Dermatologic Emergencies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cervical Schwannoma: Report of Four Cases
25-Cervical_3-PRIMARY.qxd 7/10/12 5:22 PM Page 345 CASE REPORT Cervical Schwannoma: Report of Four Cases Rohaizam Jaafar, MD (UKM), Tang Ing Ping, MS ORL-HNS (UM), Doris Evelyn Jong Yah Hui, MS ORL-HNS (UKM), Tan Tee Yong, MS ORL-HNS (UM), Mohammad Zulkarnaen Ahmad Narihan, MPATH (UKM) School of Health Sciences, Health Campus, Hospital Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia. SUMMARY Physical examination revealed a 3 x 3 cm mass located at Extracranial schwannomas in the head and neck region are right lateral upper third of the cervical region. The mass was rare neoplasms. The tumours often present as asymptomatic, firm, mobile and non-tender. She had a right facial nerve slowly enlarging lateral neck masses and determination of palsy (House-Brackman Grade IV) due to a previous operation the nerve origin is not often made until the time of surgery. for a right acoustic neuroma in 2000 and a right supraorbital Preoperative diagnosis maybe aided by imaging studies such wound for a plexiform schwannoma in 2007. as magnetic resonance imaging or computed tomography, while open biopsy is no longer recommended. The accepted A computed tomography of the neck and thorax was treatment for these tumors is surgical resection with performed and showed a well defined, minimally enhancing preservation of the neural pathway. We report four cases of lesion at the left parapharyngeal space measuring 2.4 x 4.3 x cervical schwannomas that we encountered at our center 10 cm. The left carotid sheath vessel is displaced medially. during four years of period. -

Case Report Head and Neck Schwannomas: a Surgical Challenge—A Series of 5 Cases
Hindawi Case Reports in Otolaryngology Volume 2018, Article ID 4074905, 10 pages https://doi.org/10.1155/2018/4074905 Case Report Head and Neck Schwannomas: A Surgical Challenge—A Series of 5 Cases Ishtyaque Ansari,1 Ashfaque Ansari,2 Arjun Antony Graison ,2 Anuradha J. Patil,3 and Hitendra Joshi2 1Department of Neurosurgery, MGM Medical College & Hospital, Aurangabad, India 2Department of ENT, MGM Medical College & Hospital, Aurangabad, India 3Department of Plastic Surgery, MGM Medical College & Hospital, Aurangabad, India Correspondence should be addressed to Arjun Antony Graison; [email protected] Received 25 September 2017; Accepted 29 January 2018; Published 4 March 2018 Academic Editor: Abrão Rapoport Copyright © 2018 Ishtyaque Ansari et al. +is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Schwannomas, also known as neurilemmomas, are benign peripheral nerve sheath tumors. +ey originate from any nerve covered with schwann cell sheath. Schwannomas constitute 25–45% of tumors of the head and neck. About 4% of head and neck schwannomas present as a sinonasal schwannoma. Brachial plexus schwannoma constitute only about 5% of schwannomas. Cervical vagal schwannomas constitute about 2–5% of neurogenic tumors. Methods. We present a case series of 5 patients of schwannomas, one arising from the maxillary branch of trigeminal nerve in the maxillary sinus, second arising from the brachial plexus, third arising from the cervical vagus, and two arising from cervical spinal nerves. Result. Complete extracapsular excision of the tumors was achieved by microneurosurgical technique with preservation of nerve of origin in all except one. -

Tumors of the Brachial Plexus (XI-1)
E. LOCAL SYNDROMES OF THE UPPER LIMBS AND RELATIVELY GENERALIZED SYNDROMES OF THE UPPER AND LOWER LIMBS GROUP XI: PAIN IN THE SHOULDER, ARM, AND HAND Tumors of the Brachial Plexus (XI-1) Definition Progressive aching, burning pain with paresthesias and sensory and motor impairment in the distribution of a branch or branches of the brachial plexus due to tumor. Site Shoulder and upper limb. System Nervous system. Tumors Benign tumors: schwannoma, neurofibroma. Malignant tumors: malignant schwannoma and fibrosarcoma, metastatic neoplasm or direct invasion from other lesion, neuroblastoma, ganglioneuroma (secondary neoplasia of peripheral nerves occurs frequently in lymphoma, leukemia, multiple myeloma). Breast, lung and thyroid neoplasia frequently involve the brachial plexus. Main Features Incidence: the specific tumors of peripheral nerve are extremely rare. Sex Ratio: there is no sex predilection. Age of Onset: young adulthood. They are more common with von Recklinghausen’s disease. Pain Quality: the pain tends to be constant, gradual in onset, aching, and burning, and associated with paresthesias in the distribution of the pain, progressive wasting of muscles depending upon what groups are involved, and sensory loss. Intensity: severe. Associated Symptoms The pain is generally not affected by activity. There is associated sensory loss and muscle wasting depending upon the area of the brachial plexus involved. Pain relief is often not adequate, even with significant narcotics. Signs and Laboratory Findings The laboratory findings are those of the underlying disease. Signs are loss of reflexes, sensation, and muscle strength in the distribution of the involved portion of the plexus. There may be a local mass. The diagnosis is usually made promptly by X-ray or by CT scan. -

Dermatologic Manifestations and Complications of COVID-19
American Journal of Emergency Medicine 38 (2020) 1715–1721 Contents lists available at ScienceDirect American Journal of Emergency Medicine journal homepage: www.elsevier.com/locate/ajem Dermatologic manifestations and complications of COVID-19 Michael Gottlieb, MD a,⁎,BritLong,MDb a Department of Emergency Medicine, Rush University Medical Center, United States of America b Department of Emergency Medicine, Brooke Army Medical Center, United States of America article info abstract Article history: The novel coronavirus disease of 2019 (COVID-19) is associated with significant morbidity and mortality. While Received 9 May 2020 much of the focus has been on the cardiac and pulmonary complications, there are several important dermato- Accepted 3 June 2020 logic components that clinicians must be aware of. Available online xxxx Objective: This brief report summarizes the dermatologic manifestations and complications associated with COVID-19 with an emphasis on Emergency Medicine clinicians. Keywords: COVID-19 Discussion: Dermatologic manifestations of COVID-19 are increasingly recognized within the literature. The pri- fi SARS-CoV-2 mary etiologies include vasculitis versus direct viral involvement. There are several types of skin ndings de- Coronavirus scribed in association with COVID-19. These include maculopapular rashes, urticaria, vesicles, petechiae, Dermatology purpura, chilblains, livedo racemosa, and distal limb ischemia. While most of these dermatologic findings are Skin self-resolving, they can help increase one's suspicion for COVID-19. Emergency medicine Conclusion: It is important to be aware of the dermatologic manifestations and complications of COVID-19. Knowledge of the components is important to help identify potential COVID-19 patients and properly treat complications. © 2020 Elsevier Inc. -

Sciatic Neuropathy from a Giant Hibernoma of the Thigh: a Case Report
A Case Report & Literature Review Sciatic Neuropathy From a Giant Hibernoma of the Thigh: A Case Report Salim Ersozlu, MD, Orcun Sahin, MD, Ahmet Fevzi Ozgur, MD, and Tolga Akkaya, MD ibernomas—rare, uniformly benign soft-tissue the gastrocnemius/soleus, posterior tibialis, and toe flexors tumors of brown fat—were originally described (tibial nerve-innervated muscles); and sensory abnormali- in 1906 by Merkel.1 These tumors are usually ties throughout the entire sciatic nerve distribution. The found in the scapular2 and posterior cervical common peroneal, posterior tibial, superficial peroneal, Hregions or (more rarely) in the folds of the buttocks or on and sural nerves were electrodiagnostically evaluated, and the thigh.3-5 reduced amplitude in the peroneal and the tibialis poste- Sciatic neuropathy is an infrequently diagnosed focal rior nerves was detected. Sensory nerve conduction of the mononeuropathy. Few case reports of lipomas compressing superficial peroneal and sural nerves in the left leg was the sciatic nerve or its peripheral branches have appeared in less than that in the right leg. These findings confirmed the literature.6-8 The present case report is to our knowledge active motor and sensory sciatic mononeuropathy of the the first on sciatic nerve palsy caused by a hibernoma. left leg. Plain x-rays of the left leg showed a large soft-tissue CASE REPORT mass without calcification. Magnetic resonance imaging A woman in her early 30s was referred to our clinic with a (MRI) of the left leg revealed a well-circumscribed large painless left-side posterior thigh mass that had been slowly soft-tissue mass that was 27 cm at its maximum dimen- enlarging over 5 years. -

A Rare Syndrome with Alemtuzumab, Review of Monitoring Protocol
Open Access Case Report DOI: 10.7759/cureus.5715 Idiopathic Thrombocytopenic Purpura: A Rare Syndrome with Alemtuzumab, Review of Monitoring Protocol Deepika Sarvepalli 1 , Mamoon Ur Rashid 2 , Waqas Ullah 3 , Yousaf Zafar 4 , Muzammil Khan 5 1. Internal Medicine, Guntur Medical College, Guntur, IND 2. Internal Medicine, AdventHealth, Orlando, USA 3. Internal Medicine, Abington Hospital - Jefferson Health, Abington, USA 4. Internal Medicine, University of Missouri - Kansas City School of Medicine, Kansas City, USA 5. Internal Medicine, Khyber Teaching Hospital, Peshawar, PAK Corresponding author: Deepika Sarvepalli, [email protected] Abstract Alemtuzumab, a humanized monoclonal antibody that targets surface molecule CD52, causes rapid and complete depletion of circulating T- and B-lymphocytes through antibody-dependent cell-mediated and complement-mediated cytotoxicity. Alemtuzumab has demonstrated superior efficacy compared to subcutaneous interferon beta-1a (SC IFNB-1a) in patients with multiple sclerosis (MS). Alemtuzumab treatment causes a rare and distinct form of secondary immune thrombocytopenic purpura (ITP), characterized by delayed onset, responsiveness to conventional therapies, and prolonged remission following treatment. In phase two and three clinical trials, the incidence of ITP was higher with alemtuzumab treatment compared to the patients receiving SC IFNB-1a. Here we report a case of ITP occurring two years after the first treatment with alemtuzumab. The patient recovered completely after a timely diagnosis -

Numb Chin Sydrome : a Subtle Clinical Condition with Varied Etiology
OLGU SUNUMU / CASE REPORT Gülhane Tıp Derg 2015;57: 324 - 327 © Gülhane Askeri Tıp Akademisi 2015 doi: 10.5455/gulhane.44276 Numb chin sydrome : A subtle clinical condition with varied etiology Devika SHETTY (*), Prashanth SHENAI (**), Laxmikanth CHATRA (**), KM VEENA (**), Prasanna Kumar RAO (**), Rachana V PRABHU (**), Tashika KUSHRAJ (**) SUMMARY Introduction One of the rare neurologic symptoms characterized by hypoesthesia or Numb Chin Syndrome (NCS) is a sensory neuropathy cha- paresthesia of the chin and the lower lip, limited to the region served by the mental nerve is known as Numb chin syndrome. Vast etiologic factors have been racterized by altered sensation and numbness in the distribu- implicated in the genesis of numb chin syndrome. Dental, systemic and malignant tion of the mental nerve, a terminal branch of the mandibular etiologies have been well documented. We present a case of a 59 year old female patient who reported with all the classical features of numb chin syndrome. On division of trigeminal nerve. Any dysfunction along the course magnetic resonance imaging, the vascular compression of the trigeminal nerve of trigeminal nerve and its branches, intracranially and ext- root was evident which has been infrequently documented to be associated with racranially either by direct injury or compression of the nerve the condition. We have also briefly reviewed the etiology and pathogenesis of 1 numb chin syndrome and also stressed on the importance of magnetic resonance can predispose to NCS. Various etiologic factors have been imaging as an investigative modality in diagnosing the condition. considered of which dental procedures and dental pathologies Key Words: Numb Chin Syndrome, Mental nerve neuropathy, trigeminal nerve root, are the most common benign causes. -

Bruise, Contusion & Ecchymosis Conventions
Bruise, Contusion and Ecchymosis MedDRA Proactivity Proposal Implementation MedDRA Version 16.0 I. MSSO Recognized Definitions of Concepts and Terms The MSSO has designated Dorland’s Illustrated Medical Dictionary as the standard reference for medical definitions. The following definitions are cited from Dorland’s 27th edition: Bruise – A superficial injury produced by impact without laceration; a contusion Contusion – A bruise; an injury of a part without a break in the skin Ecchymosis – A small hemorrhagic spot, larger than a petechia, in the skin or mucous membrane forming a nonelevated, rounded or irregular, blue or purplish patch. Hematoma – A localized collection of blood, usually clotted, in an organ, space, or tissue, due to a break in the wall of a blood vessel. Hemorrhage – The escape of blood from the vessels; bleeding. Petechia – A pinpoint, non-raised, perfectly round, purplish red spot caused by intradermal or submucous hemorrhage. Additional comments regarding the definitions: Bruise and contusion are synonymous, and are often used in a colloquial context. Bruise and contusion are each considered a result of injury. Bruise and contusion have been used to describe minor hemorrhage within tissue, where traumatized blood vessels leak blood into the interstitial space. Commonly, capillaries and sometimes venules are injured within skin, subcutaneous tissue, muscle, or bone. In addition to trauma, the terms bruise, ecchymosis, and to a lesser extent, contusion, have also been used as clinical signs of disorders of platelet function, coagulopathies, venous congestion, allergic reactions, etc. Hemorrhage may be used to describe blood escaping from vessels and retained in the interstitial space, and perhaps more commonly, to describe the escape of blood from vessels, and flowing freely external to the tissues. -

COVID-19 Vaccine (Vero Cell), Inactivated (Sinopharm) Manufacturer: Beijing Institute of Biological Products Co., Ltd
COVID-19 Vaccine Explainer 24 MAY 20211 COVID-19 Vaccine (Vero Cell), Inactivated (Sinopharm) Manufacturer: Beijing Institute of Biological Products Co., Ltd The SARS-CoV-2 Vaccine (VeroCell) is an inactivated vaccine against coronavirus disease 2019 (COVID-19) which stimulates the body’s immune system without risk of causing disease. Once inactivated viruses get presented to the body’s immune system, they stimulate the production of antibodies and make the body ready to respond to an infection with live SARS-CoV-2. This vaccine is adjuvanted (with aluminum hydroxide), to boost the response of the immune system. A large multi-country phase 3 trial has shown that two doses administered at an interval of 21 days had the efficacy of 79% against symptomatic SARS-CoV-2 infection 14 days or more after the second dose. The trial was not designed and powered to demonstrate efficacy against severe disease. Vaccine efficacy against hospitalization was 79%. The median duration of follow up available at the time of review was 112 days. Two efficacy trials are underway. The data reviewed at this time support the conclusion that the known and potential benefits of Sinopharm vaccine outweigh the known and potential risks. Date of WHO Emergency Use Listing (EUL) recommendation: 7 May 2021 Date of prequalification (PQ): currently no information National regulatory authorities (NRAs) can use reliance approaches for in-country authorization of vaccines based on WHO PQ/EUL or emergency use authorizations by stringent regulatory authorities (SRAs). Product characteristics Presentation Fully liquid, inactivated, adjuvanted, preservative-free suspension in vials and AD pre-filled syringes Number of doses Single-dose (one dose 0.5 mL) Vaccine syringe type Two available presentations: and needle size 1. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Measles Clinical Guidance: Identification & Testing of Suspect Measles Cases
June 2019 Measles Clinical Guidance: Identification & Testing of Suspect Measles Cases The United States declared measles eliminated in 2000, meaning that there is not endemic transmission within the country and reported cases are due to infection while visiting another country. Measles continues to circulate in much of the world, including Europe, Asia and Africa. International travel, domestic travel through international airports, and contact with international visitors can pose a risk for exposure to measles. When measles is imported into the United States, additional transmission can occur locally. While providers should consider measles in patients with fever and a descending rash, measles is unlikely in the absence of confirmed measles cases in your community or a history of travel or exposure to travelers. This guidance discusses which patients should be prioritized for measles testing. Testing for measles should be based on: A) Measles symptoms: • Fever, including subjective fever. • Rash that starts on the head and descends. • Usually 1 or 2 of the 3 “Cs” – cough, coryza and conjunctivitis. B) Risk factors increasing the likelihood of a measles diagnosis: • In the prior 3 weeks: travel outside of North America, transit through U.S. international airports, or interaction with foreign visitors, including at a U.S. tourist attraction. • Confirmed measles cases in your community. • Never immunized with measles vaccine and born in 1957 or later. NOTE: Fever and rash occur in approximately 5% of MMR vaccine recipients, typically 6-12 days after immunization. Such reactions can be clinically identical to measles infection, and result in positive laboratory testing for measles. This reflects an immune response due to exposure to measles vaccine virus rather than wild measles virus and the patient is not infectious. -
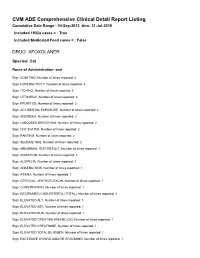
FDA CVM Comprehensive ADE Report Listing for Afoxolaner
CVM ADE Comprehensive Clinical Detail Report Listing Cumulative Date Range : 04-Sep-2013 -thru- 31-Jul-2018 Included 1932a cases = : True Included Medicated Feed cases = : False DRUG: AFOXOLANER Species: Cat Route of Administration: oral Sign: VOMITING, Number of times reported: 4 Sign: HYPERACTIVITY, Number of times reported: 3 Sign: ITCHING, Number of times reported: 3 Sign: LETHARGY, Number of times reported: 3 Sign: PRURITUS, Number of times reported: 3 Sign: ACCIDENTAL EXPOSURE, Number of times reported: 2 Sign: ANOREXIA, Number of times reported: 2 Sign: LABOURED BREATHING, Number of times reported: 2 Sign: NOT EATING, Number of times reported: 2 Sign: PANTING, Number of times reported: 2 Sign: SEIZURE NOS, Number of times reported: 2 Sign: ABNORMAL TEST RESULT, Number of times reported: 1 Sign: AGITATION, Number of times reported: 1 Sign: ALOPECIA, Number of times reported: 1 Sign: ANAEMIA NOS, Number of times reported: 1 Sign: ATAXIA, Number of times reported: 1 Sign: CERVICAL VENTROFLEXION, Number of times reported: 1 Sign: CONSTIPATION, Number of times reported: 1 Sign: DECREASED CHOLESTEROL (TOTAL), Number of times reported: 1 Sign: ELEVATED ALT, Number of times reported: 1 Sign: ELEVATED AST, Number of times reported: 1 Sign: ELEVATED BUN, Number of times reported: 1 Sign: ELEVATED CREATINE-KINASE (CK), Number of times reported: 1 Sign: ELEVATED CREATININE, Number of times reported: 1 Sign: ELEVATED TOTAL BILIRUBIN, Number of times reported: 1 Sign: EXCESSIVE LICKING AND/OR GROOMING, Number of times reported: 1 Sign: FEVER,