The Multiple Borders in the Health Care Provided to Foreigners in Corumbá
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
En En Motion for a Resolution
European Parliament 2014-2019 Plenary sitting B8-0315/2018 2.7.2018 MOTION FOR A RESOLUTION to wind up the debate on the statement by the Vice-President of the Commission / High Representative of the Union for Foreign Affairs and Security Policy pursuant to Rule 123(2) of the Rules of Procedure on the migration crisis and humanitarian situation in Venezuela and at its borders (2018/2770(RSP)) Agustín Díaz de Mera García Consuegra, José Ignacio Salafranca Sánchez-Neyra, Cristian Dan Preda, Luis de Grandes Pascual, José Inácio Faria, Verónica Lope Fontagné, Gabriel Mato, David McAllister, Dubravka Šuica, Sandra Kalniete, Elmar Brok, Lorenzo Cesa, Michael Gahler, Francisco José Millán Mon, Tunne Kelam, Fernando Ruas, Laima Liucija Andrikienė, Eduard Kukan, Julia Pitera, Ivan Štefanec, Jaromír Štětina, Esteban González Pons on behalf of the PPE Group RE\1158023EN.docx PE621.741v01-00 EN United in diversity EN B8-0315/2018 European Parliament resolution on the migration crisis and humanitarian situation in Venezuela and at its borders (2018/2770(RSP)) The European Parliament, – having regard to its previous resolutions on Venezuela, in particular those of 27 February 2014 on the situation in Venezuela1, of 18 December 2014 on the persecution of the democratic opposition in Venezuela2, of 12 March 2015 on the situation in Venezuela3, of 8 June 2016 on the situation in Venezuela4, of 27 April 2017 on the situation in Venezuela5, of 8 February 2018 on the situation in Venezuela6, and of 3 May 2018 on the elections in Venezuela7, – having regard -

The Marouini River Tract and Its Colonial Legacy in South America
The Marouini River Tract And Its Colonial Legacy in South America Thomas W. Donovan∗ I. Introduction In perhaps the most desolate and under-populated area in the South America lies one of the most lingering boundary conflicts of modern nations. Suriname and French Guiana (an overseas colony of France) dispute which of the upper tributaries of the Maroni River1 was originally intended to form the southern extension of their border. The Maroni River exists as the northern boundary between the two bordering nations on the Caribbean coast, and was intended to serve as the boundary to the Brazilian border.2 The disputed area, deemed the Marouini River Tract,3 is today administered by France under the Overseas Department. Most modern maps, except those produced by Suriname, indicate that the land is a possession of French Guiana. However, Suriname claims that it has always been the rightful owner of the region and that France should relinquish it to them. The territory covers approximately 5,000 square miles of inland Amazon forest and apparently contains significant bauxite, gold, and diamond resources and potential hydroelectric production. The area has remained undeveloped and subject to dispute for over 300 years. It has received scant international attention. And today it remains one of many borders in the Guianas that has resisted solution. 4 It is a continuous reminder of the troubled colonial legacy in Latin America and the Caribbean. This paper will describe the historical roots of the dispute, the different claims over time, and the legal precedents to support such claims. The paper will indicate that French Guiana would be more likely to perfect title to the Marouini River Tract if the issue were ever referred to an international tribunal. -
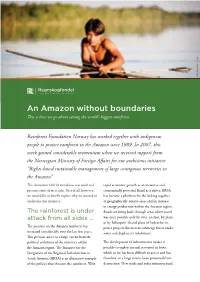
An Amazon Without Boundaries This Is How We Go About Saving the World’S Biggest Rainforest
Photo:: Jørgen Braastad Jørgen Photo:: An Amazon without boundaries This is how we go about saving the world’s biggest rainforest Rainforest Foundation Norway has worked together with indigenous people to protect rainforest in the Amazon since 1989. In 2007, this work gained considerable momentum when we received support from the Norwegian Ministry of Foreign Affairs for our ambitious initiative “Rights-based sustainable management of large contiguous territories in the Amazon”. This document (2012) introduces our work and rapid economic growth as an incentive and presents some of its results. First of all, however, economically powerful Brazil as a driver, IIRSA we would like to briefly explain why we wanted to has become a platform for the linking together undertake this initiative. of geographically remote areas and an increase in energy production within the Amazon region. The rainforest is under Roads are being built through areas where travel attack from all sides … was once possible only by river, on foot, by plane or by helicopter. Grand plans of hydroelectric The pressure on the Amazon rainforest has power projects threaten to submerge forest under increased considerably over the last few years. water and displace its inhabitants. This pressure arises to a large extent from the political ambitions of the countries within The development of infrastructure makes it the Amazon region. The Initiative for the possible to exploit natural resources in forest Integration of the Regional Infrastructure in which so far has been difficult to access and has South America (IIRSA) is an illustrative example therefore, to a large extent, been protected from of the policies that threaten the rainforest. -

Integration and International Security in the Guyana Shield: Challenges and Opportunities
43 Integration and International Security in the Guyana Shield: challenges and opportunities Paulo Gustavo Pellegrino Correa1 Eliane Superti2 Resumo O presente trabalho se propõe a discutir o binômio integração/segurança internacional na região do Platô das Guianas, composto por cinco territórios: Brasil, Guiana Francesa (França), Suriname, Guiana e Venezuela. Abordaremos o binômio no Platô a partir de elementos recorrentes que compõem a constelação de segurança e a dinâmica de integração. Quais sejam: o fluxo migratório intraregional, com destaque aos grupos brasileiros presentes nos territórios da região; a extração de ouro e as atividades que compõem o garimpo (armas, drogas, comércio, prostituição), colocada como um problema de segurança em diferentes aspectos; os litígios fronteiriços não resolvidos desde o período colonial que, com exceção do Brasil, envolve todos os países do Platô das Guianas; a falta de interconectividade entre os territórios, colocando-os “de costas” para o subcontinente. Palavras-Chave: Guiana, Platô das Guianas; Integração das Guianas. Resumen Este estudio se propuso analizar el binomio integración/seguridad internacional de la región de las Guayanas, integrada por cinco países: Brasil, Guayana Francesa (Francia), Surinam, Guyana y Venezuela. Se discute el binomio en la Meseta de los elementos que conforman la constelación de la seguridad y la dinámica de la integración. A saber: la migración intrarregional, especialmente a los grupos brasileños presentes en la región; la extracción de oro y de las actividades que conforman la minería (armas, drogas, comercio, prostitución) colocado como un problema de seguridad en diferentes aspectos; disputas fronterizas sin resolver desde la época colonial, con la excepción de Brasil, involucra todos los países de las Guyanas; la falta de interconexión entre las regiones, de ponerlos "en la espalda" al subcontinente. -

WILDLIFE TRAFFICKING in BRAZIL Sandra Charity and Juliana Machado Ferreira
July 2020 WILDLIFE TRAFFICKING IN BRAZIL Sandra Charity and Juliana Machado Ferreira TRAFFIC: Wildlife Trade in Brazil WILDLIFE TRAFFICKING IN BRAZIL TRAFFIC, the wildlife trade monitoring network, is a leading non-governmental organisation working globally on trade in wild animals and plants in the context of both biodiversity conservation and sustainable development. © Jaime Rojo / WWF-US Reproduction of material appearing in this report requires written permission from the publisher. The designations of geographical entities in this publication, and the presentation of the material, do not imply the expression of any opinion whatsoever on the part of TRAFFIC or its supporting organisations concerning the legal status of any country, territory, or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. TRAFFIC David Attenborough Building, Pembroke Street, Cambridge CB2 3QZ, UK. Tel: +44 (0)1223 277427 Email: [email protected] Suggested citation: Charity, S., Ferreira, J.M. (2020). Wildlife Trafficking in Brazil. TRAFFIC International, Cambridge, United Kingdom. © WWF-Brazil / Zig Koch © TRAFFIC 2020. Copyright of material published in this report is vested in TRAFFIC. ISBN: 978-1-911646-23-5 UK Registered Charity No. 1076722 Design by: Hallie Sacks Cover photo: © Staffan Widstrand / WWF This report was made possible with support from the American people delivered through the U.S. Agency for International Development (USAID). The contents are the responsibility of the authors and do not necessarily -

Mission in Brazil
Prestes Filho: The Karajá Mission in Brazil UBIRAJARA DE FARIAS PRESTES FILHO The Karajá Mission in Brazil Introduction For a long time indigenous peoples were pretty much a marginal- ized part of Brazil’s official history. Their conquest and genocide lasted for five hundred years while the traditional view of history emphasizes a harmonious meeting between indigenous people and Europeans, which together with the Africans formed Brazil’s national culture. However, a more detailed analysis shows what really happened was a very violent and cruel conquest with enslavement, transmission of diseases, land inva- sion, and intolerance towards their religious ideas. The story of Brazil’s actions towards its indigenous people is a story full of tragedies, few hopes, and little expectation, but things have started to change in the last few decades. There was a widely held idea that the natural evolution of the indigenous people would integrate them with the national society in such a way that their indigenous cultures would blend in with the rest of Brazil’s cultures as they were assimilated. Contrary to what many people taught in the 20th century, the indigenous nations did not disappear by the end of the millennium. Instead, their population is increasing every year, and there are a growing number of institutions that are fighting to get back their lands and to force changes that will result in respect for their cultures. During the 20th century there was progress in the study of anthropol- ogy and people became more conscious about the need to promote self- determination among the various people groups and to allow all people groups to have the right to live according to their own cultural beliefs. -

Territorial Planning an La Plata Basin Borders
© 2018 Editors Antonio Paulo Cargnin Aldomar Arnaldo Rückert Bruno de Oliveira Lemos Editorial Board Carla Giane Soares da Cunha Fernando Dreissig de Moraes Irma Carina Macolmes Language Review Marlise Margô Henrich Layout Diego MeneghettI Ronaldo Machado Cover Design Laurie Fofonka Cunha Institutional support Programa de Pós-Graduação em Geografia (POSGEA) Instituto de Geociências (IGEO) Universidade Federal do Rio Grande do Sul (UFRGS), Brazil Secretaria de Planejamento, Governança e Gestão (SPGG) Governo do Estado do Rio Grande do Sul, Brazil Dados Internacionais de Publicação Bibliotecária Regina de Carvalho Pereira CRB8/91772 T327 Territorial planning and La Plata Basin borders / Antonio Paulo Cargnin, Aldomar Arnaldo Rückert, Bruno www.editoraletra1.com.br de Oliveira Lemos (Eds.) . – Porto Alegre : Editora Letra1, [email protected] 2018. 232p. (+5551) 3372 9222 ISBN 978-85-63800-35-0 DOI 10.21826/9788563800350 Rua Lopo Gonçalves, 554 1. Brasil - Fronteiras.2. La Plata - Fronteira. 3. Território. I. Cidade Baixa 90050-350 Cargnin, Antonio Paulo. II. Rückert, Aldomar Arnaldo. III Porto Alegre, RS, Brazil Lemos, Bruno de Oliveira. III. Título. CNPJ 12.062.268/0001-37 CDD 320.12 III LA PLATA REGION TRIPOINTS: STATE OF THE MATTER AND DESCRIPTIVE COMPARISON Alejandro Benedetti ABSTRACT Where the Paraná and Iguazú rivers meet, the most important and studied trinational region of South America is located: the Triple Frontier. However, this is only one of the 13 tripartite points that were formed in that continental region from the process of interstate delimitation which occurred, centrally, between the late 19th and early 20th century. Five out of these involve the countries of La Plata Basin, and will be called: Quareim (Argentina-Brazil-Uruguay); Iguazú (Argentina-Brazil-Paraguay); Esmeralda (Argentina-Bolivia-Paraguay); Zapaleri (Argentina-Bolivia-Chile); and Bahía Negra (Argentina- Bolivia-Brazil). -

Terrorism Base Potential in the Tri-Border Area of Latin America
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Calhoun, Institutional Archive of the Naval Postgraduate School Calhoun: The NPS Institutional Archive Theses and Dissertations Thesis Collection 2006-12 Terrorism base potential in the tri-border area of Latin America Halaburda, Pablo. Monterey, California. Naval Postgraduate School http://hdl.handle.net/10945/2454 NAVAL POSTGRADUATE SCHOOL THESIS TERRORISM BASE POTENTIAL IN THE TRI-BORDER AREA OF LATIN AMERICA by Pablo Halaburda December 2006 Thesis Advisor: Kalev Sepp Second Reader: Hy Rothstein Approved for public release; distribution is unlimited THIS PAGE INTENTIONALLY LEFT BLANK REPORT DOCUMENTATION PAGE Form Approved OMB No. 0704-0188 Public reporting burden for this collection of information is estimated to average 1 hour per response, including the time for reviewing instruction, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to Washington headquarters Services, Directorate for Information Operations and Reports, 1215 Jefferson Davis Highway, Suite 1204, Arlington, VA 22202-4302, and to the Office of Management and Budget, Paperwork Reduction Project (0704-0188) Washington DC 20503. 1. AGENCY USE ONLY (Leave blank) 2. REPORT DATE 3. REPORT TYPE AND DATES COVERED December 2006 Master’s Thesis 4. TITLE AND SUBTITLE: Terrorism Base Potential in the Tri-Border Area 5. FUNDING NUMBERS of Latin America 6. AUTHOR(S) Pablo Halaburda 7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES) 8. PERFORMING Naval Postgraduate School ORGANIZATION REPORT Monterey, CA 93943-5000 NUMBER 9. -
En En Motion for a Resolution
European Parliament 2014-2019 Plenary sitting B8-0320/2018 2.7.2018 MOTION FOR A RESOLUTION to wind up the debate on the statement by the Vice-President of the Commission / High Representative of the Union for Foreign Affairs and Security Policy pursuant to Rule 123(2) of the Rules of Procedure on the migration crisis and humanitarian situation in Venezuela and at its borders (2018/2770(RSP)) Ignazio Corrao, Fabio Massimo Castaldo on behalf of the EFDD Group RE\1158028EN.docx PE621.748v01-00 EN United in diversity EN B8-0320/2018 European Parliament resolution on the migration crisis and humanitarian situation in Venezuela and at its borders (2018/2770(RSP)) The European Parliament, – having regard to the Universal Declaration of Human Rights of 1948, – having regard to the International Covenant on Civil and Political Rights, – having regard to the International Covenant on Economic, Social and Cultural Rights, – having regard to the Rome Statute of the International Criminal Court and to the statement of 8 February 2018 by the Prosecutor of the International Criminal Court, Ms Fatou Bensouda, – having regard to the statement of the UN High Commissioner for Human Rights on Venezuela of 31 March 2017, – having regard to the report by the Office of the UN High Commissioner for Human Rights (OHCHR) entitled ‘Human Rights violations in the Bolivarian Republic of Venezuela’ of 22 June 2018, – having regard to the declaration of 20 April 2018 by the Organisation of American States (OAS) on the worsening humanitarian situation in Venezuela, -

State Devices, Illegalisms and Social Practices In
e-ISSN 2395-9134 Estudios Fronterizos, vol. 19, 2018, e012 https://doi.org/10.21670/ref.1812012 Articles State devices, ilegalisms, and social practices in the Brazil-Paraguay border (1890-2015) Dispositivos estatales, ilegalismos y prácticas sociales en la frontera Brasil-Paraguay (1890-2015) Eric Cardin a* https://orcid.org/0000-0001-7813-5544 Cintia Fiorotti Lima b https://orcid.org/0000-0003-2704-3230 a Universidad Estadual del Oeste de Paraná, Brazil, e-mail: [email protected] b Secretaria do Estado de Educação do Paraná, Brazil, e-mail: [email protected] Abstract The objective of the investigation is to analyze the development of illegal prac- tices and their relations with the control and repression devices in the Brazil/ Paraguay border, specifically in the boundaries between Foz de Iguazú-Ciudad del Este and Guaíra-Salta del Guairá. Methodologically, we use interviews, bib- liographic sources and criminal processes. Through the sociological historical approach, we problematize the relations between illegal practices and state ap- Received on June 13, 2017. Accepted on May 24, 2018. paratus in three specific moments, which represent periods where the Brazilian Published on June 21, 2018. government and the inhabitants of the zones referred to presented different po- sitions in relation to the borders. The investigation allowed to conclude that the organization of the labor market and the experiences of the residents of the bor- der are related to the intensity of the presence of the State in the region studied. ORIGINAL ARTICLE LANGUAGE: SPANISH. Keywords: borders, State, society, illegal practices. Resumen *Corresponding author: Eric Cardin, e-mail: [email protected] El objetivo de la investigación es analizar el desarrollo de las prácticas ilegales y sus relaciones con los aparatos de fiscalización y represión en la frontera Bra- sil-Paraguay, específicamente en los límites entre Foz de Iguazú-Ciudad del Este y Guaíra-Salto del Guairá. -

Summary History of Brazil
SUMMARY HISTORY OF BRAZIL By Joey Willemsen and Bart Leferink Historical overview map of Brazil In this historical overview map of Brazil, the Meridian of Tordesillas, borders of the capitanias (as introduces by King João of Portugal in the sixteenth century), routes of the bandeirantes, current borders of Brazil and important cities are shown. This map will help to clarify the described history. Pará Maranhão Piauí Ceará Itamaracá • Olinda • Recife Pernambuco Mato Bahia Grosso • São Salvador da Bahia de Todos os Ilhéus Santos BOLIVIA Pôrto Seguro Meridian of Tordesillas Minas Gerais Espírito Santo Route of the São Tomé bandeirismo Rio de Janerio NEIGHBOUR COUNTRY PARAGUAY • Rio de Janeiro São Paulo de Piratininga • Santo Amaro capitania São Vicente • São Vicente • City Santana Rio Grande ARGENTINA do Sul URUGUAY La Plata Figure 1 Historical overview map of Brazil. (Based on C.M. Schulten, 1966 pag. 1) Pre-colonial history By the time the Portuguese arrived in 1500 AD, the area of what is now Brazil was already populated for thousands of years. Researchers found evidence of human presence there 50.000 years ago. Most of the indigenous peoples were Tupi-Guarani Indians, but the population was quite diverse. Unlike the Inca’s and the Maya’s on the west coast, Brazil’s early inhabitants never developed a highly advanced civilization. The Andes and the mountain range in northern South America formed a rather sharp cultural boundary between the civilizations. The indigenous Brazilians left only a few clues for archaeologists to follow, like pottery and skeletons. For this reason, very little is known about the indigenous people of Brazil. -

A Cross-Border Deforestation Index to Understand Underlying Drivers of Deforestation
XIII World Forestry Congress Buenos Aires, Argentina, 18 – 23 October 2009 A cross-border deforestation index to understand underlying drivers of deforestation L.M See1, S. Fritz, I. McCallum, M. Obersteiner, and S. Bone This paper considers a preliminary investigation involving the development of a Cross-Border Deforestation Index (CBDI), which is an attempt to quantify the differences in deforestation between two countries or potentially any two administrative units. In this study, the focus was on countries. For each pair of bordering countries, a 50 km buffer zone was drawn and the average value of the Vegetation Continuous Field (VCF) was calculated for each country in the pair. The ratio of these two averages is the CBDI. Values of 1 indicate similar levels of forest cover but values greater than 1 point towards dissimilar land use policies within countries and/or sub-national administrative levels. This index was calculated for all pairs of bordering tropical countries in South and Central America, Asia and Africa. In addition, a visual analysis of the spatial variation of the VCF was undertaken to show how this can complement the CBDI. The results showed that countries such as Argentina, Brazil, Chile, El Salvador, Laos, Thailand and DR Congo, in combination with different neighbouring countries, all have CBDI values differing from 1. These areas are worth examining in greater detail in order to understand what types of drivers are behind these outlying CBDI values. These drivers could include land use policy, population pressure, accessibility, etc. Future work will include the addition of environmental factors. By computing the CBDI for so called Homogeneous Response Units (HRU: areas of similar or identical environmental conditions in terms of soil, altitude and slope), we will be able to examine the changing effect on the CBDI.