Prescribing Outlook Includes Such Drugs but Underpinning the Strategic Direction for Managing New Quantifying Their Impact Is Difficult
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Biological, Physiological, Pathophysiological, and Pharmacological Aspects of Ghrelin
0163-769X/04/$20.00/0 Endocrine Reviews 25(3):426–457 Printed in U.S.A. Copyright © 2004 by The Endocrine Society doi: 10.1210/er.2002-0029 Biological, Physiological, Pathophysiological, and Pharmacological Aspects of Ghrelin AART J. VAN DER LELY, MATTHIAS TSCHO¨ P, MARK L. HEIMAN, AND EZIO GHIGO Division of Endocrinology and Metabolism (A.J.v.d.L.), Department of Internal Medicine, Erasmus Medical Center, 3015 GD Rotterdam, The Netherlands; Department of Psychiatry (M.T.), University of Cincinnati, Cincinnati, Ohio 45237; Endocrine Research Department (M.L.H.), Eli Lilly and Co., Indianapolis, Indiana 46285; and Division of Endocrinology (E.G.), Department of Internal Medicine, University of Turin, Turin, Italy 10095 Ghrelin is a peptide predominantly produced by the stomach. secretion, and influence on pancreatic exocrine and endo- Ghrelin displays strong GH-releasing activity. This activity is crine function as well as on glucose metabolism. Cardiovas- mediated by the activation of the so-called GH secretagogue cular actions and modulation of proliferation of neoplastic receptor type 1a. This receptor had been shown to be specific cells, as well as of the immune system, are other actions of for a family of synthetic, peptidyl and nonpeptidyl GH secre- ghrelin. Therefore, we consider ghrelin a gastrointestinal tagogues. Apart from a potent GH-releasing action, ghrelin peptide contributing to the regulation of diverse functions of has other activities including stimulation of lactotroph and the gut-brain axis. So, there is indeed a possibility that ghrelin corticotroph function, influence on the pituitary gonadal axis, analogs, acting as either agonists or antagonists, might have stimulation of appetite, control of energy balance, influence clinical impact. -

Clinical Commissioning Policy: Susoctocog Alfa for Treating Bleeding Episodes in People with Acquired Haemophilia a (All Ages)
Clinical Commissioning Policy: Susoctocog alfa for treating bleeding episodes in people with acquired haemophilia A (all ages) NHS England Reference: 170061P 1 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy Finance Publications Gateway Reference: 07603 Document Purpose Policy Clinical commissioning policy: Susoctocog alfa for treating bleeding Document Name episodes in people with acquired haemophilia A (all ages) Author Specialised Commissioning Team Publication Date 29 June 2018 Target Audience CCG Clinical Leaders, Care Trust CEs, Foundation Trust CEs , Medical Directors, Directors of PH, Directors of Nursing, NHS England Regional Directors, NHS England Directors of Commissioning Operations, Directors of Finance, NHS Trust CEs Additional Circulation #VALUE! List Description Routinely Commissioned - NHS England will routinely commission this specialised treatment in accordance with the criteria described in this policy. Cross Reference 0 Superseded Docs 0 (if applicable) Action Required 0 Timing / Deadlines By 00 January 1900 (if applicable) Contact Details for [email protected] further information 0 0 0 0 0 0 Document Status This is a controlled document. Whilst this document may be printed, the electronic version posted on the intranet is the controlled copy. Any printed copies of this document are not controlled. As a controlled document, this document should not be saved onto local or network drives but should always be accessed from the intranet. 2 Standard Operating Procedure: Clinical Commissioning Policy: Susoctocog alfa for treating bleeding episodes in people with acquired haemophilia A (all ages) First published: June 2018 Prepared by the National Institute for Health and Care Excellence (NICE) Commissioning Support Programme Published by NHS England, in electronic format only. -

Somatostatin Analogues in the Treatment of Neuroendocrine Tumors: Past, Present and Future
International Journal of Molecular Sciences Review Somatostatin Analogues in the Treatment of Neuroendocrine Tumors: Past, Present and Future Anna Kathrin Stueven 1, Antonin Kayser 1, Christoph Wetz 2, Holger Amthauer 2, Alexander Wree 1, Frank Tacke 1, Bertram Wiedenmann 1, Christoph Roderburg 1,* and Henning Jann 1 1 Charité, Campus Virchow Klinikum and Charité, Campus Mitte, Department of Hepatology and Gastroenterology, Universitätsmedizin Berlin, 10117 Berlin, Germany; [email protected] (A.K.S.); [email protected] (A.K.); [email protected] (A.W.); [email protected] (F.T.); [email protected] (B.W.); [email protected] (H.J.) 2 Charité, Campus Virchow Klinikum and Charité, Campus Mitte, Department of Nuclear Medicine, Universitätsmedizin Berlin, 10117 Berlin, Germany; [email protected] (C.W.); [email protected] (H.A.) * Correspondence: [email protected]; Tel.: +49-30-450-553022 Received: 3 May 2019; Accepted: 19 June 2019; Published: 22 June 2019 Abstract: In recent decades, the incidence of neuroendocrine tumors (NETs) has steadily increased. Due to the slow-growing nature of these tumors and the lack of early symptoms, most cases are diagnosed at advanced stages, when curative treatment options are no longer available. Prognosis and survival of patients with NETs are determined by the location of the primary lesion, biochemical functional status, differentiation, initial staging, and response to treatment. Somatostatin analogue (SSA) therapy has been a mainstay of antisecretory therapy in functioning neuroendocrine tumors, which cause various clinical symptoms depending on hormonal hypersecretion. Beyond symptomatic management, recent research demonstrates that SSAs exert antiproliferative effects and inhibit tumor growth via the somatostatin receptor 2 (SSTR2). -

Human and Recombinat Coagulation Factor VIII
08 July 2016 EMA/PRAC/471535/2016 PRAC List of questions To be addressed by the marketing authorisation holder(s) for human and recombinant coagulation factor VIII containing medicinal products Referral under Article 31 of Directive 2001/83/EC resulting from pharmacovigilance data Procedure number: EMEA/H/A-31/1448 Advate EMEA/H/C/0520/A31/0078 Elocta EMEA/H/C/3964/A31/0006 Helixate Nexgen EMEA/H/C/0276/A31/0178 Iblias EMEA/H/C/4147/A31/0002 Kogenate EMEA/H/C/0275/A31/0185 Kovaltry EMEA/H/C/3825/A31/0004 Novoeight EMEA/H/C/2719/A31/0014 Nuwiq EMEA/H/C/2813/A31/0015 Obizur EMEA/H/C/2792/A31/0003 Refacto AF EMEA/H/C/0232/A31/0134 Voncento EMEA/H/C/2493/A31/0022 Active substances: human coagulation factor VIII; efmoroctocog alfa; moroctocog alfa; octocog alfa; simoctocog alfa; susoctocog alfa; turoctocog alfa 30 Churchill Place ● Canary Wharf ● London E14 5EU ● United Kingdom Telephone +44 (0)20 3660 6000 Facsimile +44 (0)20 3660 5555 Send a question via our website www.ema.europa.eu/contact An agency of the European Union © European Medicines Agency, 2016. Reproduction is authorised provided the source is acknowledged. 1. Background Today’s standard treatment of congenital haemophilia (and acquired haemophilia A) is based on prophylactic or on-demand replacement therapy with coagulation factor VIII (FVIII), either with plasma derived or with recombinant FVIII products. Principally both substance classes may be used for prophylactic treatment as well as for therapeutic treatment in case of spontaneous bleedings. Inhibitor development in haemophilia A patients receiving FVIII products mostly occurs in previously untreated or minimally treated patients (PUPs), who are still within the first 50 days of exposure to the treatment. -

WO 2016/133483 Al 25 August 2016 (25.08.2016) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization I International Bureau (10) International Publication Number (43) International Publication Date WO 2016/133483 Al 25 August 2016 (25.08.2016) P O P C T (51) International Patent Classification: SHENIA, Iaroslav Viktorovych [UA/UA]; Feodosiyskyy A61L 15/44 (2006.01) A61L 26/00 (2006.01) lane, 14-a, kv. 65, Kyiv, 03028 (UA). A61L 15/54 (2006.01) (74) Agent: BRAGARNYK, Oleksandr Mykolayovych; str. (21) International Application Number: Lomonosova, 60/5-43, Kyiv, 03189 (UA). PCT/UA20 16/0000 19 (81) Designated States (unless otherwise indicated, for every (22) International Filing Date: kind of national protection available): AE, AG, AL, AM, 15 February 2016 (15.02.2016) AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, (25) Filing Language: English DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (26) Publication Language: English HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, MG, (30) Priority Data: MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, a 2015 01285 16 February 2015 (16.02.2015) UA PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, SC, u 2015 01288 16 February 2015 (16.02.2015) UA SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, (72) Inventors; and TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. -
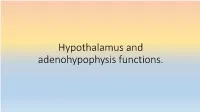
Prezentace Aplikace Powerpoint
Hypothalamus and adenohypophysis functions. Neuroendocrine regulation THALAMUS - NON-SPECIFIC NUCLEI - SPECIFIC SENSORY NUCLEI - SPECIFIC NONSENSORY NUCLEI - ASSOCIATION NUCLEI HYPOTHALAMUS - SYSTEM OF SEVERAL DOZENS OF NUCLEI - PARAVENTRICULAR - MEDIAL - LATERAL REGION HYPOPHYSIS - PARS DISTALIS (STH, PRL, TSH, FSH, LH,ACTH) - PARS TUBERALIS (FSH, LH) - PARS INTERMEDIA (MSH) Behavior Ventrolateral medulla Hypothalamus (heart, stomach) Body temperature regulation Amygdala Neuroendocrine (associative regions of neocortex, regulation olfactory bulb, hippocampal formation, subcortical structures Appetitive behavior including brain stem) (hunger, thirst, sexual behavior) Hippocampus (associative regions of neocortex, Defensive reactions thalamus, reticular formation nuclei, etc.) Biorhythms and their regulation Nucleus solitarius (viscerosensory information– Autonomic nervous heart, lungs, GIT, blood vessels – system (modulation) baro-/chemoreceptors) Locus coeruleus (prefrontal cortex, N. Lamina terminalis Orbitofrontal cortex paragigantocellularis – integration of external and (blood, blood (sensory perception, reaction to composition) reward/punishment) autonomic stimuli – stress, panic) Circumventricular organs Eminentia mediana Subfornical organ Subcommissural organ - Afferent sensoric organ - Body fluid homeostasis - Mainly unknown function - Functional connection of - Blood pressure regulation (R for ANP and ATII) - R for neuropeptides and hypothalamus and hypophysis - Oxytocin secretion regulation neurotransmitters - Point of entry -

Annual Report 2016
Annexes to the annual report of the European Medicines Agency 2016 Annex 1 – Members of the Management Board ............................................................... 2 Annex 2 - Members of the Committee for Medicinal Products for Human Use ...................... 4 Annex 3 – Members of the Pharmacovigilance Risk Assessment Committee ........................ 6 Annex 4 – Members of the Committee for Medicinal Products for Veterinary Use ................. 8 Annex 5 – Members of the Committee on Orphan Medicinal Products .............................. 10 Annex 6 – Members of the Committee on Herbal Medicinal Products ................................ 12 Annex 7 – Committee for Advanced Therapies .............................................................. 14 Annex 8 – Members of the Paediatric Committee .......................................................... 16 Annex 9 – Working parties and working groups ............................................................ 18 Annex 10 – CHMP opinions: initial evaluations and extensions of therapeutic indication ..... 24 Annex 10a – Guidelines and concept papers adopted by CHMP in 2016 ............................ 25 Annex 11 – CVMP opinions in 2016 on medicinal products for veterinary use .................... 33 Annex 11a – 2016 CVMP opinions on extensions of indication for medicinal products for veterinary use .......................................................................................................... 39 Annex 11b – Guidelines and concept papers adopted by CVMP in 2016 ........................... -

Therapeutics Advisory Group
Therapeutics Advisory Group CCG and NHS Trusts in Norfolk and Waveney Index of TAG recommendations Generic name Indication BNFclass Trafficlight IQoro euromuscular training Hiatus hernia - improving symptoms No BNF entry - device Double Red Not recommended for device routine use / Not commissioned (L-) Carnitine Carnitine Deficiency 9.8.1 Drugs used in Red Hospital / Specialist metabolic disorders only (Para-)aminosalicylic acid Tuberculosis 5.1.9 Antituberculosis Double Red Not recommended for drugs - routine use / Not Antimycobacterials commissioned 5-fluorouracil + salicyclic acid Hyperkeratotic actinic keratosis 13.8.1 Photodamage Double-GreenSuitable for GPs to topical solution initiate and prescribe 5-fluorouracil 5% w/w cream Non-hypertrophic actinic keratosis 13.8.1 Photodamage Double-GreenSuitable for GPs to initiate and prescribe Abacavir HIV infection in combination with other 5.3.1 HIV Infection Red Hospital / Specialist antiretroviral drugs only Abacavir + dolutegravir + HIV infection in combination with other 5.3.1 HIV Infection Red Hospital / Specialist lamivudine antiretroviral drugs only Abacavir and lamivudine HIV infection in combination with other 5.3.1 HIV Infection Red Hospital / Specialist antiretroviral drugs only Abaloparatide Male and juvenile osteoporosis 6.6.1 Calcitonin and Double Red Not recommended for Calcitonin and routine use / Not parathyroid hormone commissioned Abatacept Rheumatoid arthritis - 1st line biologic 10.1.3 Drugs that suppress Red Hospital / Specialist after failure of non-biologic DMARDs -
![Ehealth DSI [Ehdsi V2.2.2-OR] Ehealth DSI – Master Value Set](https://docslib.b-cdn.net/cover/8870/ehealth-dsi-ehdsi-v2-2-2-or-ehealth-dsi-master-value-set-1028870.webp)
Ehealth DSI [Ehdsi V2.2.2-OR] Ehealth DSI – Master Value Set
MTC eHealth DSI [eHDSI v2.2.2-OR] eHealth DSI – Master Value Set Catalogue Responsible : eHDSI Solution Provider PublishDate : Wed Nov 08 16:16:10 CET 2017 © eHealth DSI eHDSI Solution Provider v2.2.2-OR Wed Nov 08 16:16:10 CET 2017 Page 1 of 490 MTC Table of Contents epSOSActiveIngredient 4 epSOSAdministrativeGender 148 epSOSAdverseEventType 149 epSOSAllergenNoDrugs 150 epSOSBloodGroup 155 epSOSBloodPressure 156 epSOSCodeNoMedication 157 epSOSCodeProb 158 epSOSConfidentiality 159 epSOSCountry 160 epSOSDisplayLabel 167 epSOSDocumentCode 170 epSOSDoseForm 171 epSOSHealthcareProfessionalRoles 184 epSOSIllnessesandDisorders 186 epSOSLanguage 448 epSOSMedicalDevices 458 epSOSNullFavor 461 epSOSPackage 462 © eHealth DSI eHDSI Solution Provider v2.2.2-OR Wed Nov 08 16:16:10 CET 2017 Page 2 of 490 MTC epSOSPersonalRelationship 464 epSOSPregnancyInformation 466 epSOSProcedures 467 epSOSReactionAllergy 470 epSOSResolutionOutcome 472 epSOSRoleClass 473 epSOSRouteofAdministration 474 epSOSSections 477 epSOSSeverity 478 epSOSSocialHistory 479 epSOSStatusCode 480 epSOSSubstitutionCode 481 epSOSTelecomAddress 482 epSOSTimingEvent 483 epSOSUnits 484 epSOSUnknownInformation 487 epSOSVaccine 488 © eHealth DSI eHDSI Solution Provider v2.2.2-OR Wed Nov 08 16:16:10 CET 2017 Page 3 of 490 MTC epSOSActiveIngredient epSOSActiveIngredient Value Set ID 1.3.6.1.4.1.12559.11.10.1.3.1.42.24 TRANSLATIONS Code System ID Code System Version Concept Code Description (FSN) 2.16.840.1.113883.6.73 2017-01 A ALIMENTARY TRACT AND METABOLISM 2.16.840.1.113883.6.73 2017-01 -
Australian Public Assessment Report for Lonoctocog Alfa (Rch)
Australian Public Assessment Report for lonoctocog alfa (rch) Proprietary Product Name: Afstyla Sponsor: CSL Behring Australia Pty Ltd January 2018 Therapeutic Goods Administration About the Therapeutic Goods Administration (TGA) · The Therapeutic Goods Administration (TGA) is part of the Australian Government Department of Health and is responsible for regulating medicines and medical devices. · The TGA administers the Therapeutic Goods Act 1989 (the Act), applying a risk management approach designed to ensure therapeutic goods supplied in Australia meet acceptable standards of quality, safety and efficacy (performance) when necessary. · The work of the TGA is based on applying scientific and clinical expertise to decision- making, to ensure that the benefits to consumers outweigh any risks associated with the use of medicines and medical devices. · The TGA relies on the public, healthcare professionals and industry to report problems with medicines or medical devices. TGA investigates reports received by it to determine any necessary regulatory action. · To report a problem with a medicine or medical device, please see the information on the TGA website <https://www.tga.gov.au>. About AusPARs · An Australian Public Assessment Report (AusPAR) provides information about the evaluation of a prescription medicine and the considerations that led the TGA to approve or not approve a prescription medicine submission. · AusPARs are prepared and published by the TGA. · An AusPAR is prepared for submissions that relate to new chemical entities, generic medicines, major variations and extensions of indications. · An AusPAR is a static document; it provides information that relates to a submission at a particular point in time. · A new AusPAR will be developed to reflect changes to indications and/or major variations to a prescription medicine subject to evaluation by the TGA. -

Dietary Supplements Compendium Volume 1
2015 Dietary Supplements Compendium DSC Volume 1 General Notices and Requirements USP–NF General Chapters USP–NF Dietary Supplement Monographs USP–NF Excipient Monographs FCC General Provisions FCC Monographs FCC Identity Standards FCC Appendices Reagents, Indicators, and Solutions Reference Tables DSC217M_DSCVol1_Title_2015-01_V3.indd 1 2/2/15 12:18 PM 2 Notice and Warning Concerning U.S. Patent or Trademark Rights The inclusion in the USP Dietary Supplements Compendium of a monograph on any dietary supplement in respect to which patent or trademark rights may exist shall not be deemed, and is not intended as, a grant of, or authority to exercise, any right or privilege protected by such patent or trademark. All such rights and privileges are vested in the patent or trademark owner, and no other person may exercise the same without express permission, authority, or license secured from such patent or trademark owner. Concerning Use of the USP Dietary Supplements Compendium Attention is called to the fact that USP Dietary Supplements Compendium text is fully copyrighted. Authors and others wishing to use portions of the text should request permission to do so from the Legal Department of the United States Pharmacopeial Convention. Copyright © 2015 The United States Pharmacopeial Convention ISBN: 978-1-936424-41-2 12601 Twinbrook Parkway, Rockville, MD 20852 All rights reserved. DSC Contents iii Contents USP Dietary Supplements Compendium Volume 1 Volume 2 Members . v. Preface . v Mission and Preface . 1 Dietary Supplements Admission Evaluations . 1. General Notices and Requirements . 9 USP Dietary Supplement Verification Program . .205 USP–NF General Chapters . 25 Dietary Supplements Regulatory USP–NF Dietary Supplement Monographs . -

Dossier Zur Nutzenbewertung Gemäß § 35A SGB V
Dokumentvorlage, Version vom 16.08.2018 Dossier zur Nutzenbewertung gemäß § 35a SGB V Turoctocog alfa pegol (Esperoct®) Novo Nordisk Pharma GmbH Modul 3 A Behandlung und Prophylaxe von Blutungen bei Patienten im Alter von 12 Jahren und älter mit Hämophilie A (angeborener Faktor VIII-Mangel). Zweckmäßige Vergleichstherapie, Anzahl der Patienten mit therapeutisch bedeutsamem Zusatznutzen, Kosten der Therapie für die GKV, Anforderungen an eine qualitätsgesicherte Anwendung Stand: 30.07.2019 Dossier zur Nutzenbewertung – Modul 3 A Stand: 30.07.2019 Vergleichstherapie, Patienten mit therap. bedeutsamem Zusatznutzen, Kosten, qualitätsgesicherte Anwendung Inhaltsverzeichnis Seite Tabellenverzeichnis .................................................................................................................. 2 Abbildungsverzeichnis ............................................................................................................. 4 Abkürzungsverzeichnis ............................................................................................................ 5 3 Modul 3 – allgemeine Informationen ............................................................................ 7 3.1 Bestimmung der zweckmäßigen Vergleichstherapie .................................................... 8 3.1.1 Benennung der zweckmäßigen Vergleichstherapie ................................................ 9 3.1.2 Begründung für die Wahl der zweckmäßigen Vergleichstherapie .......................... 9 3.1.3 Beschreibung der Informationsbeschaffung für Abschnitt