Sleep Medicine a Special Report June 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 De Juan Et Al
US 200601 10428A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 de Juan et al. (43) Pub. Date: May 25, 2006 (54) METHODS AND DEVICES FOR THE Publication Classification TREATMENT OF OCULAR CONDITIONS (51) Int. Cl. (76) Inventors: Eugene de Juan, LaCanada, CA (US); A6F 2/00 (2006.01) Signe E. Varner, Los Angeles, CA (52) U.S. Cl. .............................................................. 424/427 (US); Laurie R. Lawin, New Brighton, MN (US) (57) ABSTRACT Correspondence Address: Featured is a method for instilling one or more bioactive SCOTT PRIBNOW agents into ocular tissue within an eye of a patient for the Kagan Binder, PLLC treatment of an ocular condition, the method comprising Suite 200 concurrently using at least two of the following bioactive 221 Main Street North agent delivery methods (A)-(C): Stillwater, MN 55082 (US) (A) implanting a Sustained release delivery device com (21) Appl. No.: 11/175,850 prising one or more bioactive agents in a posterior region of the eye so that it delivers the one or more (22) Filed: Jul. 5, 2005 bioactive agents into the vitreous humor of the eye; (B) instilling (e.g., injecting or implanting) one or more Related U.S. Application Data bioactive agents Subretinally; and (60) Provisional application No. 60/585,236, filed on Jul. (C) instilling (e.g., injecting or delivering by ocular ion 2, 2004. Provisional application No. 60/669,701, filed tophoresis) one or more bioactive agents into the Vit on Apr. 8, 2005. reous humor of the eye. Patent Application Publication May 25, 2006 Sheet 1 of 22 US 2006/0110428A1 R 2 2 C.6 Fig. -

Tactics of Family Doctors in Case of Syncopal States
MINISTRY OF PUBLIC HEALTH OF UKRAINE ZAPORIZHZHIA STATE MEDICAL UNIVERSITY DEPARTMENT OF GENERAL PRACTICE – FAMILY MEDICINE AND INTERNAL DISEASES DEPARTMENT OF GENERAL PRACTICE – FAMILY MEDICINE, THERAPY, CARDIOLOGY AND NEUROLOGY OF THE POSTGRADUATE FACULTY TACTICS OF FAMILY DOCTORS IN CASE OF SYNCOPAL STATES STUDY GUIDE for the students of the specialty "Medicine" in the program of the educational discipline "General Practice - Family Medicine" Zaporizhzhia 2020 2 UDC 616.8-009.832-08(072) М 99 Аpproved by Central Methodical Council of Zaporizhzhia State Medical University as а study guide (Protocol № 3 of 27.02.2020) and recommended for use in the educational process Authors: N. S. Mykhailovska - Doctor of Medical Sciences, Professor, head of the Department of General practice – family medicine and internal diseases, Zaporizhzhia State Medical University; A. V. Grytsay - PhD, associated professor of the Department of General practice – family medicine and internal diseases, Zaporizhzhia State Medical University; І. S. Kachan - associated professor of the Department of Family medicine, therapy, cardiology and neurology of the Postgraduate faculty, Zaporizhzhia State Medical University. Readers: S. Y. Dotsenko – Doctor of Medical Sciences, Professor, Head of the Internal Medicine №3 Department, Zaporozhye State Medical University; S. M. Kiselev – Doctor of Medical Sciences, Professor, Professor of the Department of Internal diseases 1, Zaporizhzhia State Medical University. Mykhailovska N. S. M99 Tactics of family doctors in case of syncopal states = Тактика сімейного лікаря при синкопальних станах: study guide for the practical classes and individual work for 6th-years students of international faculty (speciality «General medicine»), discipline «General practice – family medicine» / N. S. Mykhailovska, A. V. Grytsay, I.S. -

List of Union Reference Dates A
Active substance name (INN) EU DLP BfArM / BAH DLP yearly PSUR 6-month-PSUR yearly PSUR bis DLP (List of Union PSUR Submission Reference Dates and Frequency (List of Union Frequency of Reference Dates and submission of Periodic Frequency of submission of Safety Update Reports, Periodic Safety Update 30 Nov. 2012) Reports, 30 Nov. -

211230Orig1s000 211230Orig2s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 211230Orig1s000 211230Orig2s000 RISK ASSESSMENT and RISK MITIGATION REVIEW(S) Division of Risk Management (DRISK) Office of Medication Error Prevention and Risk Management (OMEPRM) Office of Surveillance and Epidemiology (OSE) Center for Drug Evaluation and Research (CDER) Application Type NDA Application Number 211230 PDUFA Goal Date December 20, 2018 OSE RCM # 2018‐1313 Reviewer Name(s) Naomi Redd, Pharm.D. Team Leader Elizabeth Everhart, RN, MSN, ACNP Division Director Cynthia LaCivita, Pharm.D. Review Completion Date September 25, 2018 Subject Evaluation of the Need for a REMS Established Name Solriamfetol Trade Name Sunosi Name of Applicant Jazz Pharmaceuticals Therapeutic class Dopamine and Norepinephrine Reuptake Inhibitor (DNRI) Formulation 75 mg, 150 mg (b) (4) oral tablets Dosing Regimen Take one tablet once daily upon awakening 1 Reference ID: 4327439 Table of Contents EXECUTIVE SUMMARY ......................................................................................................................................................... 3 1 Introduction ..................................................................................................................................................................... 3 2 Background ...................................................................................................................................................................... 3 2.1 Product Information .......................................................................................................................................... -

Misuse of Drugs Act 1975
Reprint as at 1 July 2014 Misuse of Drugs Act 1975 Public Act 1975 No 116 Date of assent 10 October 1975 Commencement see section 1(2) Contents Page Title 4 1 Short Title and commencement 4 2 Interpretation 4 3 Act to bind the Crown 9 3A Classification of drugs 9 4 Amendment of schedules that identify controlled drugs 10 and precursor substances, and set amount, level, or quantity at and over which controlled drugs are presumed to be for supply 4A Procedure for bringing Order in Council made under 12 section 4(1) or (1B) into force 4B Matters to which Minister must have regard before 13 recommending Order in Council under section 4(1) or (1B) 4C Temporary class drug notice [Repealed] 14 4D Effect of temporary class drug notice [Repealed] 15 4E Duration of temporary class drug notice [Repealed] 15 Note Changes authorised by subpart 2 of Part 2 of the Legislation Act 2012 have been made in this official reprint. Note 4 at the end of this reprint provides a list of the amendments incorporated. This Act is administered by the Ministry of Health. 1 Reprinted as at Misuse of Drugs Act 1975 1 July 2014 5 Advisory and technical committees 15 5AA Expert Advisory Committee on Drugs 15 5A Approved laboratories 17 5B Functions of Minister 17 6 Dealing with controlled drugs 18 7 Possession and use of controlled drugs 20 8 Exemptions from sections 6 and 7 22 9 Cultivation of prohibited plants 26 10 Aiding offences against corresponding law of another 27 country 11 Theft, etc, of controlled drugs 28 12 Use of premises or vehicle, etc 29 12A Equipment, -

Nonpeptide Orexin Type-2 Receptor Agonist Ameliorates Narcolepsy-Cataplexy Symptoms in Mouse Models
Nonpeptide orexin type-2 receptor agonist ameliorates narcolepsy-cataplexy symptoms in mouse models Yoko Irukayama-Tomobea,1, Yasuhiro Ogawaa,1, Hiromu Tominagaa,1, Yukiko Ishikawaa, Naoto Hosokawaa, Shinobu Ambaia, Yuki Kawabea, Shuntaro Uchidaa, Ryo Nakajimaa, Tsuyoshi Saitoha, Takeshi Kandaa, Kaspar Vogta, Takeshi Sakuraia, Hiroshi Nagasea, and Masashi Yanagisawaa,2 aInternational Institute for Integrative Sleep Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8575, Japan Contributed by Masashi Yanagisawa, March 22, 2017 (sent for review January 13, 2017; reviewed by Thomas S. Kilduff and Thomas E. Scammell) Narcolepsy-cataplexy is a debilitating disorder of sleep/wakefulness methylphenidate and modafinil), sedative (sodium oxybate), and caused by a loss of orexin-producing neurons in the lateroposterior tricyclic antidepressants. However, the use of these medications is hypothalamus. Genetic or pharmacologic orexin replacement ame- often limited by adverse side effects such as headache, nausea, liorates symptoms in mouse models of narcolepsy-cataplexy. We anxiety, irritability, and insomnia. have recently discovered a potent, nonpeptide OX2R-selective Murine models of narcolepsy-cataplexy include OXKO mice − − − − agonist, YNT-185. This study validates the pharmacological activity (2), orexin receptor-deficient (Hcrtr1 / ;Hcrtr2 / , abbreviated as of this compound in OX2R-transfected cells and in OX2R-expressing OXRDKO) mice, and the orexin/ataxin-3 transgenic mice (in neurons in brain slice preparations. Intraperitoneal, and intracere- which orexin neurons are genetically and postnatally ablated) broventricular, administration of YNT-185 suppressed cataplexy-like (12). Tabuchi et al. created another narcolepsy mouse model, episodes in orexin knockout and orexin neuron-ablated mice, but not which expressed diphtheria toxin A in orexin neurons under in orexin receptor-deficient mice. -

Unarousable Unresponsiveness in Which the Patient Lies with the Eye Closed and Has No Awareness of Self and Surroundings (2)
Neurological Disease Deborah M Stein, MD, MPH 1. Coma a. Coma is defined as “a state of extreme unresponsiveness, in which an individual exhibits no voluntary movement or behavior” (1). i. Alternatively, coma is a state of unarousable unresponsiveness in which the patient lies with the eye closed and has no awareness of self and surroundings (2). b. Coma lies on a spectrum with other alterations in consciousness – from confusion to delirium to obtundation to stupor to coma and, ultimately, brain death (2). c. To be clearly distinguished from syncope, concussion, or other states of transient unconsciousness coma must persist for at least one hour (2). d. There are 2 important characteristics of the conscious state (3) i. The level of consciousness – “arousal or wakefulness” 1. Regulated by physiological functioning and consists of more primitive responsiveness to the world such as predictable involuntary reflex responses to stimuli. 2. Arousal is maintained by the reticular activating system (RAS) - a network of structures (including the brainstem, the medulla, and the thalamus) ii. The content of consciousness – “awareness” 1. Regulated by cortical areas within the cerebral hemispheres, e. There are two main causes for coma: i. Bihemispheric diffuse cortical or white matter damage or ii. Brainstem lesions bilaterally affecting the subcortical reticular activating systems. f. A huge number of conditions can result in coma. One way to categorize these conditions is to divide them into the anatomic and the metabolic causes of coma. i. Anatomic causes of coma are those conditions that disrupt the normal physical architecture and anatomy, either at the level of the cerebral cortex or the brainstem ii. -

Heat Illness & Hydration
Sideline Emergencies: Exertional Heat Illness- Prevention and Treatment Updates AOSSM: 2019 Sports Medicine & Football - Youth to the NFL Damion A. Martins, MD Medical Director of Sports Medicine Sports Medicine Fellowship Program Director, Atlantic Health Systems Director of Internal Medicine, New York Jets DISCLOSURE Neither I, (Damion Martins, MD), nor any family member(s), author(s), have any relevant financial relationships to be discussed, directly or indirectly, referred to or illustrated with or without recognition within the presentation. Learning Objectives Describe the pathophysiology of Exertional Heat Illness Identify signs and symptoms of Exertional Heat Stroke Understand urgent on the field management and treatment of Heat Illness Understand current evidence for prevention and treatment of Exertional Heat Stroke Overview Heat Illness – Diagnosis – Pathophysiology – Risk Factors – Evaluation / Treatment Hydration – NCAA / NFL data – IV vs PO data McNair video 6 Physiology Thermoregulation Production Dissipation – – basal metabolism conduction – – exercise radiation – convection – evaporation Sandor RP. Phys SportsMed. 1997;25(6):35-40. Heat Illness Spectrum Heat Illness Heat Injury Heat Stroke Definitions Exertional Heat Illness (EHI) Heat edema – initial days of heat exposure – self-limited, mild swelling of hands / feet Heat cramps or Exercise Associated Muscle Cramps (EAMCs) – skeletal muscle cramping during or after exercise – usually abdominal and extremities Heat syncope – orthostatic dizziness or sudden -
Neurologic Manifestations of Hypoglycemia
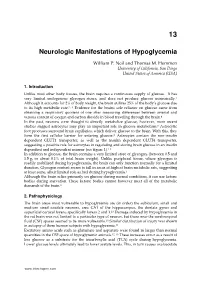
13 Neurologic Manifestations of Hypoglycemia William P. Neil and Thomas M. Hemmen University of California, San Diego United States of America (USA) 1. Introduction Unlike most other body tissues, the brain requires a continuous supply of glucose. It has very limited endogenous glycogen stores, and does not produce glucose intrinsically.1 Although it accounts for 2% of body weight, the brain utilizes 25% of the body’s glucose due to its high metabolic rate.2, 3 Evidence for the brains sole reliance on glucose came from obtaining a respiratory quotient of one after measuring differences between arterial and venous content of oxygen and carbon dioxide in blood traveling through the brain.4 In the past, neurons were thought to directly metabolize glucose, however, more recent studies suggest astrocytes may play an important role in glucose metabolism.5 Astrocytic foot processes surround brain capillaries, which deliver glucose to the brain. With this, they form the first cellular barrier for entering glucose.5 Astrocytes contain the non-insulin dependent GLUT1 transporter, as well as the insulin dependent GLUT4 transporter, suggesting a possible role for astrocytes in regulating and storing brain glucose in an insulin dependent and independent manner (see figure 1).6-8 In addition to glucose, the brain contains a very limited store of glycogen, (between 0.5 and 1.5 g, or about 0.1% of total brain weight). Unlike peripheral tissue, where glycogen is readily mobilized during hypoglycemia, the brain can only function normally for a limited duration. Glycogen content seems to fall in areas of highest brain metabolic rate, suggesting at least some, albeit limited role as fuel during hypoglycemia.7 Although the brain relies primarily on glucose during normal conditions, it can use ketone bodies during starvation. -

Public Comment 8
www.JazzPharmaceuticals.com May 20, 2021 Priya Shah West Virginia Medicaid 350 Capitol Street, Room 251 Charleston WV 25301 Dear Priya Shah, Thank you for your request for information regarding XYWAV™ (calcium, magnesium, potassium, and sodium oxybates) oral solution. If you did not specifically request the enclosed information, please contact Jazz Medical Information at 1-800-520-5568. XYWAV is indicated for the treatment of cataplexy or excessive daytime sleepiness (EDS) in patients 7 years of age and older with narcolepsy. Below is the information you requested. • XYWAV (calcium, magnesium, potassium, and sodium oxybates) Oral Solution Written Comments for Medicaid • XYWAV Prescribing Information Please refer to the accompanying XYWAV™ full Prescribing Information including the Boxed Warning. This information is provided to you as a professional courtesy and may include content that has not been approved by the United States Food and Drug Administration (FDA). Statements in this communication are not intended to advocate any indication, dosage, or other claim not set forth in the prescribing information. This response contains information of a general nature and is intended solely to assist you in formulating your own conclusions regarding our product. It is not meant to be a thorough review of the literature and does not represent all professional points of view on this subject. Thank you for your interest in XYWAV™. Please contact Medical Information at 1-800-520-5568 if you have further questions. Sincerely, Jazz Pharmaceuticals -

Les Perspectives Dans La Prise En Charge Thérapeutique De L'alcoolo
Les perspectives dans la prise en charge thérapeutique de l’alcoolo-dépendance Leslie Bellec To cite this version: Leslie Bellec. Les perspectives dans la prise en charge thérapeutique de l’alcoolo-dépendance. Sciences du Vivant [q-bio]. 2016. dumas-01758776 HAL Id: dumas-01758776 https://dumas.ccsd.cnrs.fr/dumas-01758776 Submitted on 5 Jun 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. N° d'ordre : ANNÉE 2016 THÈSE D'EXERCICE / UNIVERSITÉ DE RENNES 1 sous le sceau de l’Université Bretagne Loire Thèse en vue du DIPLÔME D'ÉTAT DE DOCTEUR EN PHARMACIE présentée par Leslie Bellec Les perspectives dans la prise Thèse soutenue à Rennes en charge le 22 juin 2016 thérapeutique de devant le jury composé de : Isabelle MOREL l’alcoolo-dépendance Professeur à la faculté de Pharmacie de l’Université de Rennes 1 / président Damien PUISSANT Docteur en Pharmacie, titulaire de la Pharmacie du Pont de Chateaudun à Rennes / examinateur Nicolas MARIE Docteur en Pharmacie, Praticien au Centre Hospitalier Guillaume Régnier à Rennes / directeur de thèse 1 N° d'ordre -

Postconcussional Disorder and Loss of Consciousness
Postconcussional Disorder and Loss of Consciousness Stephen D. Anderson, MD, FRCP(C) Postconcussional disorder (PCD) has been described in the psychiatric, neuro- logical, neuropsychological, and rehabilitation medicine literature for many years. PCD has recently been introduced into DSM-IV, appearing in an appendix that contains a number of proposals for new categories and axes that were suggested for possible inclusion in DSM-IV. There are some major difficulties with the proposed criteria for PCD. This article explores some of these difficulties, partic- ularly focusing on the criteria of loss of consciousness (LOC). A review of the literature demonstrates that LOC is not necessary for PCD to occur. The major difficulty with the DSM-IV criteria is the definition of concussion. The article suggests that, instead, the criteria for mild traumatic brain injury, as defined by the American Congress of Rehabilitation Medicine, may be more appropriate. Postconcussional disorder (PCD) has been symptoms include headache pain, nausea. described in the medical literature for dizziness or vertigo. unsteadiness or poor over a century. The telm Post-concussion coordination, tinnitus, hearing loss. blurred syndrome was coined by Strauss and vision, diplopia, convergence insufficiency. Savitsky in 1934.' PCD is the most preva- light and noise sensitivity, and altered sense lent and yet controversial neuropsychiat~ic of taste and smell. The cognitive deficits diagnosis following brain injury. PCD is include memory difticulties, decreased at- linked most commonly to minor brain in- tention and concentration, decreased speed jury. because the symptoms are unobscured of information processing, communication by the myriad of findings that accompany a difficulties, difficulties with executive fin- more severe brain injuly.