Local Parks in the Howick Local Board Area Column6
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Student Handbook Golflands Campus 2017
Student Handbook Golflands Campus 2017 Table of Contents Pages INTRODUCTION 3 VISION STATEMENT 4 GENERAL AIMS 5 ELIM CHRISTIAN COLLEGE CURRICULUM 6 - 8 Vision Statement/Principles/Arise/Values PARENT COMMITMENT & RESPONSIBILITIES 9 STUDENT GUIDELINES 10 - 15 At school/At home/Mufti Days Before School Rules/ Lunchtime Rules/Playground Rules Expectations for Student Behaviour/Golflands Campus Behaviour Management/Expectations for Classroom Use Digital Citizenship GENERAL INFORMATION AND PROCEDURES 15 - 30 Term Dates/Bell Times/ARISE Parents/Assemblies/BYOD Complaints made against Teachers Emergency Evacuations/Homework/Illness or Accident/Lateness Leave or Absence/Library/Lunches/Messages to Students During School Time Movement To and From School/Newsletter/Office Hours/Parent Involvement Parent-Teacher-Student Conferences Prize Giving Ceremonies/Property/Queries/Reports/School Fees/Donations/School Links/ Stationery Staff Only Days/Student Counsellor/Telephone/The School Day/Toilet Blocks/Uniform - Regula- tion Details/Hair/Uniform Uniform sales/Second hand items/Visitors/Withdrawing from Elim/What to do if… PEOPLE TO KNOW 31 - 33 APPENDICES 34 - 39 Appendix 1 - Procedure: Internet Acceptable Use Appendix 2 - Agreement: Internet Acceptable Use Agreement Appendix 3 - Blended Class/BYOD Agreement Appendix 4 - Student Contract Appendix 5 - A Brief History of Elim Christian College 2 Introduction Welcome to the 2017 school year at Elim Christian College, one school on two sites! We are so glad to have you and your family as part of our school community. In fact this is your school and we look forward to a wonderfully productive partnership. Students I encourage you to allow God to challenge, shape and grow your character this year. It is the depth and quality of your character that will open doors for you, enable you to face hard situations and to help you pursue your dreams. -

Somerville Intermediate School
ARADE Christian Centre 1 RES 2 3 4 5 6 7 8 9 ANMALLOY OA BEACH IVI ESPLANADE V AYLMER K W HOSTE O O CASABELLA COURT ..........E2 GILLETT PLACE .................E2 MEADOWLAND DRIVE ......E3 ROBBIES ROAD ................ D5 D ACCESS R R INDEX DORRINGTON O LAINGS G ADDIS PLACE .................... D5 CASTLEMAINE CLOSE ..... G2 GILNOCKIE CLOSE ........... H2 MELLEFONT CLOSE ......... G2 ROCHESTER CRESCENT.. D3 E R CHALE PLACE ................... D4 GLANWORTH PLACE ....... G2 MELLICK PLACE ................F2 ROSETTA COURT ............. D4 T ADVENE ROAD ................. D4 E EMBLING A CHERRYWOOD GLASSONBY ROAD ...........F1 MERINO AVENUE ...............E3 SAINT ELMO RISE .............F3 K ALEXANDERT STREET ....... D4 A o U ROAD D ALF PLACEa .........................E4 CRESCENT ........................F2 GLASTRY CLOSE ................I1 MICHAEL RICHARD SALE STREET ................... C3 n F o w AVE d e rr n CHIANA PLACE ..................E3 GLENCULLEN PLACE ....... G2 PLACE ............................... H3 SAN JOSE RISE .................F3 I ALICIA ROADW ..................... D3 Schnapper TA y to U a K T A i w CHISBURY TERRACE ........E4 GOLDERS PLACE ............. D3 MIDDLEFIELD DRIVE ..........I1 SANDALWOODRock PLACE ......E3 T h e AMADEUS PLACEn ..............E2 Motukaraka SOMERVILLE e r k m A DR e u CHURCHILL ROAD ............ C4 IslandGOOCH PLACE ..................E3 MILLHOUSE DRIVE ............E2 SANDSPIT ROAD ...............E4 i AMBERWOOD DRIVEn ........F2 I c View Bay a s k PEDERSEN l l a l CLAREMONT WAY ............ H1 GRACECHURCH DRIVE .....I1 MILLISLE PLACE ............... G2 SANTA ANA DRIVE .............F2 AMBLESIDE DRIVEan ............F2 Pohutukawa Tamaki Strait n Tamaki Strait RESERVE d A SEAS SPRAY d CLEARY TERRACE ........... C4 GRANGER ROAD .............. C4 MINERVA TERRACE.......... D3 SANTABay CRUZ DRIVEPOHUTUKAWA ..........F3 A O AMBROSE LANE ............... H4 RR CRES CLIFTON ROAD ..................E7 GRIGGS ROAD ................. -

Teacher Reprimanded for Threat
Officer and his Sallies' appeal dog get bravery for Christmas awards P5 begins P8 Eastern Courier Wednesday, November 23, 2016 ԜϢвыӃ冟ϣФϤнզۡ Magic night of fun Midnight Madness in Howick always draws the crowds and last Friday’s event once again showed off the best the township offers to thousands of party and shopping revellers. More photos, page 4. Teacher reprimandedfor threat CRAIG HOYLE son off at the centre at 9.15am on ‘‘Watch your back, as I know where you a relatively lengthy career, and June 19. that she was held in sufficient pro- An early childhood teacher has However, the drop-off time was and your son live.’’ fessional regard by Kauri Kids to been censured for serious miscon- changed to 8.30am in the centre’s be promoted to head teacher’’. duct after she threatened the records, meaning the mother was backed up by other staff dren and bullied other staff, and The tribunal ordered her to mother of a young child. would have been charged for members who were nearby at the that she had allowed a teacher to complete a professional develop- Ngametuaangai Tuaputa, the additional time. time. She later laid a complaint start working at Kauri Kids ment programme with a focus on former head teacher at Kauri Kids Tuaputa insisted the mother about Tuaputa’s behaviour. before she’d been vetted by police. developing and maintaining centre in Howick, told the mother: had actually dropped her son off The committee uncovered a The NZ Teachers Disciplinary respectful relationships. It ‘‘Watch your back, as I know at 8.30am even after being raft of other allegations against Tribunal decided there was not rejected a submission from the where you and your son live.’’ confronted with CCTV footage Tuaputa when it began enough evidence to support some complaints assessment committee The Education Council’s com- which proved otherwise. -

Alfriston College Aorere College Botany Downs Secondary College
Alfriston College Aorere College Botany Downs Secondary College Bucklands Beach Intermediate School Destiny School Drury School Elim Christian College Howick College Howick Intermediate School Macleans College Manurewa High School Manurewa Intermediate School Maraetai Beach School Otahuhu Intermediate School Pukekohe High School Randwick Park School Saint Kentigern College Somerville Intermediate School Tyndale Park Christian School 1 CONVENOR’S REPORT It gives me great pleasure to be associated with the 2009 MIT Manukau Science and Technology Fair. This is our fifteenth year as a full Regional Fair and we continue the tradition of previous years enthusiastically. For many students the fair provides a platform outside of the confines of the classroom to explore an area of interest. Past award winning participants all agree that their participation and achievements in the fair have helped them to secure a variety of scholarships and prizes, as well as boosting their applications for places in restricted courses at tertiary institutions. The successful award winners tonight represent the best of hundreds of projects in our region from nineteen participating schools. The committee and judges have been very impressed with both the high standard of presentation of work and the ingenious and innovative nature of the investigations undertaken by students. Each exhibit represents hours of toil which often extends over a number of weeks. These projects are in most cases the result of considerable input and guidance from parents and teachers.To produce work of this calibre requires a high quality of teaching and learning – I believe that the work shown here tonight reflects very favourably on the sort of good learning that is taking place in Manukau City classrooms. -
To Botany Town Centre to Bucklands Beach Via Highland Park Via Highland Park
to Botany Town Centre to Bucklands Beach via Highland Park via Highland Park Botany Botany Bucklands BeachHighland Park Town Town Centre Highland Park Bucklands Route (Stop 6163) (Stop 6209) Centre Route (Stop 6231) (Stop 2076) Beach Monday to Friday 545 Monday to Friday 545 AM 545 6.25 6.40 6.55 AM 545 7.00 7.15 7.25 545 6.55 7.10 7.25 545 7.30 7.45 7.55 545 7.25 7.40 7.55 545 8.00 8.15 8.25 545 7.55 8.10 8.25 545 8.30 8.45 8.55 545 8.25 8.40 8.55 545 9.00 9.15 9.25 545 8.55 9.10 9.25 545 9.30 9.45 9.55 545 9.25 9.40 9.55 545 10.00 10.15 10.25 545 9.55 10.10 10.25 545 10.30 10.45 10.55 545 10.25 10.40 10.55 545 11.00 11.15 11.25 545 10.55 11.10 11.25 545 11.30 11.45 11.55 545 11.25 11.40 11.55 PM 545 12.00 12.15 12.25 545 11.55 12.10 12.25 545 12.30 12.45 12.55 PM 545 12.25 12.40 12.55 545 1.00 1.15 1.25 545 12.55 1.10 1.25 545 1.30 1.45 1.55 545 1.25 1.40 1.55 545 2.00 2.15 2.25 545 1.55 2.10 2.25 545 2.30 2.45 2.55 545 2.25 2.40 2.55 545 3.00 3.15 3.25 545 2.55 3.10 3.25 545 3.30 3.45 3.55 545 3.25 3.40 3.55 545 4.00 4.15 4.25 545 3.55 4.10 4.25 545 4.30 4.45 4.55 545 4.25 4.40 4.55 545 5.00 5.15 5.25 545 4.55 5.10 5.25 545 5.30 5.45 5.55 545 5.25 5.40 5.55 545 6.00 6.15 6.25 545 6.30 6.45 6.55 Saturday 545 Saturday 545 AM 545 6.55 7.10 7.25 545 7.55 8.10 8.25 AM 545 7.30 7.45 7.55 545 8.55 9.10 9.25 545 8.30 8.45 8.55 545 9.55 10.10 10.25 545 9.30 9.45 9.55 545 10.55 11.10 11.25 545 10.30 10.45 10.55 545 11.55 12.10 12.25 545 11.30 11.45 11.55 PM 545 12.55 1.10 1.25 PM 545 12.30 12.45 12.55 545 1.55 2.10 2.25 545 1.30 1.45 1.55 545 -

Application Form
Postal Address: PO Box 58 644, Botany, 2163, Auckland Phone: (09)538 0368 Email: [email protected] www.elim.school.nz APPLICATION FORM Please indicate which campus you are applying for: Botany Campus: 159 Botany Road, Botany Downs, 2010, Auckland Years 11-13 Golflands Campus: 94 Golfland Drive, Botany Downs, 2013, Auckland Years 1-10 Mt Albert Campus: 1 McLean Street, Mt Albert, 1025, Auckland Years 1-13 Franklin Campus: Expression of Interest Only Surname of Student: ________________________________ Forenames: _____________________________________________ Proposed Date of Entry to Elim Christian College: _________________________Proposed Year Level: __________________ Church Currently Attending: __________________________Length of Attendance:__________Affiliation:_______________ Address: __________________________________________________________________________Postal Code:______________ Home Phone: _____________________________Family Email: ______________________________________________________ Date of Birth: ________________ Date First Started Schooling: __________________Country of Citizenship: ______________ Iwi Affiliation (If student of NZ Maori descent, please enter name(s) of his/her Iwi):______________________________________________ Ethnicity: __________________________________(for MOE purposes)First Language:_________________________________ Early Childhood Education prior to School: _____________________________________________________________________ Current School: _______________________________________________________Present -
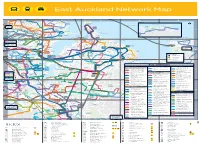
East Auckland Network Map
J002915_East Auckland Public Transport Guide.indd 4-5 East Auckland Network Map d Gl R ov er R d i Kohimarama Cl Karaka Musick Pt Beach Bay Reserve R Vale R u d r Ri k amaki D T A ut d Ronaki R Mission u Churchill Park r d t Poly d a C go ihill ve c nR R Bay de i k d N Ave School R S S A p d l ei l n l l ght a V l t St n Bay a S n atatu t ne S T o R M ri t a e d h A e l B C D E T d a M nd e St Heliers el R S n wy a e v ne C t k l d e e s a d t e t P v A S i ea e ia h t S v Howick t R a t H R l P r e a a l A im a a R S d o o R A e v a d l r Y e e l a n Golf Club A e k i C h A d e u n s a m D t dar v e S Kohimarama g i a n St n o i il m a n u te a r e M K Churchill Park i s d Maraetai o School g ns B Kohimarama r Paun e S s a l D t S e R a C K t e Rd t m d t Sy h e t S n u Madills R lo C es h d t d l t P d v d hi t A r e L i a l Farm Res a e e Rd e k a n r r l c o o fi R y e e v i P t Bucklands u R el o w s y ng d Orakei R K a S d A b d H m P A le u C A To ai St y K a v le o w e v r C View Bay M Beach u F a Omana Beach Ed D Dingle a um k d e l r te pe l s d B Cr Go R r e i Pohutukawa s d t Dell d h n de t A r A c u e n Cr o n v S d r e St Riddell R St nRd d o t t e d p gh g le c Bay Shelly o S Saye R d G k P C Ferries to Aucklando T Sunkist h R a r l l utuk Maraetai aw Glendowie H o Bay er W a Refer to a Glendowie T Mo G d a v e t St Thomas c a Kellys ampb e R e Glendowie t e Bay w C e n nd C n S r t ll R t a College a r l a d e r l R r R P Rd r School S ay Park d w r y d g a os Kep m o o d Beach i e e Selwyn B C ra T Central a -

Public Information Boards (PDF 3MB)
PAKURANGA - BOTANY Why are we here today? • To give an update on AMETI progress • Explain future programme • Discuss the Pakuranga-Botany phase of AMETI • Present ideas for the Bus Rapid Transit Network (RTN) …to seek your feedback What is AMETI? Overview of the various elements of the AMETI project N Panmure / Glen Innes New local road link Mt Wellington Quarry Link Road • The Auckland Manukau Transport Initiative Highway - Merton Road New link to Pilkington Road (AMETI) aims to improve transport links Panmure Station Panmure Town Centre New bus/rail interchange Roundabout replacement between the eastern suburbs of Manukau Rail Corridor streetscape improvements and Auckland City for all road users: car and Ellerslie Panmure Highway Panmure Lagoon Drive - Busway truck drivers, bus and rail users, cyclists and Tamaki River Highway pedestrians Mt Wellington SEART / Waipuna Road Panmure Bridge Pedestrian and cycle facility • AMETI will open potential for economic Grade separation development by improving access and HHowickowick easing congestion on key transport routes. Mt Wellington Highway Bus lanes and streetscape improvements Pakuranga Road Pakuranga Reeves Road Sylvia Town Flyover Park Waipuna Bridge Centre Who is delivering AMETI? SH1 Southern Motorway Duplication Ti Rakau Drive and Pakuranga Road Ti Rakau Drive - Busway and intersection improvements • Auckland Transport, an Auckland Council SEART / Carbine Road organisation, is responsible for delivering Grade separation AMETI Gossamer Drive • This picks up the previous work done by Gossamer Drive to Trugood Drive Trugood Drive Manukau and Auckland City Council and the Intersection improvements Auckland Regional Transport Agency (ARTA) Highbrook Botany Town Harris Road • The project is also funded by the New Industrial Area Centre Zealand Transport Agency (NZTA). -

Summary of Your Feedback on Proposed Traffic Flow Improvements for Ti Rakau Drive
Summary of your feedback on proposed traffic flow improvements for Ti Rakau Drive February 2018 – Ti Rakau Drive traffic flow improvements feedback report Contents Summary ............................................................................................................................. 2 Outcome ........................................................................................................................... 2 Next steps ........................................................................................................................ 2 Background ......................................................................................................................... 3 Project overview ............................................................................................................... 3 Aspects of project ............................................................................................................. 3 1. Peak hour bus lanes on Ti Rakau Drive ................................................................................... 4 2. Edgewater Drive (east) intersection.......................................................................................... 5 3. Gossamer Drive intersection .................................................................................................... 6 4. Botany Road intersection .......................................................................................................... 7 5. Te Irirangi Drive Countdown carpark entrance ........................................................................ -

The Warehouse New Zealand Ltd: Store and Distribution Centre Addresses Revised: 23 Nov 2016
The Warehouse New Zealand Ltd: Store and Distribution Centre Addresses Revised: 23 Nov 2016 Global Location Branch Number Number Branch Name Full Address Address 1 Address 2 Address 3 Address 4 Postcode (GLN) 103 The Warehouse NZ Ltd - WESTCITY 103 22-30 RAILSIDE AVE, WESTCITY MALL, HENDERSON,22-30 RAILSIDEAUCKLAND, AVE 0612 WESTCITY MALL HENDERSON AUCKLAND 0612 9429000092029 107 The Warehouse NZ Ltd - NEW LYNN 107 7-13 RATA STREET, NEW LYNN, AUCKLAND, 06007-13 RATA STREET NEW LYNN AUCKLAND 0600 9429000090988 110 The Warehouse NZ Ltd - TE AWAMUTU 110 5-7 GEORGE STREET, TE AWAMUTU, 3800 5-7 GEORGE STREET TE AWAMUTU 3800 9429000091008 111 The Warehouse NZ Ltd - PUKEKOHE 111 124 MANUKAU RD, PUKEKOHE, AUCKLAND, 2120124 MANUKAU RD PUKEKOHE AUCKLAND 2120 9429000091015 113 The Warehouse NZ Ltd - NEWMARKET 113 64-74 BROADWAY, NEWMARKET, AUCKLAND,64-74 1023 BROADWAY NEWMARKET AUCKLAND 1023 9429000091039 114 The Warehouse NZ Ltd - PAKURANGA FC 114 1 AYLESBURY STREET, PAKURANGA, AUCKLAND,1 AYLESBURY 2010 STREET PAKURANGA AUCKLAND 2010 9429000091046 115 The Warehouse NZ Ltd - WHANGAPARAOA 115 WADE RIVER RD, WHANGAPARAOA, AUCKLAND,WADE 0932 RIVER RD WHANGAPARAOA AUCKLAND 0932 9429000091053 116 The Warehouse NZ Ltd - WHANGAREI FC 116 PORT ROAD, WHANGAREI, 0110 PORT ROAD WHANGAREI 0110 9429000091060 117 The Warehouse NZ Ltd - KAITAIA 117 2 NORTH PARK DRIVE, KAITAIA, 0410 2 NORTH PARK DRIVE KAITAIA 0410 9429000091077 118 The Warehouse NZ Ltd - BIRKENHEAD 118 BIRKENHEAD SHOPPING CENTRE., MOKOIA RD,BIRKENHEAD BIRKENHEAD, SHOPPING AUCKLAND, CENTRE. 0626 -

Love Your Skin Balm Stockists
Love Your Skin Balm Stockists North Island, New Zealand Northland | Auckland – North | Auckland – Central | Auckland – East | Auckland – South Auckland – West | Hamilton / Waikato / Coromandel | Hawkes Bay / East Coast Bay of Plenty / Rotorua | Taranaki | Manawatu – Wanganui | Wellington / Kapiti Coast Northland Back to Top Flax Bush 50 Waterfront Road Mangonui 0442 Gifts on Rathbone 10 Rathbone Street Whangarei Whitcoulls Whangarei The Strand, Cameron St CBD Whangarei Matakana Pharmacy 2 Matakana Valley Rd, Matakana Life Pharmacy Franklin’s 48 Queen Street Warkworth Auckland – North Back to Top Whitcoulls Whangaparoa The Plaza, Cnr Main St & Whangaparaoa Rds, Arkles Bay Whangaparaoa Red Beach Pharmacy Cnr Bay St & Red Beach Rd Red Beach North Island, New Zealand Torbay Pharmacy 1040 Beach Rd Torbay Health 100 2/357 Albany Highway Albany Whitcoulls Albany (by New World) Shop S214, Westfield Albany Don McKinnon Drive Albany Whitcoulls Albany (by Foodcourt) Shop MM05, Westfield Don McKinnon Drive Albany Unsworth Heights Pharmacy 108 Unsworth Drive Albany Northcross Pharmacy 855 East Coast Road Browns Bay Whitcoulls Browns Bay Cnr Clyde & Anzac Rds Browns Bay North Harbour Pharmacy 1/326 Sunset Rd Mairangi Bay Whitcoulls Milford Shop 155, Milford Shopping Mall, 24 Milford Rd Milford Whitcoulls Takapuna Shop G31, Shore City Shopping Centre, 42 Anzac St Takapuna North Island, New Zealand Shorecare Pharmacy Smales Farm 74 Taharoto Road Takapuna Elements Glenfield Shop 359 Westfield Shopping Mall Cnr Glenfield Rd and Downing Street Glenfield -

Manukau City T2060 Concept Future Residential Demand & Distribution
Manukau City T2060 Concept Future Residential Demand & Distribution Manukau City Council May 2009 SCHEDULE Code Date Information / Comments Project Leader 004 May 2009 Report Adam Thompson DISCLAIMER Property Economics has taken every care to ensure the correctness of all the information contained in this report. All information has been obtained by what are considered to be reliable sources, and Property Economics has no reason to doubt its accuracy. It is however the responsibility of all parties acting on information contained in this report to make their own enquiries to verify correctness. This document has been prepared for the use of Manukau City Council only. Copyright © 2009 by Property Economics Ltd. 50616-5.0-004 MCC T2060 Residential Assessment.doc - 1 - TABLE OF CONTENTS 1. EXECUTIVE SUMMARY 3 2. INTRODUCTION 6 2.1 INFORMATION SOURCES 6 3. POPULATION & HOUSEHOLD GROWTH 7 4. RESIDENTIAL LAND SUPPLY 8 5. RESIDENTIAL CAPACITY ANALYSIS 9 6. HOUSING TYPE PREFERENCES 14 7. RESIDENTIAL MARKET AREA PROFILES 16 8. APARTMENT DEVELOPMENT VIABILITY 19 9. HOUSING TYPE & LOCATION PREERENCES 21 10. ECONOMIC IMPLICATIONS OF HOUSING SUPPLY 23 11. SOCIAL IMPLICATIONS OF HOUSING SUPPLY 23 12. ENVIRONMENTAL IMPLICATIONS OF HOUSING SUPPLY 24 13. HOUSING DISTRIBUTION & STAGING RECOMMENDATIONS 25 14. APPENDIX 1: FUTURE HIGH DEMAND AREAS 29 15. APPENDIX 2: HIGH DENSITY 800M AROUND CENTRES 30 16. APPENDIX 3: STATS NZ VS ARC GROWTH DISTRIBUTION 31 17. APPENDIX 4: MCC CAPACITY VS ARC GROWTH 32 LIST OF TABLES TABLE 1: RESIDENTIAL CAPACITY ESTIMATE PEL 10 TABLE 2: ESITMATED DEMAND BY HOUSE TYPE BY MARKET AREA 2060 (PEL) 11 TABLE 3: FORECAST RESIDENTIAL LOCATION PREFERENCE 12 TABLE 4: MARKET AREA VARIABLES 16 TABLE 5: APARTMENT DEVELOPMENT VIABILITY SCENARIOS 19 TABLE: 6: HOUSING PREFERENCES FOR MANUKAU CITY 2006 (CENSUS) 22 LIST OF FIGURES FIGURE 1: MANUKAU HOUSING MARKET AREAS 9 FIGURE 2: REGIONAL INCOME DISTRIBUTION 28 50616-5.0-004 MCC T2060 Residential Assessment.doc - 2 - Manukau City T2060 Concept Future Residential Demand & Distribution 1.