carcinoma Webs Esophageal Varices Barrett’s Adenocarcinoma Achalasia Chemical CONGENITAL Fistula. Fistulas often occur together with atresias. Atresias are where a tube (in this case the esophagus) ends in a blind pouch. A Fistula is where a tube connects to another tube. A Tracheoesophageal fistula is a connection between the trachea and the esophagus. Over 80% of these lesions occur with atresia of the proximal esophagus, and a fistula of the distal esophagus to the trachea. This means that when the baby swallows, the food goes into the trachea! This is pretty clear early on, presenting with dysphagia (spitting up, not vomiting, food), and Coughing + Cyanosis during feeding. Air in stomach may be seen as well. This must be surgically corrected, which is easy to do. Webs. Esophageal webs are simply extensions of mucosal epithelium into the lumen of the esophagus. They act as nets which can catch food trying to be swallowed. This presents with dysphagia and foul breath as the food that gets stuck putrefies in the esophagus. Webs are associated with Plummer‐ Vinson Syndrome from the Heme block, presenting with iron deficiency anemia and an increased risk for sqaumous cell carcinoma. These will persist into adulthood Achalasia. This is a failure of the LES to relax. When food is swallowed, it cannot pass into the stomach, causing distension of the esophagus (megaesophagus) and dysphagia. Over time, the food is pushed through the tight sphincter. It is caused by death of ganglionic cells in the LES. -

Gastroesophageal Reflux Disease & Peptic Ulcer
Case scenario L1&2: Gastroesophageal Reflux Disease & Peptic Ulcer objectives ● Describe the definition, pathogenesis, clinical features, pathology (gross and microscopic features) and complications of reflux esophagitis. ● Describe the definition, main cause, pathology (gross and microscopic features) and complications (dysplasia and adenocarcinoma) of Barrett esophagus. ● Define ulcer and erosion. ● Describe the pathogenesis, pathology and clinical features of acute gastric ulcers. ● Describe the pathogenesis (H pylori, NSAID, Z-E syndrome), clinical features, pathology (gross and microscopic features) and complications (bleeding, perforation, obstruction) of chronic peptic ulcers. Black: original content Orange: Doctor notes Red: Important Grey: Extra/Robbins Green: only found in males slides Purple: Only found in females slides Editing File Lecture Content Physiological GERD reflux Esophagitis (pathological) Severe stress Acute gastritis Hyperacidity response Acute Ulcers Chronic Gastric Duodenal NSAIDs Bile Reflux H. pylori Infection Hyperacidity Esophagitis Reflux esophagitis ● Symptoms or mucosal damage produced by the abnormal reflux of gastric content into the esophagus, often chronic and relapsing. ● Esophagitis is rarely caused by anything other than reflux. ● May see complications of GERD in patients who lack typical symptoms. ● Some other causes include: ○ Infective ■ Fungal infection (common): candida albicans. ■ Viral infection: Herpes simplex and cytomegalovirus in AIDS patients. ■ Bacterial infection is very rare. ○ Physical Agent -
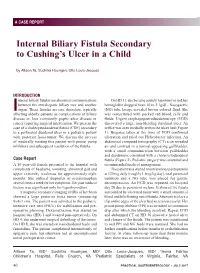
Internal Biliary Fistula Secondary to Cushing's Ulcer in a Child
A CASE REPORT A CASE REPORT Internal Biliary Fistula Secondary to Cushing’s Ulcer in a Child by Allison Ta, Suchitra Hourigan, Otto Louis-Jacques INTRODUCTION nternal biliary fistulas are abnormal communications On HD 11, she became acutely hypotensive and her between the extrahepatic biliary tree and another hemoglobin dropped from 10 to 5.1g/dL. Nasogastric Iorgan. These fistulas are rare disorders, typically (NG) tube lavage revealed brown colored fluid. She affecting elderly patients as complications of biliary was resuscitated with packed red blood cells and disease or, less commonly, peptic ulcer disease or fluids. Urgent esophagogastroduodenoscopy (EGD) cancer requiring surgical intervention. We present the discovered a large, non-bleeding duodenal ulcer. An case of a cholecystoduodenal fistula (CDF) secondary orifice was seen medially within the ulcer bed (Figure to a perforated duodenal ulcer in a pediatric patient 1). Biopsies taken at the time of EGD confirmed with posterior fossa tumor. We discuss the success ulceration and ruled out Helicobacter infection. An of medically treating this patient with proton pump abdominal computed tomography (CT) scan revealed inhibitors and subsequent resolution of the fistula. air and contrast in a normal-appearing gallbladder, with a small communication between gallbladder and duodenum, consistent with a cholecystoduodenal Case Report fistula (Figure 2). Pediatric surgery was consulted and A 10 year-old female presented to the hospital with recommended medical management. complaints of headache, vomiting, abnormal gait and The patient was started on intravenous pantoprazole upper extremity weakness for approximately eight at 120 mg daily (roughly 1.6mg/kg/day), total parenteral months. She utilized ibuprofen or acetaminophen nutrition and a NG tube was placed for gastric several times a week for her symptoms. -

Peptic Ulcer Disease
19 September 2018 Surgery of the stomach and duodenum: Peptic ulcer disease *- Congenital hypertrophic pyloric Nature stenosis Sites of peptic ulcer disease Etiology *- Acute gastric dilatation Types: *- Peptic ulcer disease (acute erosions – *- Gastric erosions (erosive gastritis) chronic peptic ulcer) *- Stress ulcers e.g. ICU patients, trauma patients, intra- *- Gastric volvulus cranial trauma or operations (Cushing ulcer), burned patients (Curling ulcer) *- Bezoars Clinical presentations *- Gastric neoplasms Diagnosis *- Gastrectomy, and its complications Treatment: Medical treatment *- Gastrostomy Endosc. treatment ( injections , Laser, or thermal ttt ) *- Gastric role in bariatric surgery Surgical treatment Gastrectomy ?? 1 Prof. Alaa Ahmad Redwan, 2017 19 September 2018 *- Chronic peptic ulcer Etiology: Increased gastric acidity is the main association, multifactorial by * Genetic predisposition (large parietal cell mass) * Increased vagal tone mainly by night may be by worry or stress * Abnormality in gastrin release and inhibition * Helicobacter pylori causing gastritis, duodenal ulcer and sometimes MALT lymphoma. * Hypergastrinaemia by pancreatic gastrinoma (Zollinger Ellison syndrome) * Spicy meals, drinks, smoking, alcohol , drugs, 2 Prof. Alaa Ahmad Redwan, 2017 19 September 2018 Clinical presentation: Incidence: *- Pain (post prandial , localized , deep, severe, Decreasing incidence of ulcer disease with 50-60% increased by codiments, wores by night) increased GE reflux and gastritis More common in males (5:1), age is around middle *- Nausea and vomiting age (??) *- Periodicity (periods of activity followed by DU : GU = 25 : 1 period of quiescence),loss of periodicity signats 15-20% 15-20% complications , penetration, or spastic pyloric Pathology: stenosis Site gastric , duodenal (Kissing ulcers) Size Single or multiple *- Complications as bleeding (hematemesis, or Shape Edge Floor Base melena, hematochasia?? ), penetration (pancreatitis), perforation (peritonitis), or ?10% pyloric obstruction. -

Peptic Ulcers and Their Complications
OESOPHAGUS AND STOMACH non-steroidal anti-inflammatory drugs (NSAIDS) and infection Peptic ulcers and their with Helicobacter pylori play by far the biggest roles. The reporting of the Campylobacter-like organism H. pylori, complications by Warren and Marshall in 19843 marked a giant leap in medical understanding of peptic ulceration. This Gram-negative, helical, Duncan J Stewart microaerophilic, flagellated bacterium has since been recognized Roger Ackroyd to be responsible for up to 95% of duodenal and 70% of gastric ulcers.4 Furthermore, it is present in up to 10% of patients with dyspepsia without ulceration. Infection with H. pylori is wide- spread and probably acquired in childhood via the faecaleoral Abstract route, although this is yet to be confirmed. In addition, socio- The incidence and management of peptic ulcer disease have changed economic status appears to be inversely related to the prevalence considerably since the first surgical interventions, carried out less than of infection.5 H. pylori colonizes only gastric mucosa, predomi- a century ago. Operative techniques refined during the early second nantly in the antrum and pyloric canal. It possesses a urease half of the 20th century have become almost obsolete in today’s practice enzyme which converts urea to ammonia and carbon dioxide, for two principal reasons. Firstly, understanding of the aetiology of the buffering gastric acid in its vicinity facilitating its survival in the disease process has taken a dramatic step forward with the discovery acidic gastric environment. of Helicobacter pylori now known to be associated with 95% of cases There are a number of mechanisms by which H. -

Boerhaave's Syndrome
Boerhaave's Syndrome: The Importance of Early Diagnosis and Treatment JOSEPH J. CURCI, M.D.,* MARC J. HORMAN, M.D.t Boerhaave's syndrome, spontaneous esophageal rupture, is asso- From the Department of Surgery and the Pulmonary Section, ciated with a 70% survival with surgical intervention. Mortality Abington Memorial Hospital, Abington, Pennsylvania and morbidity are increased in direct proportion to the time be- tween diagnosis and appropriate surgical intervention. Sepsis, hypovolemia and shock are the predominant causes of morbidity and mortality in Boerhaave's syndrome. Two cases of Boerhaave's Two recent cases ofspontaneous rupture ofthe esopha- syndrome are presented which were diagnosed rapidly, and gus successfully treated at Abington Memorial Hospital were managed surgically, resulting in survival of the patients. in Abington, Pennsylvania, will be presented along with A review of the literature is also presented with emphasis on a the clinical and roentgenologic methods of diagnosis of spon- review of the recent literature. taneous esophageal rupture. Particular attention is given to the fact that early diagnosis and treatment will unquestionably Case Reports reduce the morbidity of this syndrome. Case 1: H.F., a 49-year-old Caucasian man, was seen in the Emer- gency Room of Abington Memorial Hospital at 5:00 pm after two epi- B AROGENIC rupture of the esophagus, the so-called sodes of vomiting approximately one hour prior to admission. The "Boerhaave Syndrome," is the most serious and second episode was followed by severe epigastric pain radiating to the rapidly lethal perforation of the gastro-intestinal tract.33 midback area and associated with diaphoresis. -
![[ Color Index | Important | Notes | Extra ]](https://docslib.b-cdn.net/cover/2185/color-index-important-notes-extra-3472185.webp)
[ Color Index | Important | Notes | Extra ]
Objectives: ● The surgical anatomy of stomach and duodenum, their blood supply, nerve supply & lymphatics. ● The surgical physiology of gastric motility and secretions. ● Special forms of peptic ulceration. ● Management of uncomplicated peptic ulcer disease. ● Complications of peptic ulceration requiring operative intervention including: ○ Perforation ( perforated ulcers). ○ Acute hemorrhage. ○ Pyloric stenosis. ● Benign Gastric neoplasms. Resources: ● Davidson’s. ● Slides ● Surgical recall. ● Raslan’s notes. ● Current diagnosis and treatment (colored in blue) ● Team 434 Done by: Lama AlZamil & Aljohara Almazroua Sub-leader: Abdullah Alghizzi Leaders: Monerah Alsalouli & Abdulrahman Alsayyari Reviewed by: Ahmad Alyahya [ Color index | Important | Notes | Extra ] [ Editing file | Feedback | Share your notes | Shared notes ] Basic review(anatomy): Doctor said:Stomach & Duodenum anatomy (including its blood supply & their origins) and physiology are included in the examination and you need to cover it(check the MCQ’s in the last page) Stomach subdivided into 5 parts (each part has secretory and nonsecretory function) Part Notes Cardia Site for Barrett's disease Fundus Secretory: parietal cell and Neurogenic: hunger feeling Body Secretory: parietal cell Antrum Site for surgical ulcer treatment: by cutdown the acid secretion (site for gastrin) Even if the ulcer in the duodenum. Pylorus Site for Dumping Syndrome (food goes immediately to SI) Duodenum parts : 25 cm long and subdivided into 4 parts Part Name Level Common site for First Upper 1st LV Ulcer Second Vertical 2nd LV Diverticulum Third Horizontal 3rd LV Superior Mesenteric Artery Syndrome Fourth Ascending 3rd LV - The 1st part of Duodenum: (Relations) - Anteriorly:The quadrate lobe of the liver and the gallbladder . - Posteriorly: The lesser sac (first inch only), the gastroduodenal artery ( that’s why Posterior ulcer bleed), the bile duct and portal vein, and the inferior vena.