SCLRPH Final Compilation of Meeting Agendas and Minutes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mass. Bill Proposed to Provide Medical Service to On-Duty Animals
Mass. bill proposed to provide medical service to on-duty animals The bill would allow EMS workers to treat K-9s injured in the line of duty Yesterday at 9:51 AM Kathleen McKiernan Boston Herald BOSTON — Police are praising proposed legislation that would allow emergency medical service workers to treat police canines injured in the line of duty, calling it a common-sense move that would save dogs serving the community. “We owe it to an animal we are pulling into service to do the best we can,” Yarmouth Police Chief Frank Frederickson said. “It’s common sense.” Barnstable Representative William L. Crocker, Jr., is sponsoring a bill that would allow first responders to treat police dogs injured on the job. Right now, Massachusetts laws penalize emergency medical technicians if they assist an animal in an emergency. The proposal prioritizes humans requiring medical attention before animals receive care, and absolves emergency personnel from liability. It also allows for licensed veterinarians to provide written guidelines or provide consultation with EMTs providing animal care, and similarly gives those vets protection from post-incident liability. Nine other legislators — Representatives Brian Ashe of Hampden, Shawn Dooley of Norfolk, Dylan Fernandes of Barnstable, Dukes and Nantucket, Susan Williams Gifford of Plymouth, Hannah Kane of Worcester, David Muradian Jr. of Worcester, Sarah Peake of Barnstable and Timothy Whelan of Barnstable; and Sen. Julian Cyr of Cape & Islands — support the bill. The proposal comes after Nero, a Yarmouth Police K9, was hospitalized for a week after he was shot in the face in a deadly incident in April. -

The General Court of the Commonwealth of Massachusetts State House, Boston, MA 02133-1053
The General Court of the Commonwealth of Massachusetts State House, Boston, MA 02133-1053 April 7, 2020 David L. Bernhardt, Secretary U.S. Department of the Interior 1849 C Street, N.W. Washington DC 20240 Dear Secretary Bernhardt, We are deeply dismayed and disappointed with the Department of the Interior's recent decision to disestablish and take lands out of trust for the Mashpee Wampanoag Tribe on March 27, 2020. Not since the mid-twentieth century has an Interior Secretary taken action to disestablish a reservation. This outrageous decision comes as we mark 400 years since the arrival of the Pilgrims in 1620 and recognize the People of the First Light who inhabited these shores for centuries before contact. The Department’s capricious action brings shame to your office and to our nation. Your decision was cruel and it was unnecessary. You were under no court order to take the Wampanoag land out of trust. Further, litigation to uphold the Mashpee Wampanoag’s status as a tribe eligible for the benefits of the Indian Reorganization Act is ongoing. Your intervention was without merit and completely unnecessary. The fact that the Department made this announcement on a Friday afternoon in the midst of the COVID-19 pandemic demonstrates a callous disregard for human decency. Mashpee Wampanoag leaders were focused on protecting members of their tribe, mobilizing health care resources, and executing response plans when they received your ill-timed announcement. As you are well aware, the Department of the Interior holds a federal trust responsibility to tribes, which includes the protection of Native American lands. -

HOUSE ...No. 1132
HOUSE DOCKET, NO. 2450 FILED ON: 2/17/2021 HOUSE . No. 1132 The Commonwealth of Massachusetts _________________ PRESENTED BY: Hannah Kane and Jack Patrick Lewis _________________ To the Honorable Senate and House of Representatives of the Commonwealth of Massachusetts in General Court assembled: The undersigned legislators and/or citizens respectfully petition for the adoption of the accompanying bill: An Act relative to emergency insulin access. _______________ PETITION OF: NAME: DISTRICT/ADDRESS: DATE ADDED: Hannah Kane 11th Worcester 2/17/2021 Jack Patrick Lewis 7th Middlesex 2/17/2021 Colleen M. Garry 36th Middlesex 2/17/2021 Joseph D. McKenna 18th Worcester 2/17/2021 Christopher Hendricks 11th Bristol 2/18/2021 Lindsay N. Sabadosa 1st Hampshire 2/18/2021 Steven G. Xiarhos 5th Barnstable 2/18/2021 Tricia Farley-Bouvier 3rd Berkshire 2/22/2021 Tami L. Gouveia 14th Middlesex 2/22/2021 Brian M. Ashe 2nd Hampden 2/23/2021 David Henry Argosky LeBoeuf 17th Worcester 2/23/2021 Mathew J. Muratore 1st Plymouth 2/24/2021 Kimberly N. Ferguson 1st Worcester 2/26/2021 Jonathan D. Zlotnik 2nd Worcester 2/26/2021 Bradley H. Jones, Jr. 20th Middlesex 2/26/2021 Andres X. Vargas 3rd Essex 2/26/2021 Angelo L. D'Emilia 8th Plymouth 3/10/2021 David F. DeCoste 5th Plymouth 3/14/2021 1 of 2 Steven S. Howitt 4th Bristol 3/15/2021 Steven C. Owens 29th Middlesex 6/1/2021 2 of 2 HOUSE DOCKET, NO. 2450 FILED ON: 2/17/2021 HOUSE . No. 1132 By Representatives Kane of Shrewsbury and Lewis of Framingham, a petition (accompanied by bill, House, No. -
MA CCAN 2020 Program FINAL
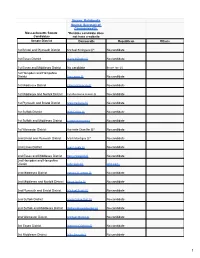
Source: Ballotpedia Source: Secretary of Commonwealth Massachusetts Senate *Denotes candidate does Candidates not have a website Senate District Democratic Republican Others 1st Bristol and Plymouth District Michael Rodrigues (i)* No candidate 1st Essex District Diana DiZoglio (i) No candidate 1st Essex and Middlesex District No candidate Bruce Tarr (i) 1st Hampden and Hampshire District Eric Lesser (i) No candidate 1st Middlesex District Edward Kennedy (i) No candidate 1st Middlesex and Norfolk District Cynthia Stone Creem (i) No candidate 1st Plymouth and Bristol District Marc Pacheco (i) No candidate 1st Suffolk District Nick Collins (i) No candidate 1st Suffolk and Middlesex District Joseph Boncore (i) No candidate 1st Worcester District Harriette Chandler (i)* No candidate 2nd Bristol and Plymouth District Mark Montigny (i)* No candidate 2nd Essex District Joan Lovely (i) No candidate 2nd Essex and Middlesex District Barry Finegold (i) No candidate 2nd Hampden and Hampshire District John Velis (i) John Cain 2nd Middlesex District Patricia D. Jehlen (i) No candidate 2nd Middlesex and Norfolk District Karen Spilka (i) No candidate 2nd Plymouth and Bristol District Michael Brady (i) No candidate 2nd Suffolk District Sonia Chang-Diaz (i) No candidate 2nd Suffolk and Middlesex District William Brownsberger (i) No candidate 2nd Worcester District Michael Moore (i) No candidate 3rd Essex District Brendan Crighton (i) No candidate 3rd Middlesex District Mike Barrett (i) No candidate 1 Source: Ballotpedia Source: Secretary of Commonwealth -

SNAP Gap Cosponsors - H.1173/S.678 91 Representatives & 28 Senators
SNAP Gap Cosponsors - H.1173/S.678 91 Representatives & 28 Senators Rep. Jay Livingstone (Sponsor) Representative Daniel Cahill Representative Jack Patrick Lewis Senator Sal DiDomenico (Sponsor) Representative Peter Capano Representative David Linsky Senator Michael Barrett Representative Daniel Carey Representative Adrian Madaro Senator Joseph Boncore Representative Gerard Cassidy Representative John Mahoney Senator William Brownsberger Representative Michelle Ciccolo Representative Elizabeth Malia Senator Harriette Chandler Representative Mike Connolly Representative Paul Mark Senator Sonia Chang-Diaz Representative Edward Coppinger Representative Joseph McGonagle Senator Jo Comerford Representative Daniel Cullinane Representative Paul McMurtry Senator Nick Collins Representative Michael Day Representative Christina Minicucci Senator Brendan Crighton Representative Marjorie Decker Representative Liz Miranda Senator Julian Cyr Representative David DeCoste Representative Rady Mom Senator Diana DiZoglio Representative Mindy Domb Representative Frank Moran Senator James Eldridge Representative Daniel Donahue Representative Brian Murray Senator Ryan Fattman Representative Michelle DuBois Representative Harold Naughton Senator Paul Feeney Representative Carolyn Dykema Representative Tram Nguyen Senator Cindy Friedman Representative Lori Ehrlich Representative James O'Day Senator Anne Gobi Representative Nika Elugardo Representative Alice Peisch Senator Adam Hinds Representative Tricia Farley-Bouvier Representative Smitty Pignatelli Senator -

HOUSE ...No. 3224
HOUSE DOCKET, NO. 3776 FILED ON: 2/19/2021 HOUSE . No. 3224 The Commonwealth of Massachusetts _________________ PRESENTED BY: Maria Duaime Robinson and Tricia Farley-Bouvier _________________ To the Honorable Senate and House of Representatives of the Commonwealth of Massachusetts in General Court assembled: The undersigned legislators and/or citizens respectfully petition for the adoption of the accompanying bill: An Act relative to virtual meetings of appointed statewide public bodies. _______________ PETITION OF: NAME: DISTRICT/ADDRESS: DATE ADDED: Maria Duaime Robinson 6th Middlesex 2/19/2021 Tricia Farley-Bouvier 3rd Berkshire 2/19/2021 Mindy Domb 3rd Hampshire 2/24/2021 Carmine Lawrence Gentile 13th Middlesex 2/24/2021 Kate Lipper-Garabedian 32nd Middlesex 2/26/2021 Christina A. Minicucci 14th Essex 2/26/2021 Mary S. Keefe 15th Worcester 2/26/2021 Patrick Joseph Kearney 4th Plymouth 2/26/2021 Michael J. Barrett Third Middlesex 2/26/2021 David Henry Argosky LeBoeuf 17th Worcester 2/26/2021 James B. Eldridge Middlesex and Worcester 2/26/2021 Bradley H. Jones, Jr. 20th Middlesex 2/27/2021 Hannah Kane 11th Worcester 3/31/2021 Jack Patrick Lewis 7th Middlesex 5/25/2021 1 of 1 HOUSE DOCKET, NO. 3776 FILED ON: 2/19/2021 HOUSE . No. 3224 By Representatives Robinson of Framingham and Farley-Bouvier of Pittsfield, a petition (accompanied by bill, House, No. 3224) of Maria Duaime Robinson, Tricia Farley-Bouvier and others relative to virtual meetings of appointed statewide public bodies. State Administration and Regulatory Oversight. The Commonwealth of Massachusetts _______________ In the One Hundred and Ninety-Second General Court (2021-2022) _______________ An Act relative to virtual meetings of appointed statewide public bodies. -

HOUSE ...No. 2267
HOUSE DOCKET, NO. 2928 FILED ON: 2/18/2021 HOUSE . No. 2267 The Commonwealth of Massachusetts _________________ PRESENTED BY: Mindy Domb and Kimberly N. Ferguson _________________ To the Honorable Senate and House of Representatives of the Commonwealth of Massachusetts in General Court assembled: The undersigned legislators and/or citizens respectfully petition for the adoption of the accompanying bill: An Act prohibiting non consensual pelvic examinations. _______________ PETITION OF: NAME: DISTRICT/ADDRESS: DATE ADDED: Mindy Domb 3rd Hampshire 2/8/2021 Kimberly N. Ferguson 1st Worcester 2/18/2021 Kay Khan 11th Middlesex 2/19/2021 Tami L. Gouveia 14th Middlesex 2/22/2021 Christina A. Minicucci 14th Essex 2/22/2021 Patrick Joseph Kearney 4th Plymouth 2/22/2021 Natalie M. Blais 1st Franklin 2/22/2021 David Henry Argosky LeBoeuf 17th Worcester 2/23/2021 Lori A. Ehrlich 8th Essex 2/24/2021 Kathleen R. LaNatra 12th Plymouth 2/24/2021 Tommy Vitolo 15th Norfolk 2/25/2021 David Allen Robertson 19th Middlesex 2/26/2021 Tram T. Nguyen 18th Essex 2/26/2021 Kate Lipper-Garabedian 32nd Middlesex 2/26/2021 Susannah M. Whipps 2nd Franklin 2/26/2021 John Barrett, III 1st Berkshire 2/26/2021 Sally P. Kerans 13th Essex 2/26/2021 Joanne M. Comerford Hampshire, Franklin and Worcester 3/4/2021 1 of 2 Hannah Kane 11th Worcester 3/15/2021 2 of 2 HOUSE DOCKET, NO. 2928 FILED ON: 2/18/2021 HOUSE . No. 2267 By Representatives Domb of Amherst and Ferguson of Holden, a petition (accompanied by bill, House, No. 2267) of Mindy Domb, Kimberly N. -

January 28, 2021 the Honorable Charles D. Baker Office of The
January 28, 2021 The Honorable Charles D. Baker Office of the Governor Massachusetts State House Boston, MA 02133 Dear Governor Baker: We write to you to express our concern regarding the current process available to the public to sign up for COVID-19 vaccines. Our constituencies have called on us for assistance in navigating the pathway laid out by your Administration. The system in use, while made to be expedient and accessible, has created barriers for our aging population, those who have limited access to technology, and those who struggle to use it. Inadvertently, restricting the sign up process to a digital format puts our senior population at risk. In searching for the official online tool, the query also provides results not affiliated with the Commonwealth. This makes residents vulnerable to scams, and exposes them to undue online risks. Collectively, we implore the Administration to create a user friendly 1-800 number which would allow Massachusetts residents to access the sign up process more easily. Additionally, we request that the Administration create a centralized system, under the COVID-19 Task Force, that would allow for a more accessible sign-up process for those who can utilize the online tools. Currently, residents must choose a location, and then follow one of many links to separate entities to book appointments. We are appreciative for the steps that the Administration has taken, and are grateful for your consideration. Please contact our offices should you have questions, concerns, or wish to discuss this further. Sincerely, Anne M. Gobi Adam Gomez State Senator State Senator Worcester, Hampden, Hampshire Middlesex District Hampden District Eric P. -

Massachusetts State House, Room # (Fill in from List Below) Triton Legislative Delegation in YELLOW 24 Beacon Street Boston, MA 02133
MASSACHUSETTS STATE LEGISLATORS - REGIONAL SCHOOLS CAUCUS All Addressed To: Massachusetts State House, Room # (fill in from list below) Triton Legislative Delegation in YELLOW 24 Beacon Street Boston, MA 02133 FIRST LAST NAME TITLE AREA ROOM # EMAIL PHONE NAME Anne Gobi State Senator, Co-Chair Hampden, Hampshire, Worcester & Middlesex Room 513 [email protected] 617-722-1540 Kimberly Ferguson State Representative, Co-Chair 1st Worcester District Room 473B [email protected] 617-722-2263 Jennifer Benson State Representative 37th Middlesex District Room 22 [email protected] 617-722-2140 Donald Berthiaume State Representative 5th Worcester District Room 540 [email protected] 617-722-2090 Nicholas Boldyga State Representative 3rd Hampden District Room 167 [email protected] 617-722-2810 William Crocker State Representative 2nd Barnstable District Room 39 [email protected] 617-722-2014 Josh Cutler State Representative 6th Plymouth District Room 26 [email protected] 617-722-2080 Andelo D'Emilia State Representative 8th Plymouth District Room 548 [email protected] 617-722-2488 Shawn Dooley State Representative 9th Norfolk District Room 167 [email protected] 617-722-2810 Carolyn Dykema State Representative 8th Middlesex District Room 127 [email protected] 617-722-2680 Ryan Fattman State Senator Worcester & Norfolk Room 213A [email protected] 617-7221420 Carmine Gentile State Representative 13th Middlesex District Room 167 [email protected] -

MASC Legislative Directory 2020
2020 Massachusetts State Legislative Directory Massachusetts Constitutional Officers Governor Charlie Baker (617) 725-4005 Room 280 Lt. Governor Karyn Polito (617) 725-4005 Room 360 Treasurer Deborah Goldberg (617) 367-6900 Room 227 Atty. General Maura Healey (617) 727-2200 1 Ashburton Place, 18th Floor [email protected] Sec. of the State William Galvin (617) 727-9180 Room 340 [email protected] State Auditor Suzanne Bump (617) 727-2075 Room 230 [email protected] Massachusetts Senate (617) 722- Email (@masenate.gov) Room # (617) 722- Email (@masenate.gov) Room # Michael Barrett 1572 Mike.Barrett 109-D Patricia Jehlen 1578 Patricia.Jehlen 424 Joseph Boncore 1634 Joseph.Boncore 112 John Keenan 1494 John.Keenan 413-F Michael Brady 1200 Michael.Brady 416-A Edward Kennedy 1630 Edward.Kennedy 70 William Brownsberger 1280 William.Brownsberger 319 Eric Lesser 1291 Eric.Lesser 410 Harriette Chandler 1544 Harriette.Chandler 333 Jason Lewis 1206 Jason.Lewis 511-B Sonia Chang-Diaz 1673 Sonia.Chang-Diaz 111 Joan Lovely 1410 Joan.Lovely 413-A Nick Collins 1150 Nick.Collins 312-D Mark Montigny 1440 Mark.Montigny 312-C Joanne Comerford 1532 Jo.Comerford 413-C Michael Moore 1485 Michael.Moore 109-B Cynthia Creem 1639 Cynthia.Creem 312-A Patrick O'Connor 1646 Patrick.OConnor 419 Brendan Crighton 1350 Brendan.Crighton 520 Marc Pacheco 1551 Marc.Pacheco 312-B Julian Cyr 1570 Julian.Cyr 309 Rebecca Rausch 1555 Becca.Rausch 218 Sal DiDomenico 1650 Sal.DiDomenico 208 Michael Rodrigues 1114 Michael.Rodrigues 212 Diana DiZoglio 1604 Diana.DiZoglio 416-B -

S643/H2480) Lead Sponsors: Senators Lewis, Chandler & Welch, Representatives Vega & Chan
AN ACT TO PROMOTE PUBLIC HEALTH THROUGH THE PREVENTION & WELLNESS TRUST FUND (S643/H2480) Lead Sponsors: Senators Lewis, Chandler & Welch, Representatives Vega & Chan REPRESENTATIVES Dylan Fernandes Juana Matias SENATORS Brian Ashe Sean Garballey Joseph McKenna Michael Barrett Cory Atkins Denise Garlick Joan Meschino Michael Brady Bruce Ayers Carmine Gentile James Miceli William Brownsberger Ruth Balser Susan Gifford Rady Mom Harriette Chandler Christine Barber Solomon Goldstein-Rose David Muradian Sonia Chang-Diaz Jennifer Benson Carlos Gonzalez Matt Muratore Julian Cyr Donald Berthiaume Danielle Gregoire James Murphy Sal DiDomenic Antonio Cabral Stephan Hay Brian Murray James Eldridge Daniel Cahill Jonathan Hecht David Nangle Jennifer Flanagan Thomas Calter Paul Heroux Shaunna O'Connell Vinny deMacedo Kate Campanale Natalie Higgins James O'Day Linda Dorcena Forry James Cantwell Kate Hogan Sarah Peake Anne Gobi Gailanne Cariddi Russell Holmes Smitty Pignatelli Adam Hinds Evandro Carvalho Kevin Honan Denise Provost Donald Humason Gerard Cassidy Daniel Hunt Angelo Puppolo John Keenan Tackey Chan Hannah Kane David Rogers Eric Lesser Nick Collins Louis Kafka Byron Rushing Jason Lewis Mike Connolly Mary Keefe Daniel Ryan Barbara L'Italien Brendan Crighton Kay Khan Paul Schmid Joan Lovely Will Crocker Peter Kocot Frank Smizik Thomas McGee Claire Cronin Robert Koczera Todd Smola Michael Moore Daniel Cullinane Stephen Kulik William Straus Patrick O'Connor Mark Cusack John Lawn Jose Tosado James Welch Josh Cutler Jack Lewis Steven Ultrino Marjorie Decker David Linsky Aaron Vega REPRESENTATIVES = 93 David DeCoste Jay Livingstone David Vieira SENATORS = 23 Daniel Donahue Adrian Madaro Joseph Wagner TOTAL = 116 Michelle Dubois John Mahoney Chris Walsh Carolyn Dykema Elizabeth Malia Bud Williams Lori Ehrlich Paul Mark Tricia Farley-Bouvier Christopher Markey 1. -

Senate House Massachusetts House of Representatives
Senate House Massachusetts House of Representatives Representative Dylan Fernandes, (Barnstable, Dukes & Nantucket) Phone: (617) 722-2013 Email: [email protected] Cities: Nantucket, Falmouth, Chilmark, Aquinnah, Gosnold, Oak Bluffs, Tisbury, West Tisbury Representative Timothy Whelan, (1st Barnstable) Phone: (617) 722-2488 Email: [email protected] Cities: Dennis, Brewster, Yarmouth Representative Kip Diggs, (2nd Barnstable) Phone: (617) 722-2800 Email: [email protected] Cities: Barnstable, Yarmouth Representative David Vieira, (3rd Barnstable) Phone: (617) 722-2230 Email: [email protected] Cities: Teaticket (Falmouth), Bourne, Mashpee Representative Sarah Peake, (4th Barnstable) Phone: (617) 722-2040 Email:[email protected] Cities Provincetown, Chatham, Eastham, Harwich, Orleans, Truro, Wellfleet Representative Steven Xiarhos, (5th Barnstable) Phone: (617) 722-2800 Email: [email protected] Cities Sandwich, Barnstable, Bourne, Plymouth Representative John Barrett, (1st Berkshire) Phone: (617) 722-2305 Email: [email protected] North Adams, Adams, Clarksburg, Florida, Williamstown, Chesire, Hancock, Lanesborough, New Ashford Representative Paul Mark, (2nd Berkshire) Phone: (617) 722-2304 Email: [email protected] Bernardston, Colrain, Dalton, Hinsdale, Leyden, Northfield, Peru, Pittsfield, Savoy, Windsor, Greenfield, Charlemont, Hawley, Heath, Monroe, Rowe Representative Tricia Farley-Bouvier, (3rd Berkshire)