Is There an Urban-Rural Divide? Population Surveys of Rheumatic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

District Taluka Center Name Contact Person Address Phone No Mobile No
District Taluka Center Name Contact Person Address Phone No Mobile No Mhosba Gate , Karjat Tal Karjat Dist AHMEDNAGAR KARJAT Vijay Computer Education Satish Sapkal 9421557122 9421557122 Ahmednagar 7285, URBAN BANK ROAD, AHMEDNAGAR NAGAR Anukul Computers Sunita Londhe 0241-2341070 9970415929 AHMEDNAGAR 414 001. Satyam Computer Behind Idea Offcie Miri AHMEDNAGAR SHEVGAON Satyam Computers Sandeep Jadhav 9881081075 9270967055 Road (College Road) Shevgaon Behind Khedkar Hospital, Pathardi AHMEDNAGAR PATHARDI Dot com computers Kishor Karad 02428-221101 9850351356 Pincode 414102 Gayatri computer OPP.SBI ,PARNER-SUPA ROAD,AT/POST- 02488-221177 AHMEDNAGAR PARNER Indrajit Deshmukh 9404042045 institute PARNER,TAL-PARNER, DIST-AHMEDNAGR /221277/9922007702 Shop no.8, Orange corner, college road AHMEDNAGAR SANGAMNER Dhananjay computer Swapnil Waghchaure Sangamner, Dist- 02425-220704 9850528920 Ahmednagar. Pin- 422605 Near S.T. Stand,4,First Floor Nagarpalika Shopping Center,New Nagar Road, 02425-226981/82 AHMEDNAGAR SANGAMNER Shubham Computers Yogesh Bhagwat 9822069547 Sangamner, Tal. Sangamner, Dist /7588025925 Ahmednagar Opposite OLD Nagarpalika AHMEDNAGAR KOPARGAON Cybernet Systems Shrikant Joshi 02423-222366 / 223566 9763715766 Building,Kopargaon – 423601 Near Bus Stand, Behind Hotel Prashant, AHMEDNAGAR AKOLE Media Infotech Sudhir Fargade 02424-222200 7387112323 Akole, Tal Akole Dist Ahmadnagar K V Road ,Near Anupam photo studio W 02422-226933 / AHMEDNAGAR SHRIRAMPUR Manik Computers Sachin SONI 9763715750 NO 6 ,Shrirampur 9850031828 HI-TECH Computer -

Analysis of Accumulated Heavy Metal Concentrations in Various Body Parts of Chillapi (Oreochromis Mossambicus) Fish from Ujjani Reservoir of Maharashtra, India
Advances in Zoology and Botany 8(2): 37-44, 2020 http://www.hrpub.org DOI: 10.13189/azb.2020.080201 Analysis of Accumulated Heavy Metal Concentrations in Various Body Parts of Chillapi (Oreochromis mossambicus) Fish from Ujjani Reservoir of Maharashtra, India 1 2 1 3 4,* Dnyaneshwar Shinde , Pramod Kamble , D.M. Mahajan ,Vikas Devkar , Sanjay Chakane 1Postgraduate Research Center in Environmental Science, Baburaoji Gholap College, India 2Department of Environmental Science, Savitribai Phule Pune University, India 3Department of Food Science and Post Harvesting Technology, Arts, Science and Commerce College, India 4Department of Physics, Arts, Science and Commerce College, India Received September 27, 2019; Revised December 3, 2019; Accepted February 7, 2020 Copyright©2020 by authors, all rights reserved. Authors agree that this article remains permanently open access under the terms of the Creative Commons Attribution License 4.0 International License Abstract The heavy metal contamination is creating Keywords Ujjani Reservoir, Heavy Metals, Chillapi, devastating effects on ecosystem and environment and Oreochromis mossambicus, AAS, World Health eventually hazardous to human health. Ujjani is one of the Organization, Biomagnifications largest reservoir in Maharashtra state. It receives water from different metropolitan cities harboring numerous industries. Moreover, anthropogenic activities pollute water and fish fauna of the reservoir. In the present study, 1. Introduction the concentrations of heavy metals such as Iron (Fe), Copper (Cu), Zinc (Zn), and Manganese (Mn) were The pollution of fresh water resources is the major analyzed from various tissues namely muscles, liver, gill, concern globally. The discharge of pollutant through and fin of Chillapi fish. The variation in level of metals was anthropogenic activity has been increased tremendously found with respect to tissue types and body weight groups. -

IEE: India: Pune-Guntakal Electrification and Daund
Initial Environmental Examination March 2011 India: Railway Sector Investment Program Pune-Guntakal Electrification and Daund–Gaulbarga Doubling Subprojects Prepared by Ministry of Railway for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 15 March 2011) Currency unit – Indian rupee (Rs) Rs1.00 = $0.22222 Rs 45.00 $1.00 = ABBREVIATIONS ACF Assistant Conservator of Forest ADB Asian Development Bank EIA environmental impact assessment EMoP environment monitoring plan EMP environment management plan ESDU Environment and Social Development Unit GIS geographic information system GOI Government of India GHG greenhouse gases HFL highest flood level IBS Intermittent Block Station ICAR Indian Council of Agricultural Research IEE initial environmental examination IS Indian Standard IUCN International Union for Conservation of Nature Jn. junction (The term used by Indian Railways for the Stations where two or more lines meet) LHS Left Hand Side MoEF Ministry of Environment and Forests MOR Ministry of Railways NAAQS National Ambient Air Quality Standard NE northeast NGO non-governmental organization NH national highway NSDP National Strategic Development Program NOx oxides of nitrogen PF protected forest PHC public health centre PIU project implementation unit PPEs personal protective equipments PMC Project Management Consultant PWD Public Works Department RDSO Research Design and Standards Organization R&R resettlement and rehabilitation RF reserved forest RHS right hand side RoB road over bridge RoW right of way RSPM respirable suspended -

Fertility Status of Soil in the Green Belt of Indapur Tahsil, Dist - Pune (Maharashtra) India by Bhore J
Global Journal of Science Frontier Research Enviornment & Earth Sciences Volume 12 Issue 1 Version 1.0 Year 2012 Type : Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-4626 & Print ISSN: 0975-5896 Fertility Status of Soil in the Green Belt of Indapur Tahsil, Dist - Pune (Maharashtra) India By Bhore J. B. , Dangat V. T. , Jaybhaye R.G. & Gatkul B. I. Pune University Abstract - The increasing land use intensity without adequate and balanced use of chemical fertilizers. Little or no use of organic manure have caused severe fertility deterioration of soil. Resulting in declining of crop productivity. Study was carried out in the belts namely sample sites 1 to20 which is a green belt of indapur Tahsil in pune district. ( Maharashtra) To investigate the fertility status of soil during 2010 and 2011. Present study show that the soil were acidic and alkaline in nature in all season. Available nitrogen & phosphorous and potash show low soils were not sufficiently fertile for crop production. GJSFR-H Classification : FOR Code: 050303 Fertility Status of Soil in the Green Belt of Indapur Tahsil Dist - Pune MaharashtraIndia Strictly as per the compliance and regulations of : © 2012. Bhore J. B. , Dangat V. T. , Jaybhaye R.G. & Gatkul B. I.This is a research/review paper, distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License http://creativecommons.org/licenses/by-nc/3.0/), permitting all non commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. Fertility Status of Soil in the Green Belt of Indapur Tahsil , Dist - Pune (Maharashtra) India Bhore J. -
Bpc(Maharashtra) (Times of India).Xlsx
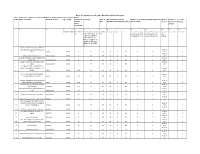
Notice for appointment of Regular / Rural Retail Outlet Dealerships BPCL proposes to appoint Retail Outlet dealers in Maharashtra as per following details : Sl. No Name of location Revenue District Type of RO Estimated Category Type of Minimum Dimension (in Finance to be arranged by the applicant Mode of Fixed Fee / Security monthly Site* M.)/Area of the site (in Sq. M.). * (Rs in Lakhs) Selection Minimum Bid Deposit Sales amount Potential # 1 2 3 4 5 6 7 8 9a 9b 10 11 12 Regular / Rural MS+HSD in SC/ SC CC1/ SC CC- CC/DC/C Frontage Depth Area Estimated working Estimated fund required Draw of Rs in Lakhs Rs in Lakhs Kls 2/ SC PH/ ST/ ST CC- FS capital requirement for development of Lots / 1/ ST CC-2/ ST PH/ for operation of RO infrastructure at RO Bidding OBC/ OBC CC-1/ OBC CC-2/ OBC PH/ OPEN/ OPEN CC-1/ OPEN CC-2/ OPEN PH From Aastha Hospital to Jalna APMC on New Mondha road, within Municipal Draw of 1 Limits JALNA RURAL 33 ST CFS 30 25 750 0 0 Lots 0 2 Draw of 2 VIllage jamgaon taluka parner AHMEDNAGAR RURAL 25 ST CFS 30 25 750 0 0 Lots 0 2 VILLAGE KOMBHALI,TALUKA KARJAT(NOT Draw of 3 ON NH/SH) AHMEDNAGAR RURAL 25 SC CFS 30 25 750 0 0 Lots 0 2 Village Ambhai, Tal - Sillod Other than Draw of 4 NH/SH AURANGABAD RURAL 25 ST CFS 30 25 750 0 0 Lots 0 2 ON MAHALUNGE - NANDE ROAD, MAHALUNGE GRAM PANCHYAT, TAL: Draw of 5 MULSHI PUNE RURAL 300 SC CFS 30 25 750 0 0 Lots 0 2 ON 1.1 NEW DP ROAD (30 M WIDE), Draw of 6 VILLAGE: DEHU, TAL: HAVELI PUNE RURAL 140 SC CFS 30 25 750 0 0 Lots 0 2 VILLAGE- RAJEGAON, TALUKA: DAUND Draw of 7 ON BHIGWAN-MALTHAN -

International Journal of Biological Innovations
IJBI 2 (2), (DECEMBER 2020) 287-294 International Journal of Biological Innovations Available online: http://ijbi.org.in | http://www.gesa.org.in/journals.php DOI: https://doi.org/10.46505/IJBI.2020.2225 Research article E-ISSN: 2582-1032 STUDY OF WADERS DIVERSITY IN THE CATCHMENT AREA OF UJANI RESERVOIR, SOLAPUR DISTRICT (MS), INDIA D. S. Kumbhar1* and D. K. Mhaske2 1Department of Zoology, D. P. Mahavidyalaya, Karjat Dist. Ahmednagar (MS), India 2Department of Zoology, MJS Mahavidyalaya, Shrigonda Dist. Ahmednagar (MS), India *Corresponding author: [email protected] Received: 20.09.2020 Accepted: 15.10.2020 Published: 25.10.2020 Abstract: The present study was an attempt to access and evaluate the status and distribution of waders associated to wetlands of Ujani Reservoir with special reference to north - west region. Waders are the birds generally observed along shorelines and mudflats that wade in order to forage for food in mud or sand. Ujani wetlands provide feeding and roosting grounds for resident and migratory waders. This study was conducted from December 2015 to November 2017 including seasonal visits to five wetland sites i.e. Kumbhargaon, Diksal, Kondhar-Chincholii, Rajegaon (Bhigwan) and Khanota. During study, about 38 species of waders were identified belonging to 14 families viz. Ardeidae, Charadriidae, Ciconiidae, Jacanidae, Laridae, Rallidae, Motacillidae, Phalacrocoracidae, Phoenicopteridae, Recurvirostridae, Rostratulidae, Scolopacidae, Threskiornithidae and Glariolidae. Keywords: Biodiversity, Ramsar Convention, Ujani Reservoir, Waders, Wetlands. INTRODUCTION ecosystem both are dependent on hydrologic Birds (Aves) also referred to as masters of air, regime and geological conditions. The are homeothermic or warm-blooded egg-laying maintenance of healthy aquatic ecosystem is vertebrates characterized by the presence of required for ecological balance, agriculture, feathers and modification of forelimbs as widespread biodiversity and human survival wings for flight. -

Solapur Division
SOLAPUR DIVISION SALIENT FEATURES OF SUR DIVISION Solapur is one of the Division of Central Railway situated on Mumbai – Chennai route having 983.70 route kilometers. Jurisdiction: Yeola - Daund, Daund -Wadi, Kurduwadi –LaturRoad &Kurduwadi- Miraj.This division plays the pivotal role of being corridor connection to West and South. Civil DistrictsHeadquarters:The Division covers 7 civil districts of Maharashtra State viz. Nasik, Ahmednagar, Pune, Solapur, Sangli, Latur, Osmanabad& One district of Karnataka i.e. Kalaburagi. The Division has 86stations in its jurisdiction under various categories. An annual average of 3.37crores originating passengers was dealt on Solapur Division in financial year 2017-18. An annual originating earning ofRs. 885.94croresgeneratedby Solapur Division in financial year 2017-18. Route length (Kms) :S/L – 799.81, Kms , D/L – 183.89Kms= Total- 983.70 Kms States in Solapur Division territory: Maharashtra: 89.76, Karnataka:10.24 %%, TICKETING SYSTEM: UTS: - Unreserved Ticketing System is provided at all 76 stations which are manned by either Commercial or operating staff on the division. At halt stations which are operated by halt station contractors the conventional printed card tickets are issued. UTS cum PRS: - Unreserved Ticketing systems Cum Passenger Reservation System are operated at 22 locations. PRS: - Computerized Passenger Reservation System at 20 PRS locations out of which 11 are Railway operated PRS centers. Balance 9 are Non Rail Head locations. JTBS: - Jansadharan Ticket Booking Sevaks are available at 4 locations. YTSK: 4 Yatri Ticket Suvidha Kendra are appointed at Solapur. ATVM :- Automatic Ticket Vending Machines–20, Co-TVM: -Coin & currency operated TicketVending Machine - 12. STBA: -Station Ticket Booking Agents have been nominated at 9, E category stations. -

Distribution of Periodical Market Centres in Pune District of Maharashtra
INTERNATIONAL RESEARCH JOURNAL OF MULTIDISCIPLINARY STUDIES Vol. 3, Issue 6, June, 2017 ISSN (Online): 2454-8499 Impact Factor: 1.3599(GIF), 0.679(IIFS) Distribution of Periodical Market Centres in Pune District of Maharashtra Muluk Dilip Dnyaneshwar Assistant professor, Department of Geography HutatmaRajguruMahavidayalaya, Rajgurunagar, Tal –Khed, Dist – Pune. Abstract: An attempt has been made in this paper to study the distribution and periodicity of the (weekly) market centers in the Pune District. Market centers are the basic and root level center of the economic and commercial activities. In various fields of Geography, Economic geography has experienced remarkable changes within the past thirty years resulting in diverse specialized branches such as geography of agriculture, industry, transportation marketing etc. All these branches are related to the study of great variations on the earth’s surface in means economic activities. Marketing is a part of human beings economic activity it deals with the marketing activity. Economic geography has considerable attention on the study of resources and factors of production associated with market places and marketing. Marketing Geography is a branch of economic Geography which seeks a specialized study of marketing places and marketing. Marketing Geography deals with the application of the Geographical principles, methods and techniques to the practical problems related to the marketing phenomena. In the present paper an analysis has been made to study the problems of weekly (periodic) market centers of Pune District and weekly market centers play process, mediating exchanger between farmers and craft manufactures for sellers and traders on the other hand urban wholesalers. The observation reveals that, there is uneven distribution and Weekly market centers in the study region Key Words :Weekly Market, economic activity, retail-wholesale trade, Marketing Geography Market centers, Distribution, Periodicity. -

Entirely Electronic Journal Published Annually by the Institute for Bird Populations
BIRD POPULATIONS A journal of global avian demography and biogeography Volume 13 2014 Published annually by The Institute for Bird Populations BIRD POPULATIONS A journal of global avian demography and biogeography Published by The Institute for Bird Populations Editor: DAVID G. AINLEY, H.T. Harvey & Associates, 983 University Avenue, Bldg D, Los Gatos, CA 95032; 415-272-9499; [email protected] Managing Editor: DAVID F. DESANTE, The Institute for Bird Populations, P.O. Box 1346, Point Reyes Station, CA 94956-1346; 415-663-2052; 415-663-9482 fax; [email protected] Spanish Translation of Abstracts: BORJA MILA, Museo Nacional de Ciencias Naturales, CSIC, José Gutiérrez Abascal 2, Madrid 28006, Spain; [email protected] Layout and Typesetting: PRISCILLA YOCOM, 5018 Albridal Way, San Ramon, CA 94582 THE INSTITUTE FOR BIRD POPULATIONS A tax-exempt California nonprofit corporation established in 1989 and dedicated to fostering a global approach to research and the dissemination of information on changes in bird populations. President: DAVID F. DESANTE , P.O. Box 1346, Point Reyes Station, CA 94956 Secretary-Treasurer: STEPHEN M. ALLAN, 962 Mistletoe Loop N, Keizer, OR 97303 Directors: CORDELL GREEN, IVAN SAMUELS, RODNEY B. SIEGEL, and DAN TOMPKINS All persons interested in birds are invited to join The Institute for Bird Populations. Individual membership dues are $35 per year. Institutional memberships are $50 per year; student and senior memberships are $15 per year. Please send check or money order (in U.S. dollars) payable to The Institute for Bird Populations, along with complete name, address, and email address to: The Institute for Bird Populations, P.O. -
Bird Watching Tour to Bhigwan | World Wetlands Day
Bird Watching Tour to Bhigwan | World Wetlands Day About This Experience On the occasion of World Wetlands Day which is celebrated on 2 February, Rupa Rahul Bajaj Centre for Environment & A (RRBCEA) is organizing a Bird Watching Tour to Bhigwan located on the backwaters of the Ujani Dam on the Bhima River about 100 km East of Pune. It is well known for aracting a large number of migratory waterbirds in the winter along with the Greater Flamingos. Almost 300 species of birds have been recorded from Bhigwan. Join us on this Wetland Day let us explore Bhigwan and learn about the impoance of large wetlands as impoant bird habitats. The tour will be led by ecologist Kedar Champhekar and organized by The Western Routes. Who Should Aend ? This leisurely day-trip is peect for people of all ages. If you want to know more about birds and the ecology, this is a peect trip for you! Highlights - Bird Watching with Expes - Chance to spot amingos and many other migratory birds - Boat Ride - Rusitc Lunch Duration : 1 Day Experiences : Hobby Trips Photography Couple Friendly Travel & Work Local Events Wildlife Leisure And Travel Weekend Getaways Location : Adults : ₹ 1900/- Kumbhargaon Birds Sanctuary, Kumbhargaon, Kids(5-10 years) : ₹ 1700/- Maharashtra, India INCLUSIONS AND EXCLUSIONS INCLUSIONS EXCLUSIONS - All travel in an AC bus - Personal expenses (Cold drinks, mineral - Breakfast & Lunch water etc.) - Boat Ride Charges at the Ujani Dam - Anything not mentioned in the 'includes' backwaters list - Expeise Charges - Travel Insurance - All taxes PICK UP POINTS Empress Garden Main Gate Fergusson College Main Gate ENQUIRE NOW For any help, contact : Key Contact Person : Prachi ( 9405591758 ) The Western Routes : 9405591758 Logout.World helpline : +91 906 706 8192 Powered By : THE PLAN IN DETAIL What we will do ? Private Vehicle Stay Not Applicable Breakfast, Lunch AC Bus - 5:30 AM - Assemble at Fergusson College Main Gate (Parking space available for cars and bikes on the road). -

Eco-Tourism – a Key to Protect the Biodiversity in Maharashtra
ISSN: 2319-8753 International Journal of Innovative Research in Science, Engineering and Technology (An ISO 3297: 2007 Certified Organization) Vol. 3, Issue 8, August 2014 Eco-Tourism – A Key to Protect the Biodiversity in Maharashtra Dr. Vandana M. Joshi, Lecturer, Department of Travel and Tourism, Maharashtra State Institute of Hotel Management and Catering Technology, Pune, India ABSTRACT: Biodiversity is an asset to tourism and it varies greatly across the globe. It is vital in maintenance of a healthy ecosystem. From the last couple of decades biodiversity has been affected due to rapid urbanization. Various efforts are made to conserve the biodiversity; one of them is protected areas which are reserved for rare and endangered species of flora and fauna. Maharashtra has up to 15,732 sq km reserved forest which is about 5.02 per cent of the State‟s geographical area. Maharashtra is rich with varied biodiversity ranging from forests, wetland, grassland to coast and evergreen forest. Natural site, Kaas in Western Ghats has been included in the World Heritage Site list by UNESCO. Conservation of endangered and rare species of flora and fauna is a challenge in developing countries as rules and regulations are not strictly followed. Ecotourism is the key to conserve the endangered species because it is referred to as sustainable nature based tourism. It incorporates tourism in harmony with nature. Further it provides opportunities for tourists to experience and explore the powerful manifestation of nature. It also emphasizes the utmost necessity of protection of biodiversity and local culture. Ecotourism helps in economic development of area through employment generation. -

Master Page.P65
BI-MONTHLY PROGRAMME JANUARY - FEBRUARY 2011 Index Director’s Letter ................................................................................................................................ 2 Secretary’s letter ............................................................................................................................... 4 10th Jan “Exploring the World of the Snow Leopard” – a slide show presentation by Dr Kaustubh Sharma: ................................................................................................... 5 16th Jan Birding in forested hill - Kanakeshwar .......................................................................... 5 23rd Jan Akshi shore birding ....................................................................................................... 5 29th Jan Mingle with migratory birds - Nerul Mudflats ................................................................ 5 30th Jan Matheran Nature Trek .................................................................................................. 5 6th Feb Know the rare trees of Jeejamata Udyan ..................................................................... 5 4 - 6 Feb Bhigwan Bird watching camp - IBA and potential Ramsar Site .................................... 6 12th Feb Karnala Bird Sanctuary Nature Trail ............................................................................. 6 13th Feb Sarasgad Nature Trek .................................................................................................. 6 19th Feb Flamingo