African Medical and Research Foundation (AMREF)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -

Violent Conflict Implications of Mega Projects in Nyangatom Woreda, Ethiopia by Fana Gebresenbet, Mercy Fekadu Mulugeta and Yonas Tariku
Briefing Note #5 - May 2019 Violent Conflict Implications of Mega Projects in Nyangatom Woreda, Ethiopia By Fana Gebresenbet, Mercy Fekadu Mulugeta and Yonas Tariku Introduction This briefing note explores conflict in the past 10 years Key Findings in the Nyangatom Woreda of South Omo Zone, South- • Recorded, violent incidents have shown a ern Nations Nationalities and Peoples’ region, Ethiopia. decline in 2017/18; The Nyangatom are one of the 16 ethnic groups indig- enous to the Zone. They are found at the southwest- • Cattle raiding remains the most frequent violent ern corner of the Zone adjacent to two international act; boundaries with South Sudan and Kenya. • The decline of violent incidents is not indicative of positive peacebuilding efforts; The study is situated in a physical and political envi- ronment that has shown rapid change due to dam • Changing resource access is a reason for the and large-scale agricultural projects. The Lower Omo decline of violence with some groups and the witnessed rapid transformation over the past decade, increase of violence with others, discouraging following the construction of the Gilgel Gibe III dam, interaction with some and encouraging it with large sugar cane plantations, factories and other others; investments, along with some infrastructural and • According to zone and woreda officials the demographic change. safety net (particularly distribution of food) This briefing is part of a research project “Shifting In/ program is also instrumental in the decline of equality Dynamics in Ethiopia: from Research to Appli- violence; cation (SIDERA).” The project explores environmen- • The decline of violence has to be comple- tal, income and conflict dynamics after the state-led mented with acts of genuine efforts to build development interventions. -

Memo on Violence in South Omo Areas, SNNPRS, Ethiopia (October 2019): a Call for Preventive Action and Rule of Law
Memo on violence in South Omo areas, SNNPRS, Ethiopia (October 2019): a call for preventive action and rule of law Concerned Scholars Ethiopia (CSE) 25 October 2019 1. Since the 2018 change of government and the significant and promising reform process in Ethiopia, not all regions and peoples have fared equally well. While the policies of the new, Nobel Laureate PM Abiy Ahmed and his government hold out hope for millions and have bought very meaningful, positive changes, developments on the local level in ‘peripheral’ regions outside the purview of the Federal government are not yet addressed. Scores of people – including those of ethnic minority groups - are suffering of displacement, killings, and discrimination – all issues that are not in line with the new ethos of democratic reform and human rights respect. 2. The present Memo calls attention to the situation in the South Omo Region - as emblematic for more general problems that play out in some areas of the Southern Regional State (SNNPRS), in Beni Shangul-Gumuz, Gambela and possibly other Regional States of Ethiopia. 3. The prime cases at hand here are that of the ‘Bodi’ people (self-name: Me’en, with two sub-divisions: Mela and Chirim) in South Omo Zone (since 2nd week of September), and the Mursi people in South Omo Zone (since 29 September 2019, through to 13 October). Since 20 October there are also indications of additional instability in the Dima area (southwest of Mizan town) that has led to killings of people of the Suri ethnic group. So far, no decisive action has been taken by either the Federal Army or by local, Zonal or SNNPRS Regional authorities against abusive police and armed forces units. -

Food Supply Prospects - 2009
FOOD SUPPLY PROSPECTS - 2009 Disaster Management and Food Security Sector (DMFSS) Ministry of Agriculture and Rural Development (MoARD) Addis Ababa Ethiopia February 10, 2009 TABLE OF CONTENTS Pages LIST OF GLOSSARY OF LOCAL NAMES 2 ACRONYMS 3 EXECUTIVE SUMMARY 5 - 8 INTRODUCTION 9 - 12 REGIONAL SUMMARY 1. SOMALI 13 - 17 2. AMHARA 18 – 22 3. SNNPR 23 – 28 4. OROMIYA 29 – 32 5. TIGRAY 33 – 36 6. AFAR 37 – 40 7. BENSHANGUL GUMUZ 41 – 42 8. GAMBELLA 43 - 44 9. DIRE DAWA ADMINISTRATIVE COUNSEL 44 – 46 10. HARARI 47 - 48 ANNEX – 1 NEEDY POPULATION AND FOOD REQUIREMENT BY WOREDA 2 Glossary Azmera Rains from early March to early June (Tigray) Belg Short rainy season from February/March to June/July (National) Birkads cemented water reservoir Chat Mildly narcotic shrub grown as cash crop Dega Highlands (altitude>2500 meters) Deyr Short rains from October to November (Somali Region) Ellas Traditional deep wells Enset False Banana Plant Gena Belg season during February to May (Borena and Guji zones) Gu Main rains from March to June ( Somali Region) Haga Dry season from mid July to end of September (Southern zone of of Somali ) Hagaya Short rains from October to November (Borena/Bale) Jilal Long dry season from January to March ( Somali Region) Karan Rains from mid-July to September in the Northern zones of Somali region ( Jijiga and Shinile zones) Karma Main rains fro July to September (Afar) Kolla Lowlands (altitude <1500meters) Meher/Kiremt Main rainy season from June to September in crop dependent areas Sugum Short rains ( not more than 5 days -

Pastoral Conflict, Emerging Trends and Environmental Stress In
Ethiopian Journal of the Social Sciences and Humanities (EJOSSAH): V. 16, No. 2 ISSN (online): 2520-582X ISSN (print): 1810-4487 Pastoral Conflict, Emerging Trends and Environmental Stress in Nyangatom, Southern Ethiopia Temesgen Thomas Halabo* and Taddesse Berisso† Abstract This study examined the dynamics of conflict, emerging trends and relationship between inter-pastoral conflicts and environmental changes in Nyangatom, Southern Ethiopia. The study employed a qualitative approach and exploratory case study research design. The study revealed that inter-pastoral conflicts stem from multiple and compounding dynamics. The environmental change has escalated intense inter-pastoralists’ contestation and conflicts, including cross- border conflict, on the scarce and fast-depleting natural resources. Indeed, there is a causal link between inter-pastoral conflicts and environmental changes. In this regard, the environmental factor has uniquely affected the Nyangatom due to the drying of Kibish River and rapid invasion of Prosopis–Juliflora in their key grazing lands. In response to environmental stresses as part of the traditional copying mechanism, the Nyangatom cross border deep into South-Sudan to their ethnic kin of Toposa and into Kenya that usually causes frequent cross-border conflicts with Turkana pastoralists. Irrespective of discernible risk of conflicts, they used to migrate to Mursi and Surma territories that caused conflict. And yet, the Nyangatom has often engaged in frequent conflicts with Dasanach. The study suggests alternative livelihood options and an understanding of the complex conflict dynamics in view of the cause-effect relationships for future management of inter-pastoral and cross-border conflicts in the region. Keywords: Nyangatom, Pastoralism, Conflict, Emerging trends and Environmental stress DOI: https://dx.doi.org/10.1314/ejossah.v16i2.5 * Corresponding author: Assistant Professor, Department of Peace and Conflict Studies, Wachemo University, Email: [email protected], Tel 0904757011, P.O.Box 667/Hossana. -
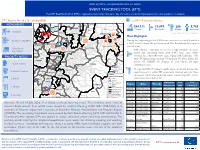
DTM Event Tracking Tool 30 (18-24 July 2020)
DISPLACEMENT TRACKING MATRIX-ETHIOPIA EVENT TRACKING TOOL (ETT) The DTM Event Tracking Tool (ETT) is deployed to track and provide up to date information on sudden displacements and other population movements ETT Report: No. 30 | 18 - 24 July 2020 CoVID-19 Situation Update ERITREA RED SEA YEMEN Wegde Kelela MOVEMENTS WembermaWest Gojam AFAR Gablalu TIGRAY Jama Zone 5 Oromia Hadhagala Ayisha KemashiSUDAN SOMALIA 364,322 12,693 200 5,785 East Gojam Gewane AFAR DJIBOUTI AMHARA GULF OF ADEN AmuruAMHARA Zone 3 Siti Tested Confirmed Deaths Recovered BENISHANGUL GUMUZ Shinile 7,876 IDPs North Shewa Dembel ADDIS ABABA Source: Ministry of Health, 24 July 2020 HARARI North Shewa 180 Kuyu DIRE DAWA GAMBELA Horo Gudru Wellega Amibara 66 Chinaksen OROMIA Jarso Main Highlights SOMALI Dulecha Miesso SNNPR Kombolcha KemashiSOUTH Gursum SUDAN Cobi Sululta Haro Maya Conict (4,202 IDPs) 3,102 Mieso 136 During the reporting period, 3,546 new cases were recorded, which is SOMALIA KENYA West Shewa UGANDA ADDIS ABABA 139 Girawa Fedis Fafan a 146% increase from the previous week. The breakdown by region is East Wellega Babile 162 Ilu Fentale East Hararge listed below. Dawo West Hararge Flash Floods 410 Boset 20 Boke Kuni Nono Merti Addis Ababa continued to record a high number of cases (3,674 IDPs) South West Shewa East Shewa Jeju Buno Bedele Sire within the reporting week with 2,447 new cases while Hawi Gudina Jarar Guraghe Fik Kumbi Degehamedo Oromia recorded 289 new cases, Tigray 236, Gambela 170, PRIORITY NEEDS Silti Sude Jimma Arsi Amigna Lege Hida Erer Yahob Afar 74, Benishangul Gumuz 73, Amhara 68, Dire Dawa 52, Yem Siltie OROMIA Gibe Seru Hamero Somali 47, SNNPR 39, Sidama 31, and Harari 20 new Hadiya Shirka Sagag 1. -

Army Worm Infestation in SNNP and Oromia Regions As of 24 May
Army worm infestation in SNNP and Oromia Regions As of 24 May, some 8,368 hectares of belg cropland was reportedly destroyed by army worms in Wolayita zone of SNNPR - an area that suffered from late onset of the 2013 belg rains and subsequent heavy rains that damaged belg crops. The damage caused by the army worms will further reduce the expected harvest this season. Similar incidents were also reported from Boricha, Bona Zuria, Dara, Dale, Hawassa Zuria and Loko Abaya woredas of Sidama zone; Loma and Mareka woredas of Dawro zone (SNNPR), as well as from drought prone areas of East and West Hararge zones of Oromia Region; and quickly spreading to neighbouring areas. In Boricha woreda, for example, more than 655 hectares of belg cropland was destroyed in the course of one week, this is indicative of the speed that damage is being caused. Immediate distribution of spraying containers and chemicals to the farmers is required to prevent further loss of belg crops. For more information, contact: [email protected] Health Update The number of meningitis cases has gradually declined since the outbreak was declared in January. To date, 1,371 cases were reported from 24 woredas in five zones of SNNP and Oromia Regions. The Government, with support from health partners, is conducting a reactive vaccination in the affected areas, with 1, 678,220 people vaccinated so far. Next week, the number of people vaccinated during the Addis Ababa City Administration meningitis vaccination campaign, conducted from 20 to 26 May, will be released. Meanwhile, the number of kebeles reporting cases of Yellow Fever in South Ari, Benatsemay and Selmago woredas of South Omo zone, SNNPR, increased. -

Baseline Survey Report for the Regional Pastoral Livelihoods Resilience Project in Ethiopia
Baseline survey report for the Regional Pastoral Livelihoods Resilience Project in Ethiopia ILRI PROJECT REPORT ISBN: 92–9146–527–5 The International Livestock Research Institute (ILRI) works to improve food and nutritional security and reduce poverty in developing countries through research for efficient, safe and sustainable use of livestock. Co-hosted by Kenya and Ethiopia, it has regional or country offices and projects in East, South and Southeast Asia as well as Central, East, Southern and West Africa. ilri.org CGIAR is a global agricultural research partnership for a food-secure future. Its research is carried out by 15 research centres in collaboration with hundreds of partner organizations. cgiar.org Baseline survey report for the Regional Pastoral Livelihoods Resilience Project in Ethiopia Berhanu Gebremedhin, Mengistu Woldehanna, Fiona Flintan, Barbara Wieland and Jane Poole December 2017 © 2017 International Livestock Research Institute (ILRI) ILRI thanks all donors and organizations which globally support its work through their contributions to the CGIAR system This publication is copyrighted by the International Livestock Research Institute (ILRI). It is licensed for use under the Creative Commons Attribution 4.0 International Licence. To view this licence, visit https://creativecommons.org/licenses/by/4.0. Unless otherwise noted, you are free to share (copy and redistribute the material in any medium or format), adapt (remix, transform, and build upon the material) for any purpose, even commercially, under the following conditions: ATTRIBUTION. The work must be attributed, but not in any way that suggests endorsement by ILRI or the author(s). NOTICE: For any reuse or distribution, the licence terms of this work must be made clear to others. -

World Bank Document
Sample Procurement Plan (Text in italic font is meant for instruction to staff and should be deleted in the final version of the PP) Public Disclosure Authorized (This is only a sample with the minimum content that is required to be included in the PAD. The detailed procurement plan is still mandatory for disclosure on the Bank’s website in accordance with the guidelines. The initial procurement plan will cover the first 18 months of the project and then updated annually or earlier as necessary). I. General 1. Bank’s approval Date of the procurement Plan: Updated Procurement Plan, M 2. Date of General Procurement Notice: Dec 24, 2006 Public Disclosure Authorized 3. Period covered by this procurement plan: The procurement period of project covered from year June 2010 to December 2012 II. Goods and Works and non-consulting services. 1. Prior Review Threshold: Procurement Decisions subject to Prior Review by the Bank as stated in Appendix 1 to the Guidelines for Procurement: [Thresholds for applicable procurement methods (not limited to the list below) will be determined by the Procurement Specialist /Procurement Accredited Staff based on the assessment of the implementing agency’s capacity.] Public Disclosure Authorized Procurement Method Prior Review Comments Threshold US$ 1. ICB and LIB (Goods) Above US$ 500,000 All 2. NCB (Goods) Above US$ 100,000 First contract 3. ICB (Works) Above US$ 15 million All 4. NCB (Works) Above US$ 5 million All 5. (Non-Consultant Services) Below US$ 100,000 First contract [Add other methods if necessary] 2. Prequalification. Bidders for _Not applicable_ shall be prequalified in accordance with the provisions of paragraphs 2.9 and 2.10 of the Public Disclosure Authorized Guidelines. -

Ethiopia: Administrative Map (August 2017)
Ethiopia: Administrative map (August 2017) ERITREA National capital P Erob Tahtay Adiyabo Regional capital Gulomekeda Laelay Adiyabo Mereb Leke Ahferom Red Sea Humera Adigrat ! ! Dalul ! Adwa Ganta Afeshum Aksum Saesie Tsaedaemba Shire Indasilase ! Zonal Capital ! North West TigrayTahtay KoraroTahtay Maychew Eastern Tigray Kafta Humera Laelay Maychew Werei Leke TIGRAY Asgede Tsimbila Central Tigray Hawzen Medebay Zana Koneba Naeder Adet Berahile Region boundary Atsbi Wenberta Western Tigray Kelete Awelallo Welkait Kola Temben Tselemti Degua Temben Mekele Zone boundary Tanqua Abergele P Zone 2 (Kilbet Rasu) Tsegede Tselemt Mekele Town Special Enderta Afdera Addi Arekay South East Ab Ala Tsegede Mirab Armacho Beyeda Woreda boundary Debark Erebti SUDAN Hintalo Wejirat Saharti Samre Tach Armacho Abergele Sanja ! Dabat Janamora Megale Bidu Alaje Sahla Addis Ababa Ziquala Maychew ! Wegera Metema Lay Armacho Wag Himra Endamehoni Raya Azebo North Gondar Gonder ! Sekota Teru Afar Chilga Southern Tigray Gonder City Adm. Yalo East Belesa Ofla West Belesa Kurri Dehana Dembia Gonder Zuria Alamata Gaz Gibla Zone 4 (Fantana Rasu ) Elidar Amhara Gelegu Quara ! Takusa Ebenat Gulina Bugna Awra Libo Kemkem Kobo Gidan Lasta Benishangul Gumuz North Wello AFAR Alfa Zone 1(Awsi Rasu) Debre Tabor Ewa ! Fogera Farta Lay Gayint Semera Meket Guba Lafto DPubti DJIBOUTI Jawi South Gondar Dire Dawa Semen Achefer East Esite Chifra Bahir Dar Wadla Delanta Habru Asayita P Tach Gayint ! Bahir Dar City Adm. Aysaita Guba AMHARA Dera Ambasel Debub Achefer Bahirdar Zuria Dawunt Worebabu Gambela Dangura West Esite Gulf of Aden Mecha Adaa'r Mile Pawe Special Simada Thehulederie Kutaber Dangila Yilmana Densa Afambo Mekdela Tenta Awi Dessie Bati Hulet Ej Enese ! Hareri Sayint Dessie City Adm. -

Social-Ecological Change in the Omo-Turkana Basin: a Synthesis of Current Developments
Ambio https://doi.org/10.1007/s13280-018-1139-3 REVIEW Social-ecological change in the Omo-Turkana basin: A synthesis of current developments Jennifer Hodbod , Edward G. J. Stevenson, Gregory Akall, Thomas Akuja, Ikal Angelei, Elias Alemu Bedasso, Lucie Buffavand, Samuel Derbyshire, Immo Eulenberger, Natasha Gownaris, Benedikt Kamski, Abdikadir Kurewa, Michael Lokuruka, Mercy Fekadu Mulugeta, Doris Okenwa, Cory Rodgers, Emma Tebbs Received: 28 February 2018 / Revised: 27 September 2018 / Accepted: 12 December 2018 Abstract This paper synthesizes current knowledge on the INTRODUCTION impacts of the Gibe III dam and associated large-scale commercial farming in the Omo-Turkana Basin, based on Semi-arid regions across Africa are undergoing a period of an expert elicitation coupled with a scoping review and the rapid environmental and social change, but the Omo-Tur- collective knowledge of an multidisciplinary network of kana region in southern Ethiopia and northern Kenya is researchers with active data-collection programs in the arguably unique in the scale and pace at which change is Basin. We use social-ecological systems and political occurring. This paper focuses on the changes taking place ecology frameworks to assess the impacts of these due to a series of current and planned future hydropower interventions on hydrology and ecosystem services in the dams in the Lower Omo, the most recently completed Basin, and cascading effects on livelihoods, patterns of being the Gilgel-Gibe III (hereafter ‘Gibe III’) dam, Afri- migration, and conflict dynamics for the people of the ca’s tallest, and the establishment of irrigated sugar estates region. A landscape-scale transformation is occurring in covering a projected 100 000 hectares (ha) as well as large- which commodities, rather than staple foods for local scale cotton schemes (Sugar Corporation 2013). -

Ethiopia Administrative Map As of 2013
(as of 27 March 2013) ETHIOPIA:Administrative Map R E Legend E R I T R E A North D Western \( Erob \ Tahtay Laelay National Capital Mereb Ahferom Gulomekeda Adiyabo Adiyabo Leke Central Ganta S Dalul P Afeshum Saesie Tahtay Laelay Adwa E P Tahtay Tsaedaemba Regional Capital Kafta Maychew Maychew Koraro Humera Asgede Werei Eastern A Leke Hawzen Tsimbila Medebay Koneba Zana Kelete Berahle Western Atsbi International Boundary Welkait Awelallo Naeder Tigray Wenberta Tselemti Adet Kola Degua Tsegede Temben Mekele Temben P Zone 2 Undetermined Boundary Addi Tselemt Tanqua Afdera Abergele Enderta Arekay Ab Ala Tsegede Beyeda Mirab Armacho Debark Hintalo Abergele Saharti Erebti Regional Boundary Wejirat Tach Samre Megale Bidu Armacho Dabat Janamora Alaje Lay Sahla Zonal Boundary Armacho Wegera Southern Ziquala Metema Sekota Endamehoni Raya S U D A N North Wag Azebo Chilga Yalo Amhara East Ofla Teru Woreda Boundary Gonder West Belesa Himra Kurri Gonder Dehana Dembia Belesa Zuria Gaz Alamata Zone 4 Quara Gibla Elidar Takusa I Libo Ebenat Gulina Lake Kemkem Bugna Kobo Awra Afar T Lake Tana Lasta Gidan (Ayna) Zone 1 0 50 100 200 km Alfa Ewa U Fogera North Farta Lay Semera ¹ Meket Guba Lafto Semen Gayint Wollo P O Dubti Jawi Achefer Bahir Dar East Tach Wadla Habru Chifra B G U L F O F A D E N Delanta Aysaita Creation date:27 Mar.2013 P Dera Esite Gayint I Debub Bahirdar Ambasel Dawunt Worebabu Map Doc Name:21_ADM_000_ETH_032713_A0 Achefer Zuria West Thehulederie J Dangura Simada Tenta Sources:CSA (2007 population census purpose) and Field Pawe Mecha