How Do Cyclic Antibiotics with Activity Against Gram-Negative Bacteria Permeate Membranes? a Machine Learning Informed Experimental Study Michelle W
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Neomycin and Polymyxin B Sulfates Solution for Irrigation, USP Rx Only
NEOMYCIN AND POLYMYXIN B SULFATES- neomycin and polymyxin b sulfates solution X-GEN Pharmaceuticals, Inc. ---------- Neomycin and Polymyxin B Sulfates Solution for Irrigation, USP Rx Only NOT FOR INJECTION DESCRIPTION Neomycin and Polymyxin B Sulfates Solution for Irrigation is a concentrated sterile antibiotic solution to be diluted for urinary bladder irrigation. Each mL contains neomycin sulfate equivalent to 40 mg neomycin base, 200,000 units polymyxin B sulfate, and Water for Injection, inactive ingredient: sulfuric acid. The 20-mL multiple dose vial contains, in addition to the above, 1 mg methylparaben (0.1%) added as a preservative. Neomycin sulfate, an antibiotic of the aminoglycoside group, is the sulfate salt of neomycin B and C produced by Streptomyces fradiae It has a potency equivalent to not less than 600 mcg of neomycin per mg. The structural formulae are: Polymyxin B sulfate, a polypeptide antibiotic, is the sulfate salt of polymyxin B1 and B2 produced by the growth of Bacillus polymyxa. It has a potency of not less than 6,000 polymyxin B units per mg. The structural formulae are: CLINICAL PHARMACOLOGY After prophylactic irrigation of the intact urinary bladder, neomycin and polymyxin B are absorbed in clinically insignificant quantities. A neomycin serum level of 0.1 mcg/mL was observed in three of 33 patients receiving the rinse solution. This level is well below that which has been associated with neomycin-induced toxicity. When used topically, polymyxin B sulfate and neomycin are rarely irritating. Microbiology: The prepared Neomycin and Polymyxin B Sulfates Solution for Irrigation is bactericidal. The aminoglycosides act by inhibiting normal protein synthesis in susceptible microorganisms. -

Review Article UDC: 615.281.015.8:616.9 Doi:10.5633/Amm.2019.0412
Review article UDC: 615.281.015.8:616.9 doi:10.5633/amm.2019.0412 THE IMPORTANCE OF OLD ANTIBIOTICS IN OVERCOMING RESISTANCE TO ANTIBIOTICS Zorica Jović1, Lidija Ristić2,3, Dane Krtinić1,4, Gorana Nedin-Ranković1, Ana Cvetanović4,5, Dušan Simić6 Antibiotics are medications used to prevent or cure infections caused by bacteria. Discovery and introduction of antibiotics into medical practice brought about revolutionary changes in therapy and eradication of infectious diseases. There is a rise of interest for usage of old antibiotics. These drugs could be invaluable in the treatment of certain infections and, in order for them to remain effective, it is necessary to conduct certain measures which would prove their worth. The aim of antibiotic therapy is to deliver the antibiotic to the place of infection and to retain it in the place of infection for a long period of time. Most of all, it is of utmost importance to educate about this all medical personnel in health care system, especially physicians. The fact that the availability of these drugs remains low in comparison to the efforts made in attempt of discovering new antibiotics, imposes the need for national regulatory agencies to get involved in regulating the usage of these drugs. Acta Medica Medianae 2019;58(4):80-84. Key words: antibiotics, resistance, infections 1University of Niš, Faculty of Medicine, Department of pletely different from contemporary industrially pro- Pharmacology and Toxicology, Niš, Serbia duced ones. Nevertheless, this does not diminish the 2 University of Niš, Faculty of Medicine, Department of Internal fact that certain herbal medicines which have anti- Medicine, Niš, Serbia 3Clinic of Pulmonary Diseases, Clinical center Niš, Niš, Serbia biotic properties were known to ancient Greeks and 4Clinic of Oncology, Clinical center Niš, Niš, Serbia Romans and that they constituted an important part 5University of Niš, Faculty of Medicine, Department of of their medical practices (1). -
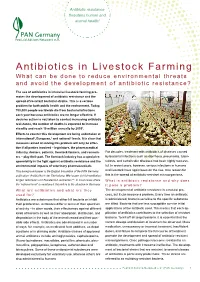
Antibiotics in Livestock Farming What Can Be Done to Reduce Environmental Threats and Avoid the Development of Antibiotic Resistance?
Antibiotic resistance threatens human and animal health! Antibiotics in Livestock Farming What can be done to reduce environmental threats and avoid the development of antibiotic resistance? The use of antibiotics in intensive livestock farming pro- motes the development of antibiotic resistance and the spread of resistant bacterial strains. This is a serious problem for both public health and the environment. Today, 700,000 people worldwide die from bacterial infections each year because antibiotics are no longer effective. If decisive action is not taken to combat increasing antibiotic resistance, the number of deaths is expected to increase steadily and reach 10 million annually by 20501. Efforts to counter this development are being undertaken at international2, European,3 and national4 levels. It is clear that measures aimed at solving this problem will only be effec- tive if all parties involved – legislators, the pharmaceutical industry, doctors, patients, livestock farmers, and consum- For decades, treatment with antibiotics of diseases caused ers – play their part. The livestock industry has a special re- by bacterial infections such as diarrhoea, pneumonia, tuber- sponsibility in the fight against antibiotic resistance and the culosis, and certain skin diseases has been highly success- environmental impacts of veterinary pharmaceuticals. ful. In recent years, however, serious infections in humans This background paper is the English translation of the PAN Germany and livestock have again been on the rise. One reason for publication “Antibiotika in der Tierhaltung. Wie lassen sich Umweltbelas- this is the spread of antibiotic-resistant microorganisms. tungen reduzieren und Resistenzen vermeiden”4a. In most cases where What is antibiotic resistance and why does the “national level” is mentioned, this refers to the situation in Germany. -

(12) Patent Application Publication (10) Pub. No.: US 2010/0028334 A1 Cottarel Et Al
US 20100028334A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2010/0028334 A1 Cottarel et al. (43) Pub. Date: Feb. 4, 2010 (54) COMPOSITIONS AND METHODS TO Publication Classification POTENTIATE COLISTIN ACTIVITY (51) Int. Cl. A638/12 (2006.01) (75) Inventors: Guillaume Cottarel, Mountain AOIN 37/00 (2006.01) View, CA (US); Jamey A 6LX 39/395 (2006.01) Wierzbowski, Stoneham, MA (US) A6IP3L/04 (2006.01) Correspondence Address: CI2O I/68 (2006.01) RONALDI. EISENSTEIN (52) U.S. Cl. ................... 424/130.1: 514/2: 514/9: 435/6 100 SUMMER STREET, NIXON PEABODY LLP BOSTON, MA 02110 (US) (57) ABSTRACT A pharmaceutical composition comprising an antimicrobial (73) Assignee: TRUSTEES OF BOSTON agent and an enhancer of an antimicrobial agent, wherein the UNIVERSITY, Boston, MA (US) enhancer of an antimicrobial agent is an inhibitor of gene, that by inactivating the gene product potentiates the effectiveness (21) Appl. No.: 12/519,336 of the antimicrobial agent. In some embodiments, the phar maceutical composition further comprises a pharmaceuti (22) PCT Filed: Dec. 13, 2007 cally acceptable carrier. In some embodiments, the antimi crobial agent is an antimicrobial peptide Such as a polymyxin, (86). PCT No.: PCT/US07/87397 for example but not limited to colistin. In some embodiments of the present invention provides methods to treat and/or S371 (c)(1), prevent infection of a Subject with a microorganism by (2), (4) Date: Jun. 15, 2009 administering a pharmaceutical composition comprising an antimicrobial agent and an enhancer of an antimicrobial Related U.S. Application Data agent. In some embodiments, the present invention provides (60) Provisional application No. -

The Bacitracin Biosynthesis Operon of Bacillus Licheniformis ATCC 10716
Research Paper 927 The bacitracin biosynthesis operon of Bacillus licheniformis ATCC 10716: molecular characterization of three multi-modular peptide synthetases Dirk Konzl, Andrea Klensl, Kurt Schbrgendorfer* and Mohamed A Marahiell Background: The branched cyclic dodecylpeptide antibiotic bacitracin, Addresses: ‘Philipps-Universittit Marburg, produced by special strains of Bacillus, is synthesized nonribosomally by a Fachbereich ChemielBiochemie, Hans-Meerwein- StraOe, 35032 Marburg, Germany. *Biochemie large multienzyme complex composed of the three bacitracin synthetases BAl , GmbH, 6330 Kufstein/Schaftenau, Austria. BA2 and BA3. These enzymes activate and incorporate the constituent amino acids of bacitracin by a thiotemplate mechanism in a pathway driven by a Correspondence: Mohamed A Marahiel protein template. The biochemical features of these enzymes have been studied E-mail: [email protected] intensively but little is known about the molecular organization of their genes. Key words: Bacillus licheniformus, bacitracin, DNA sequence, peptide antibiotics, peptide Results: The entire bacitracin synthetase operon containing the genes synthetases, thiazoline ring bacA-bacC was cloned and sequenced, identifying a modular structure typical of peptide synthetases. The bacA gene product (BAI , 598 kDa) contains five Received: 30 September 1997 Accepted: 28 October 1997 modules, with an internal epimerization domain attached to the fourth; bacB encodes BA2 (297 kDa), and has two modules and a carboxy-terminal Chemistry & Biology December 1997,4:927-937 epimerization domain; bacC encodes BA3, five modules (723 kDa) with http://biomednet.comlelecref/1074552100400927 additional internal epimerization domains attached to the second and fourth. A 0 Current Biology Ltd ISSN 1074-5521 carboxy-terminal putative thioesterase domain was also detected in BA3. -

Polypeptide Antibiotic
Polypeptide antibiotic •POLYMYXIN •BACITRACINE •TYROTHRICIN •VANCOMYCINE DR ARPITA SHRIVASTAV Polymyxin 2 Source- Bacillus polymyxa These are cyclic polypeptide classified ABCDE&M MECHANISM OF ACTION-:these are cationic surface active agent It interact with negatively charged phospholipids in bacterial cell membrane increase permeability of cell membrane and disrupt it leading to cell lysis It also inactivate endotoxins DR ARPITA SHRIVASTAV ASSISTANT 19/04/2020 PROFESSOR VETERINARY COLLEGE REWA Antibacterial spectrum 3 Its action against gram negative bacteria e.g.. E-coli, Salmonella , Pseudomonas except Proteus Gram positive bacteria is less sensitive Resistance Through reduce permeability Cross resistance between polymyxin B& D Pharmacokinetics They are neither absorbed topically nor orally and do not penetrate BBB Systemic effect by parental administration Excreted in urine DR ARPITA SHRIVASTAV ASSISTANT 19/04/2020 PROFESSOR VETERINARY COLLEGE REWA 4 Contraindication Renal disease patients Drug interaction Synergistic effect with sulphonamide,trimethopri(enterobector) polymyxine+amphoteresin B(antifungal) Toxicity Nephrotoxic Neurotoxin and neuromuscular blocked at high concentration Uses Orally used in life threatening infection caused by gram negative bacilli or pseudomonas Tropically in eye, ear and skin infection and bovine mastitis DR ARPITA SHRIVASTAV ASSISTANT 19/04/2020 PROFESSOR VETERINARY COLLEGE REWA Bacitracin 5 It is polypeptide antibiotic obtained from Bacillus subtilis It is narrow spectrum similar -

Intravenous Colistin in the Treatment of Sepsis from Multiresistant Gram
Critical Care October 2003 Vol 7 No 5 Markou et al. Research Open Access Intravenous colistin in the treatment of sepsis from multiresistant Gram-negative bacilli in critically ill patients Nikolaos Markou1, Haralampos Apostolakos2, Christiana Koumoudiou1, Maria Athanasiou1, Alexandra Koutsoukou3, Ioannis Alamanos1 and Leonidas Gregorakos1 1Intensive Care Unit B, Athens Trauma Hospital KAT, Athens, Greece 2Head of Department, Intensive Care Unit B, Athens Trauma Hospital KAT, Athens, Greece 3Microbiology Laboratory, Athens Trauma Hospital KAT, Athens, Greece Correspondence: Nikolaos Markou, [email protected] Received: 1 May 2003 Critical Care 2003, 7:R78-R83 (DOI 10.1186/cc2358) Revisions requested: 9 June 2003 This article is online at http://ccforum.com/content/7/5/R78 © 2003 Markou et al., licensee BioMed Central Ltd Revisions received: 7 July 2003 (Print ISSN 1364-8535; Online ISSN 1466-609X). This is an Open Accepted: 8 July 2003 Access article: verbatim copying and redistribution of this article are permitted in all media for any purpose, provided this notice is Published: 28 July 2003 preserved along with the article's original URL. Abstract Introduction The increasing prevalence of multiresistant Gram-negative strains in intensive care units (ICUs) has recently rekindled interest in colistin, a bactericidal antibiotic that was used in the 1960s for treatment of infections caused by Gram-negative bacilli. We conducted the present observational study to evaluate the efficacy of intravenous colistin in the treatment of critically ill patients with sepsis caused by Gram-negative bacilli resistant to all other antibiotics. Patients and method Critically ill patients with sepsis caused by Gram-negative bacilli resistant to all antibiotics with the exception of colistin were treated in the six-bed ICU of a trauma hospital. -

Polymyxin B, a Cationic Polypeptide Antibiotic, Interacts with Various
VOL. XXIX NO. 7 THE JOURNAL OF ANTIBIOTICS 735 EVIDENCES FOR COMPLEX FORMATION BETWEEN POLYMYXIN B AND LIPOPOLYSACCHARIDES FROM SERRATIA MARCESCENS* JOSEPH C. TSANG**, DOUGLAS A. WEBER and DAVID A. BROWN Departments of Chemistry and Biological Sciences, Illinois State University Normal, Illinois, U.S.A. (Received for publication January 27, 1976) In vitro and in vivo complex formations of polymyxin B and lipopolysaccharides (LPS) from resistant and sensitive cells of Serratia marcescens were studied by poly- acrylamide gel electrophoresis in sodium dodecyl sulfate and electron microscopy. In vitro treatment of LPS from resistant cells with polymyxin B gave two populations of spherical complexes of different molecular weights as determined electrophoretically. Similar treatment of LPS from sensitive cells resulted in dissociation of the LPS-protein and subsequent complexing with the LPS moiety into stable spheres. In vivo treatment of resistant cells with polymyxin B resulted in LPS-polymyxin B complexes which were comparatively smaller and existed in two morphological forms: spheres and linear ribbons. LPS from the sensitive cells were degraded extensively into small rods and an amorphous mass by the in vivo polymyxin B treatment. In both systems, the electrophoretic results consistently matched the electron microscopic evidences for complex formation of LPS with polymyxin B. It is suggested that the disruptive effects of polymyxin B on LPS in the outer membrane of S. marcescens may be the explanation for the change in permeability barrier in the resistant cells and disor- ganization of the outer membrane and subsequent death in the sensitive cells. Fur- thermore, the ability of the LPS to complex with the polymyxin B molecules in resistant cells may be the basis of their resistance to the antibiotic. -

University of Oklahoma
UNIVERSITY OF OKLAHOMA GRADUATE COLLEGE ANTIBIOTIC COMBINATION THERAPY AGAINST MULTIDRUG-RESISTANT STAPHYLOCOCCUS EPIDERMIDIS BIOFILMS AND BROADENING ANTIBIOTIC SPECTRUM USING POLYETHYLENIMINE A DISSERTATION SUBMITTED TO THE GRADUATE FACULTY in partial fulfillment of the requirements for the Degree of DOCTOR OF PHILOSOPHY By ANH KIM LAM Norman, Oklahoma 2020 ANTIBIOTIC COMBINATION THERAPY AGAINST MULTIDRUG-RESISTANT STAPHYLOCOCCUS EPIDERMIDIS BIOFILMS AND BROADENING ANTIBIOTIC SPECTRUM USING POLYETHYLENIMINE A DISSERTATION APPROVED FOR THE DEPARTMENT OF CHEMISTRY AND BIOCHEMISTRY BY THE COMMITTEE CONSISTING OF Dr. Charles V. Rice, Chair Dr. Si Wu Dr. Zhibo Yang Dr. Yihan Shao Dr. Mark Nanny © Copyright by ANH KIM LAM 2020 All Rights Reserved. Dedicated to my mom and all teachers, scientists, researchers, health care providers, policy makers, and others who are supporting science. Acknowledgements The completion of this graduate-school journey could not have been possible without the guidance and support of many people. Although my words are fallen short in expressing boundless gratitude for them whose names may not all be enumerated, I am immensely grateful! The most special thankfulness goes to my family, Quen Nguyen (Mẹ/Mother), Tai Lam (Ba/Father), Nhan Bunn (Cô-2/Aunt), and Travis Bunn (Daddle) for their strong and rooted support. My sincere thanks also arise for my cherished and valued friends who have become my adopted family: Melissa Hill, Anita Ly, Hannah Panlilio, and Dai & Ninh Nguyen! I feel deeply grateful to all the colleagues and members in the Rice Lab for each of them helped me in ways that I could never fully express: Erika Moen, Casey Wouters, Jennifer Pusavat, Beatrice Wilson, Andrew Neel, Tristan Haight, and Neda Heydarian. -

A Review of the Clinical Pharmacokinetics of Polymyxin B
Review A Review of the Clinical Pharmacokinetics of Polymyxin B Sean N. Avedissian 1,2,3, Jiajun Liu 1,2,3, Nathaniel J. Rhodes 1,2,3, Andrew Lee 4, Gwendolyn M. Pais 1,2, Alan R. Hauser 5, Marc H. Scheetz 1,2,3,6,* 1 Department of Pharmacy Practice, Chicago College of Pharmacy, Midwestern University, Downers Grove, IL 60515, USA; [email protected] (S.N.A.); [email protected] (J.L.); [email protected] (N.J.R.); [email protected] (G.M.P.) 2 Pharmacometrics Center of Excellence, Midwestern University Downers Grove, IL 60515, USA 3 Department of Pharmacy, Northwestern Memorial Hospital, Chicago, IL 60611, USA 4 Departments of Chemical and Biological Engineering, Northwestern University, Evanston, IL 60208, USA; [email protected] 5 Departments of Microbiology-Immunology and Medicine, Northwestern University, Feinberg School of Medicine, Chicago, IL 60611, USA; [email protected] 6 College of Graduate Studies, Department of Pharmacology, Midwestern University, Downers Grove, IL 60515, USA * Correspondence: [email protected]; Tel.: +1-630-515-6116; Fax: +1-630-515-6958 Abstract: Polymyxin B remains an antibiotic of last resort because of its toxicities. Although newer therapies are becoming available, it is anticipated that resistance to these agents will continue to emerge, and understanding the safest and most efficacious manner to deliver polymyxin B will remain highly important. Recent data have demonstrated that polymyxin B may be less nephrotoxic than colistin. Pharmacokinetically, polymyxin B is primarily eliminated via non-renal pathways, and most do not recommend adjusting the dose for renal impairment. However, some recent studies suggest a weak relationship between polymyxin B clearance and patient creatinine clearance. -
Colistimethate Sodium for Injection BP
For the use of only a registered medical practitioner or hospital or laboratory Colistimethate sodium for injection BP TM KOOLISTIN MÑ ÍsÉÍxOlÉ COMPOSITION • Intravenous administration for the treatment of some serious Each Vial contains infections caused by Gram-negative bacteria, including those Colistimethate Sodium BP 1 million IU of the lower respiratory tract and urinary tract, when more (IU: International Units) commonly used systemic antibacterial agents may be contra- indicated or may be ineffective because of bacterial resistance. DESCRIPTION • Treatment by inhalation of Pseudomonas aeruginosa lung Colistimethate sodium is a cyclic polypeptide antibiotic derived infection in patients with cystic fibrosis (CF). from Bacillus polymyxa var. colistinus and belongs to the polymyxin group. Usage Parenteral administration CLINICAL PHARMACOLOGY The normal adult dose of 2 million units should be dissolved in 10- Pharmacodynamics 50ml of 0.9% sodium chloride intravenous infusion or water for injections to form a clear solution. The solution is for single use Mechanism of action only and any remaining solution should be discarded. To avoid Colistimethate is a polymyxin group of antibiotic. The polymyxin frothing reconstitute the vial slowly without vigorous shaking and antibiotics are cationic agents that work by damaging the cell once reconstituted, should be used immediately. membrane. The resulting physiological affects are lethal to the bacterium. Polymyxins are selective for Gram-negative bacteria Inhalation that have a hydrophobic outer membrane. The required amount of powder is dissolved preferably in 2-4ml 0.9% sodium chloride solution and poured into the nebuliser. Microbiology Alternatively, water for injections may be used. The solution will Commonly susceptible species be slightly hazy and may froth if shaken. -

Antimicrobial Chemotherapy
Antimicrobial chemotherapy Prof. Beata M. Sobieszczańska Department of Microbiology University of Medicine Antimicrobials • Antibiotic is a low molecular substance produced by microorganisms (molds, bacteria) that at a low concentration inhibits or kills other microorganisms • Antimicrobial is any substance of natural, semisynthetic or synthetic origin that kills or inhibits the growth of microorganisms but causes little or no damage to the host All antibiotics are antimicrobials but not all antimicrobials are antibiotics Antimicrobials • Bacteriostatic = they inhibit bacterial growth but generally do not kill the bacteria e.g. protein synthesis inhibitors (macrolides, tetracyclines, aminoglycosides, streptogramins, lincosamides, oxazolidinones, chloramfenicol) • Bactericidal = agent that kills the target bacteria (β- lactams, glycopeptides, bacitracin, polymyxin, fluoroquinolones, metronidazole, rifampin) Drug’s spectrum of activity Depending on the range of bacterial species susceptible to antimicrobials – they are classified as: narrow spectrum - have limited activity to some bacteria e.g. GP or GN (e.g. penicillin, glycopeptides) broad spectrum – are active against both GP and GN (e.g. amoxycillin, carbapenems, fluoroquinolones) Sites of action of different antimicrobial agents Bactericidal - without cell wall, osmotic pressure causes bacteria to burst Examples • β-lactams • Glycopeptides • Bacitracin PBP=penicillin binding proteins (enzymes e.g. transpeptydases) : Penicillins in blocking transpeptidase enzymes from assembling the