The First Decade of Roll Back Malaria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fossil Fuel Racism How Phasing out Oil, Gas, and Coal Can Protect Communities
© Les Stone / Greenpeace Fossil Fuel Racism How Phasing Out Oil, Gas, and Coal Can Protect Communities PUBLISHED: APRIL 13, 2021 www.greenpeace.org/usa/fossil-fuel-racism Contents Executive Summary . 1 Introduction . 5 1 . Environmental Justice . 7 2 . Fossil Fuels and Air Pollutants . 10 AUTHORS 3 . Fossil Fuel Phaseout . 12 Tim Donaghy, Ph.D. 4 . Extraction . 15 Charlie Jiang Oil and Gas Extraction . 15 Coal Mining . 18 CONTRIBUTORS Colette Pichon Battle, Esq. 5 . Processing & Transport . 19 Emma Collin Oil Refining, Natural Gas Processing & Petrochemical Manufacturing . 19 Janet Redman Pipelines & Terminals . 23 Ryan Schleeter 6 . Combustion . 24 General Exposure to Criteria Air Pollution . 24 SPECIAL THANKS TO Coal and Natural Gas Power Plants . 25 Noel Healy Aidan Farrow Mobile Sources and Traffic Exposure . 26 Anusha Narayanan 7 . Climate Impacts . 28 Ashley Thomson 8 . Policy Recommendations . 30 Caroline Henderson Charlie Cray 1. End fossil fuel racism and reverse the legacies of historical injustices . 30 Jonathan Butler 2. Phase out fossil fuel production . 31 Angela Mooney D’Arcy 3. Ensure no worker or community is left behind . 31 Michael Ash 4. Enact a green and just economic recovery . 31 EDITOR 5. Protect and expand our democracy to make it work for all people . 32 Charlie Jiang Acknowledgments . 33 Endnotes . 34 DESIGNED BY Kyle McKibbin Cover image by Les Stone © Robert Visser / Greenpeace This report is endorsed by: Alliance of Nurses for Healthy Environments ...and more. See the full list at: http://greenpeace.org/usa/fossil-fuel-racism FOSSIL FUEL RACISM | II Executive Summary Fossil fuels — coal, oil, and gas — lie at the heart of the crises we face, including public health, racial injustice, and climate change. -

Womanfwoman1-5,991,992Rev8
Women for Women International 2009 Annual Report In 2009, Women For Women International: • Served 85,458 women through our core program and microcredit. • Distributed $16.6 million in direct aid and microcredit loans. • Facilitated the exchange of 104,787 letters between sponsors and their sisters. • Revised our core rights awareness and life skills curriculum to deepen program impact and equip women with tools to rebuild their lives, families and communities. • Implemented new country-specific income generation and employment strategies, including market-based vocational and business skills trainings and pilot projects linked to the consumer value-chain. • Developed innovative public-private partnerships to help women access the knowledge and resources they need to lead long-term change. From the Chair of the Board of Directors As the Chair of Women for Women International’s Board of Monitoring and Evaluation systems will ensure effective Directors, I want to thank you for making it possible for and efficient data collection relevant to women’s economic Women for Women International to remain a lifeline to status, decision-making abilities, physical and psychological women in one of the most economically turbulent times in wellness, and social networks. recent history. In 2009, as most charities saw a significant reduction in donations and grant revenue, your steadfast Publicly, we were granted special consultative status with support allowed us to continue uniting our global community the United Nations Economic and Social Council, and we and fostering stability for women survivors of war as they expanded our European presence through successful UK- rebuild their lives, families and communities. based advocacy and outreach. -
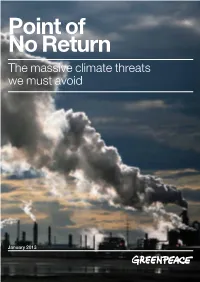
Point of No Return the Massive Climate Threats We Must Avoid
Point of No Return The massive climate threats we must avoid January 2013 © LU GUANG / GREENPEACE Contents #1 Executive summary 4 #2 The world’s biggest dirty energy projects 10 #3 Calculating the impact of the dirtiest energy projects 16 #4 Overshooting 2°C: A world we don’t want 22 #5 Clean solutions for the power sector 26 #6 The vision of the Energy [R]evolution can achieve results 34 #7 Action! 36 Appendix 40 Endnotes 54 For more information contact: [email protected] Written by: Ria Voorhar & Lauri Myllyvirta Edited by: Brian Blomme, Steve Erwood, Xiaozi Liu, Nina Schulz, Stephanie Tunmore, James Turner Acknowledgements: Ben Ayliffe, Ricardo Bartelo, Arif Fiyanto, Paul Johnston, Harri Lammi, Kelly Mitchell, Renata Nitta, Deng Ping, Sun Qingwei, Keith Stewart, Aslihan Tumer, Georgina Woods Creative Design and Direction: Sue Cowell / Atomo Design www.atomodesign.nl Cover photograph: © Paul Langrock / Greenpeace JN 437 Published in January 2013 by Greenpeace International Ottho Heldringstraat 5 1066 AZ Amsterdam The Netherlands greenpeace.org Image Smoke from factories causes severe air pollution in Huolin Gol city, Inner Mongolia, whose economy relies heavily on coal-related industries. “In 2020, the emissions from the 14 projects showcased in this report – if they were all to go ahead – would raise global CO2 emissions from fossil fuels by 20% and keep the world on a path towards 5°C to 6°C of warming.” Point of No Return The massive climate threats we must avoid 3 section one Image Traffic moves through billowing smoke and lingering, passing by oil refineries in Alberta, Canada. -
The First Decade of Roll Back Malaria
PROGRESS & IMPACT SERIES Number 1 . March 2010 Malaria Funding & Resource Utilization: The First Decade of Roll Back Malaria WHO Library Cataloguing-in-Publication Data Malaria funding and resource utilization: the first decade of Roll Back Malaria. 1.Malaria - prevention and control. 2.Malaria - therapy. 3.Financing, health. 4.Program evaluation. 5.International cooperation. I.Global Partnership to Roll Back Malaria. II.Johansson, Emily White. III.Cibulskis, R. E. IV.Steketee, Richard W. ISBN 978 92 4 159916 0 (NLM classification: WC 765) © 2010 World Health Organization on behalf of the Roll Back Malaria Partnership Secretariat All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, Avenue Appia 20, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). Some photographs are subject to licensing fees and may not be reproduced freely; all photo enquiries should be addressed to the Roll Back Malaria Partnership Secretariat at the address listed below. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization, the Roll Back Malaria Partnership Secretariat or any of its individual Partners concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

2013 Fiscal Year Annual Report
2013 Annual Report Red Cross emergency response vehicles are loaded with hot meals for the nightly dinner run through Long Island, N.Y., after Superstorm Sandy. Mission Statement The American Red Cross prevents and alleviates human suffering in the face of emergencies by mobilizing the power of volunteers and the generosity of donors. Principles of the International Red Cross and Red Crescent Network Humanity • Impartiality • Neutrality • Independence • Voluntary service • Unity • Universality Cover photo: At a Red Cross shelter in Toms River, N.J., a teenager finds refuge after Superstorm Sandy. © 2013 The American National Red Cross A Message From the Chairman Looking back on the past year, one word comes to mind: resiliency. People in communities across the United States—from the Jersey shore to the California canyons— faced difficulties in the form of disasters of every kind…natural and human-caused. And in the aftermath of these hardships, people banded together, not only for survival, but to help their communities become even stronger. This spirit of triumph over adversity is indispensable when disaster strikes. The American Red Cross is privileged to work shoulder to shoulder through the entire disaster cycle…helping people prepare for emergencies, providing essential services when disasters strike, and then assisting families and communities as they begin their recovery and build resiliency for the future. Thanks to the incredible generosity of the American public and our volunteers and partners who make everything we do possible, the Red Cross was there last year, offering help and hope in the aftermath of disasters. This included major disasters such as Superstorm Sandy, the devastating tornadoes in Oklahoma, and wildfires in the West. -

2012 Calendar of Events and Resource Guide
CALENDAR OF EVENTS JANUARY 25 — MARCH 17, 2012 2012 2012 WELCOME One Book, One Philadelphia isw a EjointLCOM projectE From of the t Mayor’sHE cHair Office pgand 3 the Free Library of Philadelphia. The mission ofa thebout program tHE isa utto promoteHors reading,pg 4 literacy, library usage, and community building throughout Greater Philadelphia. additional rEading suggEstions pg 5 discussion QuEstions pg 6 feat One BOOk discussion groups pg 7 gEnEral EvEnts pg 8 EvENTS witH EDWIDGE DANTICAT pg 12 EvEnts For cHildrEn and FamiliEs pg 14 bEyond One BOOk pg 18 u acknowlEdgEmEnts pg 19 The centerpiece of 2012 One Book, One Philadelphia is a stirring collection of RED essays and memoir, Edwidge Danticat’s Create Dangerously: The Immigrant Artist at Work. While telling deeply moving stories of Haitian artists, heroes, and everyday people—including members of Danticat’s own family—the award-winning author makes an impassioned case for immigrant writers T and artists to bear witness against oppression in their countries of origin, i Create Dangerously: sometimes imperiling their own and their readers’ lives. Danticat’s focus on TLES The Immigrant Artist at Work the reading and writing of important truths makes this book an apt choice by EdwidgE danticat for One Book, One Philadelphia’s 10th anniversary. As with all outstanding literature, Create Dangerously provides a reading experience that will Create Dangerously: The Immigrant Artist at Work transport Philadelphians across borders of the imagination, where they will is a collection of essays that reflects on art and exile, recognize their own selves in the lives of people from other circumstances exploring what it means to be an immigrant artist and places. -
Taxing Carbon (And Boosting the Economy) We See More Than a Risk Tolerance
Engineering Life • Francis Parkman • Public Speaking September-OctOber 2014 • $4.95 Taxing Carbon (and boosting the economy) We see more than a risk tolerance. At Fiduciary Trust we understand that life is about balancing risks and rewards. Let us design a financial strategy that grows and protects your wealth—so you can enjoy all that life has to offer. PLEASE CONTACT RANDY KINARD AT 617.574.3432 FIDUCIARYTRUSTBOSTON.COM INVESTMENT MANAGEMENT | TRUST SERVICES | FINANCIAL AND ESTATE PLANNING | FAMILY OFFICE SERVICES | ESTATE SETTLEMENT 140905_FiduciaryTrust.indd 1 7/14/14 3:10 PM SEPTEMBER-OCTOBER 2014 VOLUME 117, NUMBER 1 FEATURES 37 The Lowell Speeches Project | by Michael Zuckerman Undergraduates build community through a public-speaking program in their House 42 Synthetic Biology’s New Menagerie | by Katherine Xue The life sciences as an engineering discipline 50 Vita: Francis Parkman | by Castle Freeman Jr. p. 17 Brief life of America’s epic historian: 1823-1893 52 Time to Tax Carbon | by Jonathan Shaw Dale Jorgenson points the way toward controlling greenhouse gases while enhancing economic growth JOHN HARVard’s JournAL 17 Installing a bell on high, Dunster House deconstruction, endowment’s changing cast and challenges, tooth tales, fitting up Quincy House, faculty survey, Loeb Classical Library online, Tibetan texts digitized, scholars speaking out, math and science awards, an honorand’s passing, online education blends in, the Undergraduate pursues his passion, new editorial fellows, Crimson cornerback, and “Cleat” laterals DEPARTMENTS -
The Kingpins of Carbon and Their War on Democracy
Page 1 The Kingpins of Carbon and Their War on Democracy ©Tim Aubry/Greenpeace Page 2 The Kingpins of Carbon and Their War on Democracy published by: Greenpeace US September 2014 all photos © Greenpeace Written by: Charlie Cray and Peter Montague Charlie Cray is a Research Specialist for Peter Montague, Ph.D., is a journalist and histo- Greenpeace US. Research assistance rian living in New Brunswick, N.J., where he is provided by Skyler Kopko and Connor active in the New Jersey Environmental Justice Gibson. Alliance. He is a member of the National Writer’s Union (UAW Local 1981, AFL-CIO), the NAACP, Greenpeace, and Sierra Club, and a fellow with the Science and Environmental Health Network in Ames, Iowa. © Les Stone /Greenpeace Page 3 The Kingpins of Carbon and Their War on Democracy Abstract Global warming is a potentially devastating problem requiring urgent action by governments. However, to date the U.S. government has remained largely paralyzed. Now new Greenpeace research has shed light on the sources of paralysis, a multi-decade war on democracy by the kingpins of carbon – the coal, oil, and gas industries allied with a handful of self-interested libertarian1 billionaires. Their strategy has aimed to (1) shrink, disable and paralyze progressive government and (2) manipulate the remaining levers of government power by (a) eliminating all restrictions on private money in elections and (b) disenfranchis- ing blacks, Latinos, the young, the elderly, and the disabled, all of whom are presumed to favor Democrats. Since 1975, their strategy has rolled back New Deal programs, weakened labor unions, and reversed victories of the civil rights movement, undermining the strength and cohesion of the middle class, further enriching and empowering a tiny self-interested elite. -

ISSAACC BAIL EY the Sussun N Newsw , Myrttrtlel Beae Ch, , S.S C
NIEMAN REPORTS ISSAAC BAILEY The SuS n Newsw , Myrttlel Beae ch, S.S C.C nr_spring_2015_covers_spine.indd 1 6/22/15 10:49 AM Contributors The Nieman Foundation for Journalism at Harvard University (page 18), a 2014 Nieman www.niemanreports.org Issac Bailey Fellow, is a metro columnist and senior writer for The Sun News in Myrtle Beach, South Carolina. He was a 2011 recipient of a Casey Medal for Meritorious Journalism for stories about a child protection case. The state subsequently publisher revamped the way it handles such cases. Ann Marie Lipinski editor Susan Smith Richardson (page 26), James Geary a 2003 Nieman Fellow, is the editor and senior editor publisher of The Chicago Reporter, a Jan Gardner nonprofi t investigative news organization that focuses on race, poverty, and income researcher/reporter inequality in the city. She has worked Jonathan Seitz at The Texas Observer, the Chicago editorial assistants Tribune, and The Sacramento Bee. Eryn M. Carlson Tara W. Merrigan Zun Lee (page 26) is a self-taught Laura Mitchell photographer who picked up a camera design in 2009. His Father Figure series of Pentagram photographs is the basis for his book editorial offices “Father Figure: Exploring Alternate One Francis Avenue, Cambridge, Notions of Black Fatherhood,” published MA 02138-2098, 617-496-6308, in 2014. Images in the series have been [email protected] exhibited in Toronto and Paris. Copyright 2015 by the President and Fellows of Harvard College. Alicia W. Stewart (page 34), a 2015 Periodicals postage paid at Nieman Fellow, most recently was an Boston, Massachusetts and editor at CNN.com. -

At the Everhart Museum in Scranton
EVERHART MUSEUM NATURAL HISTORY, SCI E N C E & A R T 1901 Mulberry Street, Scranton, PA 18510 [tel] 570-346-7186 [fax] 570-346-0652 [web] www.everhart-museum.org For Immediate Release Press Photographs are Available Upon Request Contact: Lauren White at 570-346-7186 or [email protected] New Exhibit Celebrating Heritage, Art & Culture in the Americas Opens September 25th at the Everhart Museum in Scranton Scranton – August 19, 2009: The Everhart Museum will open Day of the Dead: Art & Culture in the Americas on September 25, 2009. Created by the Everhart Museum, this exhibit illustrates the Day of the Dead (El Día de los Muertos) holiday as a personal and community-based celebration focused on the remembrance of family, friends, and other beloved people. The exhibit highlights the rich cultures of Central and South America by showcasing contemporary art from nationally and internationally recognized artists and photographers, along with Latino folk art and selections from the Museum’s ethnographic collections. Day of the Dead: Art & Culture in the Americas is exclusive to the Everhart and will be on display through December 31, 2009. The exhibition is funded in part by a grant from The Pennsylvania Humanities Council, with additional underwriting from the Foley Law Firm, Gertrude Hawk Chocolates, Inc. and Prudential Retirement. While Mexico is perhaps best-known for their Day of the Dead celebration, many other Latin American and Caribbean countries honor their ancestors on this holiday, including Brazil, Guatemala, Haiti, Martinique, and Peru. The Day of the Dead occurs on November 1st and 2nd in connection with the Roman Catholic observances of All Saints’ Day and All Souls’ Day. -

Soros Foundations Network 2003 Annual
Building Open Societies SOROS FOUNDATIONS NETWORK 2003 REPORT The Open Society Institute, a private operating and grantmaking foundation, aims to shape public policy to promote democratic governance, human rights, and economic, legal, and social reform. On a local level, OSI implements a range of initiatives to support the rule of law, education, public health, and independent media. At the same time, OSI works to build alliances across borders and continents on issues such as combating corruption and rights abuses. OSI was created in 1993 by investor and philanthropist George Soros to support his foundations in Central and Eastern Europe and the former Soviet Union. Those founda- tions were established, starting in 1984, to help countries make the transition from communism. OSI has expanded the activities of the Soros foundations network to other areas of the world where the transition to democracy is of particular concern. The Soros foundations network encompasses more than 60 countries, including the United States. www.soros.org Building Open Societies SOROS FOUNDA TIONS NETWORK 2003 REPORT OPEN SOCIETY INSTITUTE 400 West 59th Street, New York, NY 10019 USA www.soros.org Building Open Societies: Soros Foundations Network 2003 Report Copyright © 2004 by the Open Society Institute 400 West 59th Street, New York, NY 10019 USA All rights reserved, including the right to reproduce this book or portions thereof in any form. CONTENTS PRESIDENT’S MESSAGE 6 America’s Waning Influence as an Open Society REGIONS 14 Middle East 16 20 Iraq: photographed -

Vol. 15 No 30 Aug 8 2019
VOL. 15 NO. 30 GRAHAMSVILLE, NY 12740 AUGUST 8, 2019 FIFTY CENTS • Local Weather Pg 8 • Mysterious Book Report John D. McKenna Pg 4 • The Olive Jar Carol La Monda Pg 6 • The Scene Too Jane Harrison Pg 11 Sullivan County Dramatic Workshop 2019 Productions - See ad on Page 16 The Pictures...and the Stories Continue Albi Performs at the Russian Mule Last summer Keiko Sono, coordinator of the Catskill Waters community began an art proj- Many local faces (past and present) were ect, Portraits and Stories, at the Blue Hole in Sundown. She recorded converstions of visi- in the audience at the Russian tors and residents to the Tri-Valley watershed area. While telling their stories artist, Jenny Mule/Claryville Event Center and listened Lee Fowler cut a silhouette portrait of the ‘story tellers’. and danced to the music of Albi. Tiny tots joined their parents on the dance floor, while most of us were content to sit back, relax, have some good food and listen to Albi. Among the audience was Larry Balestra, and his wife Kathy.. There were three more local sessions – one at the Neversink General Store, one at the Claryville Church Hall and then back to Sundown at the Church Hall. This past Saturday a reception was hosted by the Neversink General Store and held in the `Larry is also a musician. What made his appearance so special? He was one of Pit Stop Art Gallery for those who participated in the program and told their stories. The ele- Albi’s music teachers back in the day.