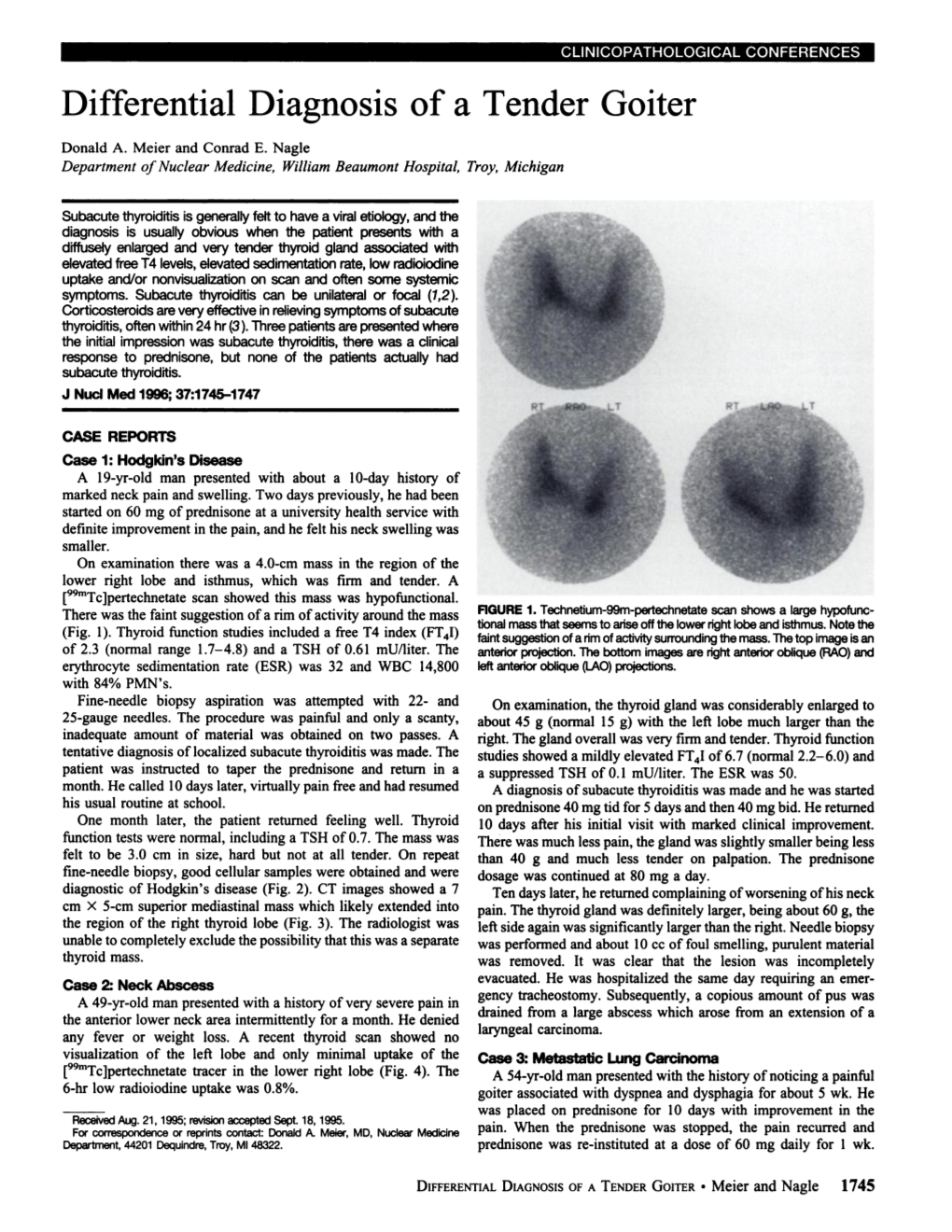
Differential Diagnosis of a Tender Goiter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hashimoto's Thyroiditis
AMERICAN THYROID ASSOCIATION® www.thyroid.org Hashimoto’s Thyroiditis (Lymphocytic Thyroiditis) WHAT IS THE THYROID GLAND? HOW IS THE DIAGNOSIS OF HASHIMOTO’S The thyroid gland is a butterfly-shaped endocrine gland THYROIDITIS MADE? that is normally located in the lower front of the neck. The diagnosis of Hashimoto’s thyroiditis may be made The thyroid’s job is to make thyroid hormones, which are when patients present with symptoms of hypothyroidism, secreted into the blood and then carried to every tissue often accompanied by a goiter (an enlarged thyroid in the body. Thyroid hormones help the body use energy, gland) on physical examination, and laboratory testing of stay warm and keep the brain, heart, muscles, and other hypothyroidism, which is an elevated thyroid stimulating organs working as they should. hormone (TSH) with or without a low thyroid hormone (Free WHAT IS HASHIMOTO’S THYROIDITIS? thyroxine [Free T4]) levels. TPO antibody, when measured, is usually elevated. The term “Thyroiditis” refers to “inflammation of the thyroid gland”. There are many possible causes of thyroiditis (see Occasionally, the disease may be diagnosed early, Thyroiditis brochure). Hashimoto’s thyroiditis, also known especially in people with a strong family history of thyroid as chronic lymphocytic thyroiditis, is the most common disease. TPO antibody may be positive, but thyroid cause of hypothyroidism in the United States. It is an hormone levels may be normal or there may only be autoimmune disorder involving chronic inflammation of isolated mild elevation of serum TSH is seen. Symptoms of the thyroid. This condition tends to run in families. Over hypothyroidism may be absent. -

Thyroiditis: an Integrated Approach LORI B
Thyroiditis: An Integrated Approach LORI B. SWEENEY, MD, Virginia Commonwealth University Health System, Richmond, Virginia CHRISTOPHER STEWART, MD, Bayne-Jones Army Community Hospital, Fort Polk, Louisiana DAVID Y. GAITONDE, MD, Dwight D. Eisenhower Army Medical Center, Fort Gordon, Georgia Thyroiditis is a general term that encompasses several clinical disorders characterized by inflammation of the thyroid gland. The most common is Hashimoto thyroiditis; patients typically present with a nontender goiter, hypothyroid- ism, and an elevated thyroid peroxidase antibody level. Treatment with levothyroxine ameliorates the hypothyroid- ism and may reduce goiter size. Postpartum thyroiditis is transient or persistent thyroid dysfunction that occurs within one year of childbirth, miscarriage, or medical abortion. Release of preformed thyroid hormone into the bloodstream may result in hyperthyroidism. This may be followed by transient or permanent hypothyroidism as a result of depletion of thyroid hormone stores and destruction of thyroid hormone–producing cells. Patients should be monitored for changes in thyroid function. Beta blockers can treat symptoms in the initial hyperthyroid phase; in the subsequent hypothyroid phase, levothyroxine should be considered in women with a serum thyroid-stimulating hormone level greater than 10 mIU per L, or in women with a thyroid-stimulating hormone level of 4 to 10 mIU per L who are symptomatic or desire fertility. Subacute thyroiditis is a transient thyrotoxic state characterized by anterior neck pain, suppressed thyroid-stimulating hormone, and low radioactive iodine uptake on thyroid scanning. Many cases of subacute thyroiditis follow an upper respiratory viral illness, which is thought to trigger an inflammatory destruction of thyroid follicles. In most cases, the thyroid gland spontaneously resumes normal thyroid hormone production after several months. -

Treating Thyroid Disease: a Natural Approach to Healing Hashimoto's
Treating Thyroid Disease: A Natural Approach to Healing Hashimoto’s Melissa Lea-Foster Rietz, FNP-BC, BC-ADM, RYT-200 Presbyterian Medical Services Farmington, NM [email protected] Professional Disclosures I have no personal or professional affiliation with any of the resources listed in this presentation, and will receive no monetary gain or professional advancement from this lecture. Talk Objectives • Define hypothyroidism and Hashimoto’s. • Discuss various tests used to identify thyroid disease and when to treat based on patient symptoms • Discuss potential causes and identify environmental factors that contribute to disease • Describe how the gut (food sensitivities) and the adrenals (chronic stress) are connected to Hashimoto’s and how we as practitioners can work to educate patients on prevention before the need for treatment • How the use of adaptogens can enhance the treatment of Hashimoto’s and identify herbs that are showing promise in the research. • How to use food, exercise, and relaxation to improve patient outcomes. Named for Hakuro Hashimoto, a physician working in Europe in the early 1900’s. Hashimoto’s was the first autoimmune disease to be recognized in the scientific literature. It is estimated that one in five people suffer from an autoimmune disease and the numbers continue to rise. Women are more likely than men to develop an autoimmune disease, and it is believed that 75% of individuals with an autoimmune disease are female. Thyroid autoimmune disease is the most common form, and affects 7-8% of the population in the United States. Case Study Ms. R is a 30-year-old female, mother of three, who states that after the birth of her last child two years ago she has felt the following: • Loss of energy • Difficulty losing weight despite habitual eating pattern • Hair loss • Irregular menses • Joints that ache throughout the day • A general sense of sadness • Cold Intolerance • Joint and Muscle Pain • Constipation • Irregular menstruation • Slowed Heart Rate What tests would you run on Ms. -

Hashimoto Thyroiditis
Hashimoto thyroiditis Description Hashimoto thyroiditis is a condition that affects the function of the thyroid, which is a butterfly-shaped gland in the lower neck. The thyroid makes hormones that help regulate a wide variety of critical body functions. For example, thyroid hormones influence growth and development, body temperature, heart rate, menstrual cycles, and weight. Hashimoto thyroiditis is a form of chronic inflammation that can damage the thyroid, reducing its ability to produce hormones. One of the first signs of Hashimoto thyroiditis is an enlargement of the thyroid called a goiter. Depending on its size, the enlarged thyroid can cause the neck to look swollen and may interfere with breathing and swallowing. As damage to the thyroid continues, the gland can shrink over a period of years and the goiter may eventually disappear. Other signs and symptoms resulting from an underactive thyroid can include excessive tiredness (fatigue), weight gain or difficulty losing weight, hair that is thin and dry, a slow heart rate, joint or muscle pain, and constipation. People with this condition may also have a pale, puffy face and feel cold even when others around them are warm. Affected women can have heavy or irregular menstrual periods and difficulty conceiving a child ( impaired fertility). Difficulty concentrating and depression can also be signs of a shortage of thyroid hormones. Hashimoto thyroiditis usually appears in mid-adulthood, although it can occur earlier or later in life. Its signs and symptoms tend to develop gradually over months or years. Frequency Hashimoto thyroiditis affects 1 to 2 percent of people in the United States. -

Graves' Disease Following the Occurrence of Hypothyroidism
Henry Ford Hospital Medical Journal Volume 28 Number 2 Richmond W. Smith Jr. Testimonial Article 14 Issue 6-1980 Graves' Disease Following the Occurrence of Hypothyroidism A. R. Guansing D. D. Klink N. Engbring Y. Leung J. Chakravarty See next page for additional authors Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons Recommended Citation Guansing, A. R.; Klink, D. D.; Engbring, N.; Leung, Y.; Chakravarty, J.; and Wilson, S. (1980) "Graves' Disease Following the Occurrence of Hypothyroidism," Henry Ford Hospital Medical Journal : Vol. 28 : No. 2 . Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol28/iss2/14 This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons. Graves' Disease Following the Occurrence of Hypothyroidism Authors A. R. Guansing, D. D. Klink, N. Engbring, Y. Leung, J. Chakravarty, and S. Wilson This article is available in Henry Ford Hospital Medical Journal: https://scholarlycommons.henryford.com/ hfhmedjournal/vol28/iss2/14 Henry Ford Hosp Med j Vol 28, No 2 and 3, 1980 Graves' Disease Following the Occurrence of Hypothyroidism A. R. Guansing, MD,* D. D. Klink, MD,* N. Engbring, MD,** Y. Leung, MD,*** J. chakravarty, MD,*** and S. Wilson, MD** Three patients with hypothyroidism of 15-48 months' dura negative antithyroglobulin and antimicrosomal antibody tion developed Graves' disease while on thyroid hormone titers. Two had demonstrable long-acting thyroid stimulator replacement therapy. -

Thyroid Disease
Thyroid Disease Thyroid disease occurs when the thyroid (a small, butterfly-shaped gland in the front of your neck) does not produce the right amount of thyroid hormone. These hormones control how your body uses energy. If you are feeling fatigued, notice skin or hair changes, or have hoarseness or pain, your doctor may conduct a physical exam and order blood tests. If these tests indicate a problem, your doctor may order thyroid scan and uptake, thyroid biopsy, or imaging tests to help diagnose and evaluate a thyroid condition. Treatment will depend on the specific nature of your thyroid condition and its underlying cause. What is thyroid disease? The thyroid is a small, butterfly-shaped gland in the front of your neck that wraps around your windpipe (trachea). The two halves of the thyroid gland are connected in the middle by a thin layer of tissue known as the isthmus. The thyroid gland uses iodine (mostly absorbed from food) to produce hormones that control how your body uses energy. Nearly every organ in the body is affected by the function of the thyroid gland. The pituitary gland and hypothalamus, an area at the base of the brain, control the rate at which the thyroid produces and releases these hormones. The main function of the thyroid gland is to release a hormone called thyroxine or T4, which is converted into a hormone called T3. Both of these hormones circulate in the bloodstream and help regulate your metabolism. The amount of T4 produced by the thyroid gland is determined by a hormone produced by the pituitary gland called TSH or thyroid-stimulating hormone. -
Care Step Pathway – Thyroiditis (Inflammation of the Thyroid Gland)
Care Step Pathway – Thyroiditis (inflammation of the thyroid gland) Assessment Look: Listen: Recognize: - Appear unwell? - Appetite/weight changes? - Other immune-related toxicity? - Changes in weight since last visit? - Hot or cold intolerance? - Prior thyroid dysfunction? o Appear heavier? Thinner? - Change in energy, mood, or behavior? - Prior history of radiation therapy? - Changes in hair texture/thickness? - Palpitations? - Signs of thyroid storm (fever, tachycardia, sweating, dehydration, cardiac - Appear hot/cold? - Increased fatigue? decompensation, delirium/psychosis, liver failure, abdominal pain, - Look fatigued? - Bowel-related changes? nausea/vomiting, diarrhea) - Sweating? Constipation/diarrhea - Hyperactive or lethargic? o - Signs of airway compression - Difficulty breathing? - Shortness of breath/edema? - Clinical presentation: Occasionally thyroiditis with transient hyperthyroidism - Swollen neck? - Skin-related changes? (low TSH and high free T4) may be followed by more longstanding - Voice change (e.g., deeper voice) o Dry/oily hypothyroidism (high TSH and low free T4) - Differential diagnosis-- Primary hypothyroidism: High TSH with low free T4; secondary (central) hypothyroidism due to hypophysitis: both TSH and free T4 are low (see HCP Assessment below for more detail about testing) Grading Toxicity HYPOTHYROIDISM Definition: A disorder characterized by decreased production of thyroid hormones from the thyroid gland Asymptomatic, subclinical Asymptomatic, subclinical Symptomatic, primary Severely symptomatic, Life-threatening, -

Hypothyroidism and Resistance to Thyroid Hormone Panel
Hypothyroidism and Resistance to Thyroid Hormone Panel Test code: EN0701 Is a 22 gene panel that includes assessment of non-coding variants. Is ideal for patients with a clinical suspicion of congenital hypothyroidism or thyroid hormone resistance. About Hypothyroidism and Resistance to Thyroid Hormone Primary congenital hypothyroidism is a permanent thyroid hormone deficiency that is present from birth. About 1 in 5,000 babies is born with congenital hypothyroidism, in which the thyroid fails to grow normally and cannot produce enough hormone. There is no identifiable cause for most cases of congenital hypothyroidism but in 15-20% are caused by an inherited defect in genes that play a role in the proper growth, function and development of the thyroid gland. Primary congenital hypothyroidism may be due to a thyroid dysgenesis where the thyroid gland fails to develop normally or it may occur as a result of an inborn error of thyroid hormone biosynthesis (also known as dyshormonogenesis) or as a result of thyroid- stimulating hormone (TSH) receptor mutations. In iodine sufficient countries, 85% of permanent congenital hypothyroidism is due to thyroid dysgenesis. The remaining 10-15% of cases can be attributed to dyshormonogenesis or to defects in peripheral thyroid hormone transport, metabolism or action. Primary congenital hypothyroidism may also be idiopathic. The prevalence is estimated at 1:2,000-1:4,000. For reasons that remain unclear, congenital hypothyroidism affects more than twice as many females as males. Thyroid dyshormonogenesis results from mutations in one of the several genes involved in the production of thyroid hormones. These genes include DUOX2, SLC5A5, TG, and TPO. -

Management of Hypopituitarism
Journal of Clinical Medicine Review Management of Hypopituitarism Krystallenia I. Alexandraki 1 and Ashley B. Grossman 2,3,* 1 Endocrine Unit, 1st Department of Propaedeutic Medicine, School of Medicine, National and Kapodistrian University of Athens, 115 27 Athens, Greece; [email protected] 2 Department of Endocrinology, Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, University of Oxford, Oxford OX3 7LE, UK 3 Centre for Endocrinology, Barts and the London School of Medicine, London EC1M 6BQ, UK * Correspondence: [email protected] Received: 18 November 2019; Accepted: 2 December 2019; Published: 5 December 2019 Abstract: Hypopituitarism includes all clinical conditions that result in partial or complete failure of the anterior and posterior lobe of the pituitary gland’s ability to secrete hormones. The aim of management is usually to replace the target-hormone of hypothalamo-pituitary-endocrine gland axis with the exceptions of secondary hypogonadism when fertility is required, and growth hormone deficiency (GHD), and to safely minimise both symptoms and clinical signs. Adrenocorticotropic hormone deficiency replacement is best performed with the immediate-release oral glucocorticoid hydrocortisone (HC) in 2–3 divided doses. However, novel once-daily modified-release HC targets a more physiological exposure of glucocorticoids. GHD is treated currently with daily subcutaneous GH, but current research is focusing on the development of once-weekly administration of recombinant GH. Hypogonadism is targeted with testosterone replacement in men and on estrogen replacement therapy in women; when fertility is wanted, replacement targets secondary or tertiary levels of hormonal settings. Thyroid-stimulating hormone replacement therapy follows the rules of primary thyroid gland failure with L-thyroxine replacement. -

Underactive Thyroid Gland
AMERICAN THYROID ASSOCIATION® www.thyroid.org Hypothyroidism WHAT IS THE THYROID GLAND? WHAT CAN YOU EXPECT OVER THE LONG TERM? The thyroid gland is a butterfly-shaped endocrine gland There is no cure for hypothyroidism, and most patients that is normally located in the lower front of the neck. have it for life. There are exceptions: many patients with The thyroid’s job is to make thyroid hormones, which are viral thyroiditis have their thyroid function return to normal, secreted into the blood and then carried to every tissue as do some patients with thyroiditis after pregnancy. in the body. Thyroid hormone helps the body use energy, Hypothyroidism may become more or less severe, and stay warm and keep the brain, heart, muscles, and other your dose of thyroxine may need to change over time. You organs working as they should. have to make a lifetime commitment to treatment. But if you take your pills every day and work with your doctor WHAT IS HYPOTHYROIDISM? to get and keep your thyroxine dose right, you should Hypothyroidism is an underactive thyroid gland. be able to keep your hypothyroidism well controlled Hypothyroidism means that the thyroid gland can’t make throughout your life. Your symptoms should disappear and enough thyroid hormone to keep the body running the serious effects of low thyroid hormone should improve. normally. People are hypothyroid if they have too little If you keep your hypothyroidism well-controlled, it will not thyroid hormone in the blood. Common causes are shorten your life span. autoimmune disease, such as Hashimoto’s thyroiditis, surgical removal of the thyroid, and radiation treatment. -

Concurrence of Graves's Disease and Hashimoto's Thyroiditis
Arch Dis Child: first published as 10.1136/adc.52.12.951 on 1 December 1977. Downloaded from Archives of Disease in Childhood, 1977, 52, 951-955 Concurrence of Graves's disease and Hashimoto's thyroiditis TAMOTU SATO, IKURO TAKATA, TOKUO TAKETANI, KOHKI SAIDA, AND HIRONORI NAKAJIMA From the Department ofPaediatrics, School of Medicine, Kanazawa University, Takaramachi 13-1, Kanazawa, 920 Japan SUMMARY Early histological changes in the thyroid gland were examined in 30 patients with juvenile thyrotoxicosis, by means of needle biopsy. Based on the degree of lymphocytic infiltration and de- generative changes in follicular epithelium, results were classified into four groups. A: hyperplastic changes without cellular infiltration (6 patients, 20%); B: hyperplastic changes with areas of focal thyroiditis <300% of specimen (10 patients, 33 %); C: those with 30 to 600% areas of thyroiditis (10 patients, 33 %); D: almost diffuse thyroiditis (4 patients, 13 %). Moderate to severe lymphocytic thyroiditis was frequently present in the early stage of hyperplastic thyroid glands. The clinical significance of the 4 histological groups was evaluated. Neither clinical signs nor routine laboratory tests could differentiate these groups except group D, in which thyrotoxic signs were mild and transient. However, serum antithyroid antibodies tended to increase in accordance with severity of thyroiditis. The rate of remission was high in groups C and D, whereas relapse was copyright. frequent in group A. These results suggest that Graves's disease and chronic lymphocytic thyroiditis are closely related in the early stage of thyrotoxicosis in children, and that the clinical course may be considerably altered by the degree of associated thyroiditis. -

Acquired Hypothyroidism in Children: a Guide for Families
Pediatric Endocrinology Fact Sheet Acquired Hypothyroidism in Children: A Guide for Families What does hypothyroidism mean? How is hypothyroidism diagnosed? Hypothyroidism refers to an underactive thyroid gland Simple blood tests are used to diagnose hypothyroidism. that does not produce enough of the active hormones T3 and These include the measurement of hormones produced by T4. This condition can be present at birth or can be acquired the thyroid gland and pituitary. Free T4 (which is more ac- any time during childhood or aduthood. Hypothyroidism is curate than just the total T4) and TSH are measured. The tests very common and occurs in about 1 in 1250 children. In most are inexpensive and widely available at your regular doctor’s cases, the condition is permanent and will require treatment office. Hypothyroidism is diagnosed when the stimulating for life. This discussion will focus on the causes of hypothy- hormone from the pituitary (TSH) is high and the free T4 roidism in children arising after birth. produced from the thyroid is low. If there is not enough TSH, The thyroid gland is a butterfly-shaped organ located in then both levels will be low. Normal ranges for free T4 and the middle of the neck. It is responsible for producing the thy- TSH are somewhat different in children than adults, so the roid hormones T3 and T4. This production is controlled by diagnosis should be made in consultation with a pediatric the pituitary gland in the brain via thyroid stimulating hor- endocrinologist. mone (called TSH). T3 and T4 perform many important ac- tions during childhood, including the maintenance of normal What is the treatment for hypothyroidism? growth and bone development.