Feigned Illness and Bodily Legibility in Eighteenth- Century British Culture
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bringing Richard Brome Online
This is a repository copy of Bringing Richard Brome Online. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/105805/ Version: Published Version Article: Hirsch, BD orcid.org/0000-0002-6231-2080 (2010) Bringing Richard Brome Online. Early Theatre, 13 (1). pp. 137-153. ISSN 1206-9078 10.12745/et.13.1.837 This article is protected by copyright. Reproduced in accordance with the publisher's self-archiving policy. Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Early Theatre Volume 13, Issue 1 2010 Article 7 Bringing Richard Brome Online Brett D. Hirsch∗ ∗University of Western Australia, [email protected] Copyright c 2010 by Early Theatre. Early Theatre is produced by The Berkeley Electronic Press (bepress). http://digitalcommons.mcmaster.ca/earlytheatre Bringing Richard Brome Online Brett D. Hirsch Abstract This review essay assesses Richard Brome Online, an online edition of the collected works of Richard Brome, in terms of the design, functionality, and usability of its features. -

Some Psychoanalytical Meanings of the Skin in the Book of Job
Verbum et Ecclesia ISSN: (Online) 2074-7705, (Print) 1609-9982 Page 1 of 8 Original Research Some psychoanalytical meanings of the skin in the book of Job Author: Traditionally, there has been a tension between psychology and religion because of the 1 Pieter van der Zwan Freudian critique of religion. This research intends to show that a deeper understanding of Affiliation: religion leading hopefully to an even deeper religiosity can be achieved by studying bodily 1Department of Old features portrayed in a (religious) text from a psychoanalytic perspective. Just as any literary Testament Studies, University character can be ‘psychoanalysed’ to produce new perspectives on it and on the narrative as a of Pretoria, South Africa whole, the personality of Job invites the postmodern reader to continue understanding this Corresponding author: book on new levels. From this approach, it becomes clear that the protagonist struggles with Pieter van der Zwan, boundaries and individuation because of his depressive tendencies experienced in issues with [email protected] reality’s harsh touch, nakedness and distance. Dates: Intradisciplinary and/or interdisciplinary implications: Just as any literary character can be Received: 09 May 2016 ‘psychoanalysed’ to produce new perspectives on it and on the narrative as a whole, the Accepted: 01 Aug. 2017 Published: 21 Sept. 2017 personality of Job invites the postmodern reader to continue understanding this book on new levels. From this approach, it becomes clear that the protagonist struggles with boundaries How to cite this article: and individuation because of his depressive tendencies experienced in issues with reality’s Van der Zwan, P., 2017, ‘Some harsh touch, nakedness and distance. -

This Electronic Thesis Or Dissertation Has Been Downloaded from the King’S Research Portal At
This electronic thesis or dissertation has been downloaded from the King’s Research Portal at https://kclpure.kcl.ac.uk/portal/ Inimitable? The Afterlives and Cultural Memory of Charles Dickens’s Characters England, Maureen Bridget Awarding institution: King's College London The copyright of this thesis rests with the author and no quotation from it or information derived from it may be published without proper acknowledgement. END USER LICENCE AGREEMENT Unless another licence is stated on the immediately following page this work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International licence. https://creativecommons.org/licenses/by-nc-nd/4.0/ You are free to copy, distribute and transmit the work Under the following conditions: Attribution: You must attribute the work in the manner specified by the author (but not in any way that suggests that they endorse you or your use of the work). Non Commercial: You may not use this work for commercial purposes. No Derivative Works - You may not alter, transform, or build upon this work. Any of these conditions can be waived if you receive permission from the author. Your fair dealings and other rights are in no way affected by the above. Take down policy If you believe that this document breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Download date: 08. Oct. 2021 1 INIMITABLE? THE AFTERLIVES AND CULTURAL MEMORY OF CHARLES DICKENS’S CHARACTERS Maureen Bridget England King’s College London Candidate Number: 1233164 Thesis for PhD in English Literature 2 This paper is dedicated to the two doctors in my life who inspired me to pursue this dream: Martin England and Jenna Higgins 3 ‘Any successfully evoked character, no matter how apparently insignificant, stands a good chance of surviving its creator.’ David Galef, The Supporting Cast (1993) 4 Table of Contents TABLE OF CONTENTS ........................................................................................................ -

Etherology, Or, the Philosophy of Mesmerism
TUFTS COLLEGE Tufts College Library « PHRENOLOG1.0AL BUST. See Page 164. • E THEE 0 LOG Y; OR, THE PHILOSOPHY OF MESMERISM . AND PHRENOLOGY: INCLUDING A NEW PHILOSOPHY OF SLEEP AND OF CONSCIOUSNESS, WITH A REVIEW OF THE PRETENSIONS OF NEUROLOGY AND PHRENO-MAGNETISM BY J. STANLEY GRIMES, COUNSELLOR AT LAW, FORMERLY PRESIDENT OF THE WESTERN PHRENOLOGICAL SOCIETY, PROFESSOR OF MEDICAL JURISPRUDENCE IN THE CASTLETON MEDICAL COLLEGE AND AUTHOR OF 4 A NEW SYSTEM OF PHRENOLOGY.' All the known phenomena of the universe may he referred to three general princi- ples, viz.: Matter, Motion, and Consciousness.—p. 17. NEW YORK: SAXTON AND MILES, NO. 205 BROADWAY PHILADELPHIA :-J AMES M. CAMPBELL. BOSTON I SAXTON, PEIRCE & CO. 1845. year by Entered according to Act of Congress, in the 1845, J. STANLEY GRIMES, the Southern District In the Clerk's Office of the District Court of of New York. 1 i m CONTENTS. SECTION I. page. SYNOFSIS OF ETHEROLOGY . 17 SECTION II. HISTORY OF ETHERIUM ..... 39 Ignorance of the Ancients concerning the causes of Ethe- rean Phenomena — Witchcraft — Divination — Magic — Discoveries which led to a Scientific Knowledge of Ethe- ropathy—Van Helmot—Mesmer—His Career—D'Eslon —Adverse Report of the French Commissioners—Foissac and the Academy of Medicine—Their favorable report —Gall—La Place. SECTION III. NATURE OF ETHERIUM ..... 75 Theory of Light—Of Heat—Of Electricity—Of Magnetism— Of Gravitation—Newton's Conjecture—Rev. Mr. Town- shend on the Mesmeric Medium—Sunderland's Notions —Animal Electricity—Experiments of Crosse—Electric Fishes. SECTION IV. OXYGEN ........ 127 SECTION V. PHILOSOPHY OF SLEEP 130 Liebig's Error. -

Los Viajes Del Caballero Inglés John Breval a España Y Portugal: Novedades Arqueológicas Y Epigráficas De 1726
Los viajes del caballero inglés John Breval a España y Portugal: novedades arqueológicas y epigráficas de 1726 ALICIA M.ª CANTO* Amicus Plato, sed magis amica veritas (Arist., Nicom. I, 4; Cerv., Quixot., 2.51) RESUMENLa accidentada vida del caballero John D. Breval (c. 1680-1738), clasicista del Tri- nity College de Cambridge, conocido literato inglés y preceptor de nobles en el «Grand Tour», incluyó una etapa como militar y hombre de confianza del Duque de Marlborough. Como militar y preceptor, viajó al sur de Portugal y España en tres ocasiones, entre 1708 y 1716. A su paso por muchas ciudades del Alentejo y Andalucía tomó múltiples notas sobre sus anti- güedades y copió 49 inscripciones romanas, la mayor parte de las cuales por autopsia. En 1726, al publicar en Londres sus Remarks on several parts of Europe (dedicado al futuro conde de Cholmondeley), incluyó al final sus notas ibéricas, acompañadas de un nutrido aparato de textos antiguos y bibliografía de su época. En este trabajo presentamos, además de algu- nas novedades biográficas sobre el autor, la traducción al español de los citados capítulos, acompañada de nuestro estudio crítico. Los epígrafes y los detalles sobre ellos que transmite Breval resultan ser un valioso testimonio para nuevas lecturas, consideración de falsos como auténticos, etc. Nuestra investigación sirve, pues, para devolver a John D. Breval su buen cré- dito como transmisor de inscripciones romanas (damnatus por Theodor Mommsen y Emil Hübner en el CIL II), y junto con él también el del gran humanista portugués Andrés de Resende, muchas veces tachado de falsario, a nuestro juicio injustamente. -

Front Matter
Cambridge University Press 978-0-521-19584-3 - Thomas Betterton: The Greatest Actor of the Restoration Stage David Roberts Frontmatter More information THOMAS BETTERTON Restoration London’s leading actor and theatre manager Thomas Betterton has not been the subject of a biography since 1891. He worked with all the best-known playwrights of his age and with the first generation of English actresses; he was intimately involved in the theatre’s responses to politics, and became a friend of leading literary men such as Pope and Steele. His innovations in scenery and company management, and his association with the dramatic inher- itance of Shakespeare, helped to change the culture of English thea- tre. David Roberts’s entertaining study unearths new documents and draws fresh conclusions about this major but shadowy figure. It con- textualises key performances and examines Betterton’s relationship to patrons, colleagues and family, as well as to significant historical moments and artefacts. The most substantial study available of any seventeenth-century actor, Thomas Betterton gives one of England’s greatest performing artists his due on the tercentenary of his death. dav id roberts is Professor and Head of English at Birmingham City University. His previous publications include The Ladies: Female Patronage of Restoration Drama (1989) and editions of Defoe’s Colonel Jack, A Journal of the Plague Year and Lord Chesterfield’s letters. His articles and reviews have appeared in leading journals including Shakespeare Quarterly, The Review of English Studies, ELH, The Times Literary Supplement and New Theatre Quarterly. © in this web service Cambridge University Press www.cambridge.org Cambridge University Press 978-0-521-19584-3 - Thomas Betterton: The Greatest Actor of the Restoration Stage David Roberts Frontmatter More information Letter from Thomas Betterton to Colonel Finch, steward to Thomas Thynne, Lord Weymouth, in Longleat House, Thynne Papers, vol. -

Volume 4 2014
2101 EAST COLISEUM BOULEVARD FORT WAYNE, IN 46805-1499 Volume 4 2014 Volume Volume 4 2014 Volume 4 2014 EDITORS at Indiana University– at Mount St. Mary’s University Purdue University Fort Wayne Emmitsburg, Maryland M. L. Stapleton, Editor Sarah K. Scott, Associate Editor Cathleen M. Carosella, Managing Editor Jessica Neuenschwander, Pub. Assistant BOARD OF ADVISORS Hardin Aasand, Indiana University–Purdue University, Fort Wayne; David Bevington, University of Chicago; Douglas Bruster, University of Texas, Austin; Dympna Callaghan, Syracuse University; Patrick Cheney, Pennsylvania State University; Sara Deats, University of South Florida; J. A. Downie, Goldsmiths College, University of London; Lisa M. Hopkins, Sheffield Hallam University; Heather James, University of Southern California; Roslyn L. Knutson, University of Arkansas, Little Rock; Robert A. Logan, University of Hartford; Ruth Lunney, University of Newcastle (Australia); Laurie Maguire, Magdalen College, Oxford University; Lawrence Manley, Yale University; Kirk Melnikoff, University of North Carolina at Charlotte; Paul Menzer, Mary Baldwin College; John Parker, University of Virginia; Eric Rasmussen, University of Nevada, Reno; David Riggs, Stanford University; John P. Rumrich, University of Texas, Austin; Carol Chillington Rutter, University of Warwick; Paul Werstine, King's College, University of Western Ontario; Charles Whitney, University of Nevada, Las Vegas Marlowe Studies: An Annual is a journal devoted to studying Christopher Marlowe and his role in the literary culture of his time, including but not limited to studies of his plays and poetry; their sources; relations to genre; lines of influence; classical, medieval, and continental contexts; performance and theater history; textual studies; the author’s professional milieu and place in early modern English poetry, drama, and culture. -
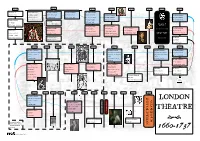
An A2 Timeline of the London Stage Between 1660 and 1737
1660-61 1659-60 1661-62 1662-63 1663-64 1664-65 1665-66 1666-67 William Beeston The United Company The Duke’s Company The Duke’s Company The Duke’s Company @ Salisbury Court Sir William Davenant Sir William Davenant Sir William Davenant Sir William Davenant The Duke’s Company The Duke’s Company & Thomas Killigrew @ Salisbury Court @Lincoln’s Inn Fields @ Lincoln’s Inn Fields Sir William Davenant Sir William Davenant Rhodes’s Company @ The Cockpit, Drury Lane @ Red Bull Theatre @ Lincoln’s Inn Fields @ Lincoln’s Inn Fields George Jolly John Rhodes @ Salisbury Court @ The Cockpit, Drury Lane @ The Cockpit, Drury Lane The King’s Company The King’s Company PLAGUE The King’s Company The King’s Company The King’s Company Thomas Killigrew Thomas Killigrew June 1665-October 1666 Anthony Turner Thomas Killigrew Thomas Killigrew Thomas Killigrew @ Vere Street Theatre @ Vere Street Theatre & Edward Shatterell @ Red Bull Theatre @ Bridges Street Theatre @ Bridges Street Theatre @ The Cockpit, Drury Lane @ Bridges Street Theatre, GREAT FIRE @ Red Bull Theatre Drury Lane (from 7/5/1663) The Red Bull Players The Nursery @ The Cockpit, Drury Lane September 1666 @ Red Bull Theatre George Jolly @ Hatton Garden 1676-77 1675-76 1674-75 1673-74 1672-73 1671-72 1670-71 1669-70 1668-69 1667-68 The Duke’s Company The Duke’s Company The Duke’s Company The Duke’s Company Thomas Betterton & William Henry Harrison and Thomas Henry Harrison & Thomas Sir William Davenant Smith for the Davenant Betterton for the Davenant Betterton for the Davenant @ Lincoln’s Inn Fields -

Gesture and Movement in Silent Shakespeare Films
Gesticulated Shakespeare: Gesture and Movement in Silent Shakespeare Films Thesis Presented in Partial Fulfillment of the Requirements for the Degree of Master of Arts in the Graduate School of The Ohio State University By Jennifer Rebecca Collins, B.A. Graduate Program in Theatre The Ohio State University 2011 Thesis Committee: Alan Woods, Advisor Janet Parrott Copyright by Jennifer Rebecca Collins 2011 Abstract The purpose of this study is to dissect the gesticulation used in the films made during the silent era that were adaptations of William Shakespeare's plays. In particular, this study investigates the use of nineteenth and twentieth century established gesture in the Shakespearean film adaptations from 1899-1922. The gestures described and illustrated by published gesture manuals are juxtaposed with at least one leading actor from each film. The research involves films from the experimental phase (1899-1907), the transitional phase (1908-1913), and the feature film phase (1912-1922). Specifically, the films are: King John (1899), Le Duel d'Hamlet (1900), La Diable et la Statue (1901), Duel Scene from Macbeth (1905), The Taming of the Shrew (1908), The Tempest (1908), A Midsummer Night's Dream (1909), Il Mercante di Venezia (1910), Re Lear (1910), Romeo Turns Bandit (1910), Twelfth Night (1910), A Winter's Tale (1910), Desdemona (1911), Richard III (1911), The Life and Death of King Richard III (1912), Romeo e Giulietta (1912), Cymbeline (1913), Hamlet (1913), King Lear (1916), Hamlet: Drama of Vengeance (1920), and Othello (1922). The gestures used by actors in the films are compared with Gilbert Austin's Chironomia or A Treatise on Rhetorical Delivery (1806), Henry Siddons' Practical Illustrations of Rhetorical Gesture and Action; Adapted to The English Drama: From a Work on the Subject by M. -

Scripted Improvisation in the Antipodes
ISSUES IN REVIEW 129 ‘Now mark that fellow; he speaks Extempore’: Scripted Improvisation in The Antipodes Concluding his near-paraphrase of Hamlet’s famous advice to the players, Letoy in Richard Brome’s The Antipodes chastises Byplay, an actor with a penchant for improvisation, with the following lines: But you, sir, are incorrigible, and Take license to yourself to add unto Your parts your own free fancy, and sometimes To alter or diminish what the writer With care and skill compos’d; and when you are To speak to your coactors in the scene, You hold interlocutions with the audients— (2.1.93–9)1 Unlike the silent company Hamlet addresses, whose leader assents to Hamlet’s presumptuous lessons with only ‘I warrant your honour’ and a slightly more defensive ‘I hope we have reformed that indifferently with us, sir’ (3.2.13, 30),2 Byplay argues back saying, ‘That is a way, my lord, has been allowed / On elder stages to move mirth and laughter.’ ‘Yes’, Letoy replies, ‘in the days of Tarlton and Kemp, / Before the stage was purged from barbarism, / And brought to the perfection it now shines with’ (2.1.100–4) . Scholars often acknowledge, like Letoy, that improvisation played a signifi- cant role in early English theatre. Actors playing Vice characters in Tudor the- atre improvised before and after the plays in which they performed.3 Renais- sance texts contain stage directions instructing actors to improvise—Greene’s Tu Quoque (1611), for example, includes a direction for characters to ‘talk and rail what they list’ and The Trial of Chivalry (1601) contains the remark- able direction, ‘speaks anything, and Exit’.4 Elizabethan clowns, and in par- ticular Richard Tarlton and William Kemp, were famous for their ability to improvise. -

Two Augustan Booksellers
Two Augustan Booksellers JOHN DUNTON and EDMUND CURLL Peter Murray Bill UNIVERSITY OF KANSAS LIBRARIES LAWRENCE, KANSAS 1958 © 1959 UNIVERSITY OF KANSAS LIBRARIES Library of Congress Catalog Card Number 58-63057 PRINTED BY THE UNIVERSITY OF KANSAS PRESS Preface In 1952 a new Chancellor and a new Director of Libraries at the University of Kansas, Franklin D. Mur• phy and Robert Vosper, came together to institute a re• vitalized program of enrichment and growth of the uni• versity libraries. One of the products of the program was the early establishment of a public lectureship on books and bibliography. In subsequent years five distinguished exponents of as many different kinds of bibliophily have visited the Lawrence campus to talk about books and bibliography. The choice of lecturers has been fortunate; all have had something to say. The present publication indicates clearly the further conviction that what the lecturers said was not only worth hearing in Kansas but is also worth reading and rereading anywhere. The University of Kansas' Annual Public Lectures on Books and Bibliography are listed overleaf. The pur• poses of the list are three: (1) To identify each of the five lectures presented up to 1958; (2) To delineate explicitly the peculiar facts of publication of the second, third, and fourth lectures within the Library Series of the Univer• sity of Kansas Publications; and thereby (3) To allow colleagues in other institutions to escape some of the ex• asperation induced by publication of parts of one series within another series. A separate list of the entire Library Series is printed inside the front cover of the present vol• ume. -

The Famous Ballads of Anna Gordon, Mrs
The Famous Ballads of Anna Gordon, Mrs. Brown (Book Chapter) The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Perry, Ruth. "The Famous Ballads of Anna Gordon, Mrs. Brown." Book Chapter in Volume Four: A Cultural History of Women in the Age of Enlightenment, Edited by Ellen Pollak, Michigan State University, USA, 2012. (A Cultural History of Women, 6 Volume Set, ed. by Linda Kalof) As Published http://www.bergpublishers.com/?TabId=15134 Publisher Berg Publishers Version Author's final manuscript Citable link http://hdl.handle.net/1721.1/69940 Terms of Use Creative Commons Attribution-Noncommercial-Share Alike 3.0 Detailed Terms http://creativecommons.org/licenses/by-nc-sa/3.0/ The Famous Ballads of Anna Gordon, Mrs. Brown Ruth Perry, MIT 5/22/2010 When one thinks of the Scottish enlightenment, one imagines men striding up the craggy peak adjoining Holyrood Park in Edinburgh, arguing and gesticulating, or reading one another‟s works by candle light, or sitting over whiskey or beer in largely male company. But there were, of course, women who participated in the intellectual ferment of that period. Among other things, women were an important part of the traditional song culture that interested Scottish intellectuals as the antiquarian remains of a precious national culture. Indeed, as Burns and Scott knew, women were often crucial in transmitting and preserving this stream of Scotland‟s literary history. Thus while learned written and printed investigations were pouring forth from the four universities of Scotland, with reverberations all over the western world, Scottish scholars and philosophers were eagerly collecting and sharing whatever records they could find of a traditional culture that was essentially oral and popular and carried forward 1 largely by working people and occasionally by their own mothers and aunts.