Punctate Palmoplantar Keratoderma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic Spiny Keratoderma: a Report of Two Cases and Literature Review
Idiopathic Spiny Keratoderma: A Report of Two Cases and Literature Review Jessica Schweitzer, DO,* Matthew Koehler, DO,** David Horowitz, DO*** *Intern, Largo Medical Center, Largo, FL **Dermatology Resident, Third Year, College Medical Center/Western University, Long Beach, CA ***Dermatology Residency Program Director, College Medical Center/Western University, Long Beach, CA Abstract Spiny keratoderma is a rare and likely underreported condition that presents with punctate hyperkeratotic growths localized to the palms and soles. We present two cases of clinically diagnosed spiny keratoderma. Although the lesions were asymptomatic, patients are at risk of an underlying internal malignancy with this condition, so diagnosis is crucial. Neither men were seeking treatment for the lesions when they were discovered, suggesting that this condition may be much more common than reported. Patients with histories of manual labor, increased UV exposure, and non-melanoma skin cancer (NMSC) may also be at higher risk for developing spiny keratoderma.1 The epidemiology, histopathologic features, differential diagnosis, and current treatments for spiny keratoderma are reviewed. Introduction Case 2 enthusiast for his entire life, spending significant Spiny keratoderma is a rare palmoplantar A 67-year-old Caucasian male presented with a time using his hands to maintain and fire his keratoderma that presents with keratotic, pinpoint one-year history of insidiously growing, pinpoint weapons and many hours outside without sun papules on the palms and soles. There are both hyperkeratotic papules projecting from his palms protection. The patient was referred back to his hereditary and acquired forms. When found, bilaterally (Figures 4-5). He presented to the clinic primary care physician for internal evaluation. -

Palmoplantar Keratoderma with Progressive Gingivitis and Recurrent Pyodermas
Palmoplantar Keratoderma With Progressive Gingivitis and Recurrent Pyodermas Tyler A. Moss, DO; Anne P. Spillane, MD; Sam F. Almquist, MD; Patrick E. McCleskey, MD; Oliver J. Wisco, DO Practice Points Papillon-Lefèvre syndrome (PLS) is an autosomal-recessive inherited transgredient palmoplantar kerato- derma (PPK) that is associated with gingivitis and recurrent pyodermas. The symptoms associated with PLS are thought to be due to cathepsin C gene, CTSC, mutations. CTSC is expressed in epithelial regions commonly affected by PLS and also plays a role in the activation of immune and inflammatory responses. Papillon-Lefèvre syndrome must be differentiated from other conditions causing PPK, such as Haim-Munk syndrome, Greither syndrome, mal de Meleda, Clouston syndrome, Vohwinkel syndrome, and Olmsted syndrome. Treatment of PLS includesCUTIS keratolytics such as urea and/or salicylic acid comb ined with oral retinoids. Active gingivitis may be treated with combined use of amoxicillin and metronidazole. Papillon-Lefèvre syndrome (PLS) is a rare inher- Case Report ited palmoplantar keratoderma (PPK) that is asso- A 30-year-old woman presented to the dermatology ciated with progressive gingivitis and recurrent clinic with erythematous hyperkeratotic plaques on pyodermas.Do We present a caseNot exhibiting classic the palmsCopy and soles. The plaques extended onto features of this autosomal-recessive condition the dorsal aspects of the fingers, toes, hands, and and review the current understanding of its patho- feet (Figures 1 and 2). The patient had psoriasiform physiology, diagnosis, and treatment. Addition- plaques on the extensor surfaces of the knees and ally, a review of pertinent transgredient PPKs is elbows (Figure 3) along with a history of slow- undertaken, with key and distinguishing features progressing gingivitis and periodontal disease that of each syndrome highlighted. -

Erythrokeratodermia Variabilis Et Progressiva Allelic to Oculo-Dento
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector COMMENTARY See related article on pg 1540 translocated into the plasma membrane. Once expressed on the cell surface, the hemichannel docks with a connexon of an adjacent cell to form a channel that Erythrokeratodermia Variabilis et is termed gap junction. Connexons can form either homotypic (docking of two Progressiva Allelic to Oculo-Dento- identical connexons), heterotypic (docking of two dissimilar homomeric Digital Dysplasia connexons), or heteromeric (docking of two heteromeric connexons) channels Sabine Duchatelet1,2 and Alain Hovnanian1,2,3 (Mese et al., 2007). These diverse Erythrokeratodermia variabilis et progressiva (EKVP) is a genodermatosis with combinations of connexins create clinical and genetic heterogeneity, most often transmitted in an autosomal different types of channels, each having dominant manner, caused by mutations in GJB3 and GJB4 genes encoding unique properties (ionic conductance, connexins (Cx)31 and 30.3, respectively. In this issue, Boyden et al. (2015) report permeability, sensitivity to voltage, or for the first time de novo dominant mutations in GJA1 encoding the ubiquitous pH). Of note, several connexins may also Cx43 in patients with EKVP. These results expand the genetic heterogeneity of form functional nonjunctional hemi- EKVP and the human disease phenotypes associated with GJA1 mutations. They channels, although their physiological disclose that EKVP is allelic to oculo-dento-digital dysplasia, a rare syndrome relevance remains uncertain (Pfenniger previously known to be caused by dominant GJA1 mutations. et al., 2010). Mutations in 11 connexin genes cause a variety of genetic dis- Journal of Investigative Dermatology (2015) 135, 1475–1478. -

Palmoplantar Keratoderma: Rare Case Report
Case Report Journal of Volume 12:4, 2021 Cytology & Histology ISSN: 2157-7099 Open Access Palmoplantar Keratoderma: Rare Case Report Dr. Ayushi Bansal1, Dr. Hemlata Munde2*, Dr. Munish Gupta3 and Dr. Santosh Munde4 1Senior Resident, Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 2Professor and Head of Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 3Assistant Professor, Department of medicine, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 4Professor and Head of Department of Orthopaedics, Kalpana Chawla Government Medical College, Karnal, Haryana, India. Abstract Palmoplantar keratodermas(PPK) are group of cornification disorders characterized by epidermal hyperkeratotic lesions involving the palms and soles. A 50years old healthy male, presented with history of multiple punctate hyperkeratotic papules since last 5 years. Keywords: Palmoplantar keratoderma • Punctate •Hyperkeratotic papules Abbreviations: PPK: Palmoplantar keratodermas • PUVA: Psoralen plus Ultraviolet A • PPPK: Punctate Palmoplantar keratodermas • USG: Ultrasound Sonography• VRDL: Venereal Disease Research Laboratory Test • ELISA: Enzyme-Linked Immunosorbent Assay Introduction Mucosal surfaces were not involved. Biopsy sample was received. On histopathological examination of biopsy revealed massive hyperkeratosis over sharply limited area with depression of malphigian layer below general Palmoplantar keratoderma (PPK), clinically and genetically comprises level of epidermis. There was increase in the thickness of granular layer. The of heterogenous group of disorders characterised by hyperkeratosis of dermis was free of inflammation. Compilation of clinical and laboratory data palms and soles [1]. It can be hereditary or acquired. Hereditary PPK can helped to conclude the diagnosis of Palmoplantar Keratoderma-Punctate be further divided into three major categories: diffuse, focal, and punctate type. -

Dermatologic Features of Smith–Magenis Syndrome
Pediatric Dermatology Vol. 32 No. 3 337–341, 2015 Dermatologic Features of Smith–Magenis Syndrome Morgane Guerin-Moreau, M.D.,*,** Estelle Colin, M.D.,†,** Sylvie Nguyen, M.D., Ph.D.,‡,** Joris Andrieux, M.D., Ph.D.,§ Helene de Leersnyder, M.D.,¶ Dominique Bonneau, M.D., Ph.D.,†,** and Ludovic Martin, M.D., Ph.D.*,** Departments of *Dermatology, †Biochemistry and Genetics, and ‡Pediatrics, University Hospital of Angers, Angers, France, §Department of Genetics, University Hospital of Lille, Lille, France, ¶Department of Pediatrics, Hopital^ Robert Debre, University of Paris VII, Paris, France, **L’UNAM University, Nantes, France Abstract: Smith–Magenis syndrome (SMS) is characterized by dis- tinctive facial and skeletal features, developmental delay, cognitive impairment, and behavioral abnormalities, including self-injurious behav- iors. We aimed to investigate whether cutaneous features are common in SMS. We performed a complete skin examination in 20 young SMS patients. Skin features secondary to self-injurious behavior, such as bites, abrasions, dystrophic scars, limited spots of hyperkeratosis, anomalies of the nails, and whitlows, were found in the majority of patients. Acral pachydermia and fissured plantar keratoderma were common. Xerosis was constant and associated with extensive keratosis pilaris in the majority of patients. Dermatofibromas were frequent in older patients. The hair was dense and shiny, with an unusual hairline. Eyelash trichomegaly and heavy brows were common, as well as folliculitis on the back. The skin features of SMS have rarely been reported in the literature. Some of these are the consequence of neurobehavioral features, but some cutaneous features and abnormalities of appendages have not been reported in other related syndromes. -
Spiny Keratoderma Thomas N
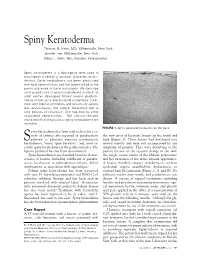
Spiny Keratoderma Thomas N. Helm, MD, Williamsville, New York Jennifer Lee, Williamsville, New York Klaus F. Helm, MD, Hershey, Pennsylvania Spiny keratoderma is a descriptive term used to encompass a variety of unusual, disparate kerato- dermas. Spiny keratoderma has been associated with lipid abnormalities and has been limited to the palms and soles in some individuals. We describe an acquired case of spiny keratoderma in which an adult woman developed filiform lesions predomi- nating on the trunk and proximal extremities. Treat- ment with topical emollients and keratolytic agents was unsuccessful, but topical tazarotene led to long periods of resolution. She has had no other associated abnormalities. The clinical features and differential diagnosis of spiny keratoderma are reviewed. FIGURE 1. Spiny keratoderma lesions on the back. piny keratoderma has been used to describe a va- riety of entities also reported as porokeratosis the new onset of keratotic lesions on the trunk and S palmaris et plantaris, punctate porokeratotic back (Figure 1). These lesions had developed over keratoderma, “music spine keratosis,” and, most re- several months and were not accompanied by any cently, spiny keratoderma of the palms and soles. Ma- symptoms of pruritus. They were disturbing to the lignant potential has not been documented. patient because of the textural change in the skin; Spiny keratodermas are classified based on charac- the rough, coarse nature of the filiform projections; teristics of lesions, including exhibition of paraker- and her awareness of her skin’s unusual appearance. atosis, localization to palmoplantar surfaces, diffuse A biopsy revealed compact orthokeratosis without involvement, or association with appendages.1 epidermal atypia, acantholytic dyskeratosis, or Palmar spiny keratoderma has been associated cornoid lamella formation (Figure 2, A and B). -

Hereditary Hearing Impairment with Cutaneous Abnormalities
G C A T T A C G G C A T genes Review Hereditary Hearing Impairment with Cutaneous Abnormalities Tung-Lin Lee 1 , Pei-Hsuan Lin 2,3, Pei-Lung Chen 3,4,5,6 , Jin-Bon Hong 4,7,* and Chen-Chi Wu 2,3,5,8,* 1 Department of Medical Education, National Taiwan University Hospital, Taipei City 100, Taiwan; [email protected] 2 Department of Otolaryngology, National Taiwan University Hospital, Taipei 11556, Taiwan; [email protected] 3 Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei City 100, Taiwan; [email protected] 4 Graduate Institute of Medical Genomics and Proteomics, National Taiwan University College of Medicine, Taipei City 100, Taiwan 5 Department of Medical Genetics, National Taiwan University Hospital, Taipei 10041, Taiwan 6 Department of Internal Medicine, National Taiwan University Hospital, Taipei 10041, Taiwan 7 Department of Dermatology, National Taiwan University Hospital, Taipei City 100, Taiwan 8 Department of Medical Research, National Taiwan University Biomedical Park Hospital, Hsinchu City 300, Taiwan * Correspondence: [email protected] (J.-B.H.); [email protected] (C.-C.W.) Abstract: Syndromic hereditary hearing impairment (HHI) is a clinically and etiologically diverse condition that has a profound influence on affected individuals and their families. As cutaneous findings are more apparent than hearing-related symptoms to clinicians and, more importantly, to caregivers of affected infants and young individuals, establishing a correlation map of skin manifestations and their underlying genetic causes is key to early identification and diagnosis of syndromic HHI. In this article, we performed a comprehensive PubMed database search on syndromic HHI with cutaneous abnormalities, and reviewed a total of 260 relevant publications. -

Blueprint Genetics Epidermolysis Bullosa Panel
Epidermolysis Bullosa Panel Test code: DE0301 Is a 26 gene panel that includes assessment of non-coding variants. Is ideal for patients with a clinical suspicion of congenital epidermolysis bullosa. About Epidermolysis Bullosa Epidermolysis bullosa (EB) is a group of inherited diseases that are characterised by blistering lesions on the skin and mucous membranes, most commonly appearing at sites of friction and minor trauma such as the feet and hands. In some subtypes, blisters may also occur on internal organs, such as the oesophagus, stomach and respiratory tract, without any apparent friction. There are 4 major types of EB based on different sites of blister formation within the skin structure: Epidermolysis bullosa simplex (EBS), Junctional epidermolysis bullosa (JEB), Dystrophic epidermolysis bullosa (DEB), and Kindler syndrome (KS). EBS is usually characterized by skin fragility and rarely mucosal epithelia that results in non-scarring blisters caused by mild or no trauma. The four most common subtypes of EBS are: 1) localized EBS (EBS-loc; also known as Weber-Cockayne type), 2) Dowling-Meara type EBS (EBS-DM), 3) other generalized EBS(EBS, gen-nonDM; also known as Koebner type) and 4) EBS-with mottled pigmentation (EBS-MP). Skin biopsy from fresh blister is considered mandatory for diagnostics of generalized forms of EBS. The prevalence of EBS is is estimated to be 1:30,000 - 50,000. EBS-loc is the most prevalent, EBS- DM and EBS-gen-nonDM are rare, and EBS-MP is even rarer. Penetrance is 100% for known KRT5 and KRT14 mutations. Location of the mutations within functional domains of KRT5and KRT14 has shown to predict EBS phenotype. -

Towards a Comprehensive Resource for Elucidating the Pathogenesis of Inherited Keratodermas
Towards a Comprehensive Resource for Elucidating the Pathogenesis of Inherited Keratodermas Dr Mozheh Zamiri BSc (Hons), MB ChB, MRCP Doctorate of Medicine University of Edinburgh 2009 Alan Lyell Centre for Dermatology, Glasgow & Section of Dermatology, University of Glasgow ABSTRACT Keratoderma – pathological hyperkeratosis of palms and soles - is a cause of disability in many clinical situations, including the rare and heterogeneous group of inherited palmoplantar keratodermas (PPKs). The aim of this study was to work towards better understanding of molecular mechanisms active in the pathogenesis of PPK by the creation of a cell and tissue culture resource and its initial application to laboratory studies. My study was based on a diverse group of autosomal dominant disorders, previously ascertained in families from Scotland, in whom the precise genetic aetiology was known. I established a tissue and cell culture resource of inherited keratodermas of known single-gene aetiology from patients with proven keratin 1, 9, 17, loricrin and mitochondrial mutations. An additional pedigree with striate keratoderma with an unknown mutation was recruited, and the causative mutation identified as a novel heterozygous A-to-T transversion in exon 5 (c.430A>T) of the desmoglein 1 gene, converting an arginine residue to a premature termination codon (p.Arg144stop). The keratinocyte culture resource was established from patients with keratin 1, 9, 17 and loricrin mutations, as well as controls. Due to the pain associated with direct infiltration of plantar skin, biopsies were obtained using peripheral nerve block for plantar biopsy. The effectiveness of this approach, which may be useful for future administration of treatment, was made the subject of an open clinical trial. -

Hereditary Palmoplantar Keratoderma "Clinical and Genetic Differential Diagnosis"
doi: 10.1111/1346-8138.13219 Journal of Dermatology 2016; 43: 264–274 REVIEW ARTICLE Hereditary palmoplantar keratoderma “clinical and genetic differential diagnosis” Tomo SAKIYAMA, Akiharu KUBO Department of Dermatology, Keio University School of Medicine, Tokyo, Japan ABSTRACT Hereditary palmoplantar keratoderma (PPK) is a heterogeneous group of disorders characterized by hyperkerato- sis of the palm and the sole skin. Hereditary PPK are divided into four groups – diffuse, focal, striate and punctate PPK – according to the clinical patterns of the hyperkeratotic lesions. Each group includes simple PPK, without associated features, and PPK with associated features, such as involvement of nails, teeth and other organs. PPK have been classified by a clinically based descriptive system. In recent years, many causative genes of PPK have been identified, which has confirmed and/or rearranged the traditional classifications. It is now important to diag- nose PPK by a combination of the traditional morphological classification and genetic testing. In this review, we focus on PPK without associated features and introduce their morphological features, genetic backgrounds and new findings from the last decade. Key words: diffuse, focal, punctate, striate, transgrediens. INTRODUCTION psoriasis vulgaris confined to the palmoplantar area (Fig. 1b) are comparatively common and are sometimes difficult to Palmoplantar keratoderma (PPK) is a heritable or acquired dis- distinguish from hereditary PPK. A skin biopsy is essential in order characterized by abnormal hyperkeratotic thickening of diagnosing these cases. Lack of a family history is not neces- the palm and sole skin. In a narrow sense, PPK implies heredi- sarily evidence of an acquired PPK, because autosomal reces- tary PPK, the phenotype of which usually appears at an early sive PPK can appear sporadically from parent carriers and age. -

Generalized Epidermolytic Ichthyosis with Palmoplantar Hyperkeratosis
Volume 27 Number 2| February 2021 Dermatology Online Journal || Photo Vignette 27(2):14 Generalized epidermolytic ichthyosis with palmoplantar hyperkeratosis Prasta Bayu Putra1 MD, Sunardi Radiono1 MD, Retno Danarti1 MD Affiliations: 1Department of Dermatology and Venereology, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada/Dr Sardjito Hospital, Yogyakarta, Indonesia Corresponding Author: Retno Danarti, Department of Dermatology and Venereology, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada/Dr Sardjito Hospital, Gedung Radiopoetro Lantai 3, Jalan Farmako Sekip Utara, Yogyakarta 55281, Indonesia, Tel/Fax: 62-274 560700, Email: [email protected] inherited in an autosomal dominant pattern, Abstract although spontaneous mutation represents about Epidermolytic ichthyosis (EI, OMIM 113800) is a rare half of all cases with no family history [1]. The autosomal dominant keratinization disorder that is prevalence of EI is reported to be about 1:100,000- caused by keratin 1 or keratin 10 gene mutation. It can 400,000 with mutations located in keratin (KRT) 1 or be classified clinically based on the presence of 10 genes. The defective KRT gene leads to skin palmoplantar hyperkeratosis involvement and fragility and blistering with erythrodermic clinical extent of skin involvement. The diagnosis is made by manifestations at birth. Hyperkeratosis and scaling clinical and histopathological examinations that can will form as the severity decreases with age [2]. be confirmed by genetic testing. We present a 2-year- old girl who presented with erythematous and thick Epidermolytic ichthyosis can be classified clinically scaling skin. Her condition began at birth as multiple based on the involvement of palmoplantar flaccid blisters that would easily break into erosions. -

How to Deal with Skin Biopsy in an Infant with Blisters?
Review How to Deal with Skin Biopsy in an Infant with Blisters? Stéphanie Leclerc-Mercier Reference Center for Genodermatoses (MAGEC Center), Department of Pathology, Necker-Enfants Malades Hospital, Paris Centre University, 75015 Paris, France; [email protected] Abstract: The onset of blisters in a neonate or an infant is often a source of great concern for both parents and physicians. A blistering rash can reveal a wide range of diseases with various backgrounds (infectious, genetic, autoimmune, drug-related, traumatic, etc.), so the challenge for the dermatologist and the pediatrician is to quickly determine the etiology, between benign causes and life-threatening disorders, for a better management of the patient. Clinical presentation can provide orientation for the diagnosis, but skin biopsy is often necessary in determining the cause of blister formations. In this article, we will provide information on the skin biopsy technique and discuss the clinical orientation in the case of a neonate or infant with a blistering eruption, with a focus on the histology for each etiology. Keywords: blistering eruption; infant; skin biopsy; genodermatosis; SSSS; hereditary epidermolysis bul- losa; keratinopathic ichthyosis; incontinentia pigmenti; mastocytosis; auto-immune blistering diseases 1. Introduction The onset of blisters in a neonate or an infant (<2 years old) is a source of great concern for both parents and physicians. Therefore, a precise diagnosis, between benign causes and Citation: Leclerc-Mercier, S. How to life-threatening disorders, is quickly needed for the best management of the baby. Deal with Skin Biopsy in an Infant Several diseases with various backgrounds (infectious, genetic, autoimmune, drug- with Blisters? Dermatopathology 2021, related, traumatic, etc.) can lead to a blistering eruption.