High Frequency Oscillatory Ventilation Anaesthesia Tutorial of the Week 261
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Effect of Spontaneous Breathing on Ventilator- Induced Lung Injury In
Xia et al. Critical Care 2011, 15:R244 http://ccforum.com/content/15/5/R244 RESEARCH Open Access Effect of spontaneous breathing on ventilator- induced lung injury in mechanically ventilated healthy rabbits: a randomized, controlled, experimental study Jingen Xia, Bing Sun, Hangyong He, Heng Zhang, Chunting Wang and Qingyuan Zhan* Abstract Introduction: Ventilator-induced lung injury (VILI), one of the most serious complications of mechanical ventilation (MV), can impact patients’ clinical prognoses. Compared to control ventilation, preserving spontaneous breathing can improve many physiological features in ventilated patients, such as gas distribution, cardiac performance, and ventilation-perfusion matching. However, the effect of spontaneous breathing on VILI is unknown. The goal of this study was to compare the effects of spontaneous breathing and control ventilation on lung injury in mechanically- ventilated healthy rabbits. Methods: Sixteen healthy New Zealand white rabbits were randomly placed into a spontaneous breathing group (SB Group) and a control ventilation group (CV Group). Both groups were ventilated for eight hours using biphasic positive airway pressure (BIPAP) with similar ventilator parameters: inspiration pressure (PI) resulting in a tidal volume (VT) of 10 to 15 ml/kg, inspiratory-to-expiratory ratio of 1:1, positive end-expiration pressure (PEEP) of 2 cmH2O, and FiO2 of 0.5. Inflammatory markers in blood serum, lung homogenates and bronchoalveolar lavage fluid (BALF), total protein levels in BALF, mRNA expressions of selected cytokines in lung tissue, and lung injury histopathology scores were determined. Results: Animals remained hemodynamically stable throughout the entire experiment. After eight hours of MV, compared to the CV Group, the SB Group had lower PaCO2 values and ratios of dead space to tidal volume, and higher lung compliance. -

Prevention of Ventilator Associated Complications
Prevention of Ventilator associated complications Authors: Dr Aparna Chandrasekaran* & Dr Ashok Deorari From: Department of Pediatrics , WHO CC AIIMS , New Delhi-110029 & * Neonatologist , Childs Trust Medical Research Foundation and Kanchi Kamakoti Childs Trust Hospital, Chennai -600034. Word count Text: 4890 (excluding tables and references) Figures: 1; Panels: 2 Key words: Ventilator associated complications, bronchopulmonary dysplasia Abbreviations: VAP- Ventilator associated pneumonia , BPD- Bronchopulmonary dysplasia, ELBW- Extremely low birth weight, VLBW- Very low birth weight, ROP- Retinopathy of prematurity, CPAP- Continuous positive airway pressure, I.M.- intramuscular, CI- Confidence intervals, PPROM- Preterm prelabour rupture of membranes, RCT- Randomised control trial, RR- Relative risk, PEEP- Peak end expiratory pressure Background: The last two decades have witnessed a dramatic reduction in neonatal mortality from 4.4 million newborn deaths annually in 1990 to 2.9 million deaths yearly in the year 2012, a reduction by 35%. In India, neonatal mortality has decreased by 42% during the same period. (1) With the increasing survival and therapeutic advances, the new paradigm is now on providing best quality of care and preventing complications related to therapy. Assisted ventilation dates back to 1879, when the Aerophone Pulmonaire, the world’s earliest ventilator was developed. This was essentially a simple tube connected to a rubber bulb. The tube was placed in the infant’s airway and the bulb was alternately compressed and released to produce inspiration and expiration. (2) With better understanding of pulmonary physiology and mechanics , lung protective strategies have evolved in the last two decades, with new resuscitation devices that limit pressure (T-piece resuscitator), non-invasive ventilation, microprocessors that allow synchronised breaths and regulate volume and high frequency oscillators/ jet ventilators. -

Biomarkers of Acute Lung Injury: Worth Their Salt? Alastair G Proudfoot1,2†, Matthew Hind1,2† and Mark JD Griffiths1,2*†
Proudfoot et al. BMC Medicine 2011, 9:132 http://www.biomedcentral.com/1741-7015/9/132 Clinical Biomarkers OPINION Open Access Biomarkers of acute lung injury: worth their salt? Alastair G Proudfoot1,2†, Matthew Hind1,2† and Mark JD Griffiths1,2*† Abstract The validation of biomarkers has become a key goal of translational biomedical research. The purpose of this article is to discuss the role of biomarkers in the management of acute lung injury (ALI) and related research. Biomarkers should be sensitive and specific indicators of clinically important processes and should change in a relevant timeframe to affect recruitment to trials or clinical management. We do not believe that they necessarily need to reflect pathogenic processes. We critically examined current strategies used to identify biomarkers and which, owing to expedience, have been dominated by reanalysis of blood derived markers from large multicenter Phase 3 studies. Combining new and existing validated biomarkers with physiological and other data may add predictive power and facilitate the development of important aids to research and therapy. Introduction The natural history of acute lung injury Thesyndromeacutelunginjury(ALI)anditsmore Regardless of the wide variety of insults that cause or severe counterpart acute respiratory distress syndrome contribute to the development of ALI, the response of (ARDS) are defined by radiographic and physiological the lung is largely stereotypic. A combination of tissue changes that characterize patients with acute lung fail- injury and inflammation affecting the gas exchange sur- ure (Table 1) [1]. All age groups may be affected, face of the lung, the alveolar-capillary membrane, causes although the syndrome has a higher incidence and mor- high permeability pulmonary edema. -

Date 10/15/2018 Page 1 of 12 Protocol Version-I
Feasibility and Impact of Volume Targeted Ventilation for preterm infants born < 32 weeks gestational age with need for invasive Positive Pressure Ventilation in the Delivery Room in reducing neonatal pulmonary morbidities Phase I: Feasibility of Measuring Tidal Volume in the Delivery Room Phase II: Feasibility of providing Volume Targeted Ventilation in the Delivery Room Primary Investigator: Ruben Vaidya, MD Co-Investigators: Paul Visintainer, PhD, Rachana Singh, MD Research Coordinator: TBD Address: Division of Newborn Medicine Department of Pediatrics UMMS-Baystate, Springfield, MA 01199 Phone: 413-794-2400 Email: [email protected] Date 10/15/2018 Page 1 of 12 Protocol Version-I SPECIFIC AIMS AND HYPOTHESIS Bronchopulmonary dysplasia (BPD) continues to be one of the most common long-term pulmonary complications associated with preterm birth. Despite significant decreases in preterm mortality, BPD rates in infants born < 28 weeks gestational age have remained unchanged at approximately 40% i ii iii. This probably is due to the multifactorial pathogenesis of BPD, with lung injury to the immature pulmonary tissue secondary to exposures including but not limited to antenatal/postnatal infection, free oxygen radical toxicity, and/or mechanical ventilation all leading to lung inflammation. Delivery room (DR) practices of preterm infant during initial resuscitation can have a significant impact on occurrence and severity BPD. Current delivery room resuscitation for intubated preterm infants focuses on pressure limited ventilation (PLV), however, rapidly changing pulmonary compliance during the early newborn transition phase results in significant variability in the tidal volume provided to the infant, which in turn can lead to volutrauma, barotrauma and/or atelactetotrauma. -

Respiratory Oscillations in Alveolar Oxygen Tension Measured in Arterial
www.nature.com/scientificreports OPEN Respiratory oscillations in alveolar oxygen tension measured in arterial blood Received: 13 February 2017 Federico Formenti 1,2, Nikhil Bommakanti1, Rongsheng Chen1, John N. Cronin 2, Hanne Accepted: 20 June 2017 McPeak1, Delphine Holopherne-Doran3, Goran Hedenstierna 4, Clive E. W. Hahn1, Anders Published: xx xx xxxx Larsson5 & Andrew D. Farmery1 Arterial oxygen partial pressure can increase during inspiration and decrease during expiration in the presence of a variable shunt fraction, such as with cyclical atelectasis, but it is generally presumed to remain constant within a respiratory cycle in the healthy lung. We measured arterial oxygen partial pressure continuously with a fast intra-vascular sensor in the carotid artery of anaesthetized, mechanically ventilated pigs, without lung injury. Here we demonstrate that arterial oxygen partial pressure shows respiratory oscillations in the uninjured pig lung, in the absence of cyclical atelectasis (as determined with dynamic computed tomography), with oscillation amplitudes that exceeded 50 mmHg, depending on the conditions of mechanical ventilation. These arterial oxygen partial pressure respiratory oscillations can be modelled from a single alveolar compartment and a constant oxygen uptake, without the requirement for an increased shunt fraction during expiration. Our results are likely to contribute to the interpretation of arterial oxygen respiratory oscillations observed during mechanical ventilation in the acute respiratory distress syndrome. In the healthy lung, arterial partial pressure of oxygen (PaO2) is thought to remain almost constant within the respiratory cycle during spontaneous breathing, via a physiological PO2 gradient between the alveoli and the pul- 1 monary circulation . Respiratory PaO2 oscillations smaller than 16 mmHg have been detected with slow response 2 −1 time sensors in animals with uninjured lungs when abnormally large tidal volumes (VT) greater than 20 ml kg or even 30 ml kg−1 were delivered during mechanical ventilation3, 4. -

“Post” COVID-19 Lungs in the Operating Room
“Post” COVID-19 Lungs in the Operating Room Kalina Nedeff, M.D., Austin Smith, D.O., Catalina Carvajal, D.O., Laszlo Balazs M.D. Introduction Results Discussion • 58 year-old male recently diagnosed with COVID-19 presented with • Patient later developed intermittent atrial fibrillation with rapid ventricular • Coronavirus (COVID-19) is an infectious disease caused by a newly worsening shortness of breath. response intermixed with bradycardia discovered strain that mainly affects the upper respiratory system • Pulse oximetry revealed 86% SpO2 on room air with improvement to 94% • Patient necessitated additional vasopressor support as well as blood • The virus is primarily spread through respiratory droplets SpO2 on 3L of oxygen via nasal cannula. products to maintain hemodynamics • Patients affected with COVID that end up on mechanical ventilation may • Patient was treated with remdesivir, ceftriaxone, azithromycin, steroids, • Copious bloody secretions were suctioned from the tracheostomy develop COVID Pneumonia which progresses to acute respiratory vitamins and anticoagulation. • Family ultimately decided to implement comfort measures distress syndrome (ARDS). • New-onset atrial fibrillation was discovered, with hypotension which • The lungs become inflamed and fill with fluid, making oxygen diffusion in required vasopressor support and declining respiratory status prompting capillaries difficult. endotracheal intubation with mechanical ventilation. • For mechanically ventilated adults with COVID-19 and ARDS, lung • Patient continued -

Mechanical Ventilation Guidelines
Newborn Critical Care Center (NCCC) Clinical Guidelines Conventional Mechanical Ventilation (CMV) BACKGROUND Mechanical ventilation is not a cure to underlying illness, but instead can be a lifesaving therapy which supports infants with respiratory failure while the underlying disease process resolves. Conventional mechanical ventilation and high frequency ventilation (HFV) are invasive therapies available for management of respiratory failure, while continuous positive airway pressure (CPAP), high flow and low flow nasal cannula and oxyhood are examples of noninvasive therapies available for management of respiratory distress. Clinicians should provide infants with the appropriate level of respiratory support to ensure optimal oxygenation and ventilation while simultaneously minimizing injury. Providing infants with inadequate respiratory support may result in morbidity due to hypoxemia, hypercarbia and/or atelectotrauma, while providing infants with extraneous respiratory support may result in morbidity due to hyperoxia, hypocarbia, barotrauma and/or volutrauma. INDICATIONS Respiratory failure secondary to severe respiratory acidosis, hypoxemia or apnea Anticipated respiratory failure, such as immediately prior to a surgical procedure or with significant cardiovascular compromise Severe metabolic acidosis with concern for impending respiratory failure PHYSIOLOGY Ventilation (CO2): o Minute ventilation is the product of respiratory rate (RR) and tidal volume (Vt) 푉̇ = 푅푅 푥 푉푇 o Ventilation is, therefore, increased by increasing the RR or Vt. Oxygenation (O2): o Is dependent on the fraction of inspired oxygen (FiO2) and the recruitment of lung tissue to participate in gas exchange, which is dependent on mean airway pressure (MAP) o Oxygenation is increased by increasing the MAP within limits imposed by lung mechanics and by increasing the FiO2. The MAP is most effectively increased by increasing PEEP, but may also be increased by increasing the inspiratory time (Ti) and peak inspiratory pressure (PIP), if in a pressure mode. -

Tidal Volume Settings in Adult Mechanical Ventilation
Setting the Tidal Volume In Adults Receiving Mechanical Ventilation: Lessons Learned From Recent Investigations Todd Bocklage, MPA, RRT Assistant Manager – Respiratory Care Services & Pulmonary Function Lab University of Missouri Health Care University Hospital & Women’s and Children’s Hospital Columbia, Missouri Robert A. Balk, MD J. Bailey Carter, MD Professor of Medicine Director – Division of Pulmonary and Critical Care Medicine Rush Medical College and Rush University Medical Center Chicago, IL Corresponding Author: Robert A. Balk, MD Division of Pulmonary and Critical Care Medicine Rush University Medical Center 1725 W. Harrison, Suite 054 Chicago, IL 60612 T 312-942-2552 F 312-942-8187 Email [email protected] Disclosure: Both authors are members of the National Board of Respiratory Care. Neither author has other real or potential conflicts of interest or other disclosures to declare. Introduction Selecting the optimum tidal volume for adult patients on ventilatory support is critical to achieving the best clinical outcomes. Over the years, guidelines about tidal volumes have varied including times when sigh breaths were set to prevent the development of atelectasis. The purpose of this article is to describe the transition that examination committees have made over the last several years in which lung protection has become the primary goal when making decisions about mechanical ventilation. Ventilator Induced Lung Injury Since the introduction of mechanical ventilatory support over 60 years ago, there has been an increasing body of -
What Is Optimal Paw Strategy 2015 Handout.Pptx
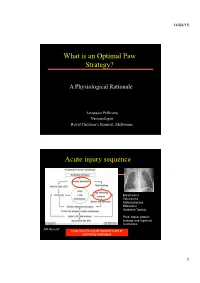
14/04/15 What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children’s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative Toxicity Fluid, blood, protein leakage and impaired mechanics NN Rocourt Lung injury is a multi-factorial event of conflicting aetiologies 1 14/04/15 Respiratory failure Mechanical ventilation Lung protective ventilaton Ventilator-induced lung injury - Oedema - Inflammation - Surfactant inhibition Lung Protective Strategies • Lung Protective Mechanical Ventilation Strategies aim to: • Achieve optimal gas exchange – Recruit collapsed alveoli uniformly – Minimise the known causes of VILI: - Atelectasis - Volutrauma - Sheer-force stresses - Oxidative Injury - Rheotrauma 2 14/04/15 Small VT, PEEP and LPV Extravascular lung I125 albumin (%) water (ml/kg) 9 80 8 70 7 60 6 50 5 40 4 30 3 20 2 1 10 0 0 HiP-HiV LoP-HiV HiP-LoV HiP-HiV LoP-HiVHiP-LoV & Dreyfuss D et al. Am Rev Resp Dis, 1985 Optimal ventilation strategy - systematic review 18 trials (n=3229 infants) • Subgroup analysis revealed it was more important how ventilation was delivered, rather than modality of ventilation: – Low lung volume strategies: worse outcomes – High lung volume strategies: small but significant reduction in death or CLD & Cools et al Lancet 2010 HFOV Workshop 21st – 22nd July 2011 3 14/04/15 Effect of a single sustained inflation on lung volume and oxygenation during HFOV Kolton et al Hamilton et al 1983 • During HFOV, a static • During ventilation, a static inflation (SI) improved inflation improved lung volume oxygenation in HFOV group Key: a- disconnection b- PEEP c- HFOV d- static inflation e- HFOV at initial Volume Paw Time & Anesth Analg 1982 & J Appl Physiol 1983 High Lung Volume and Oxygenation 480 400 320 HFO-A/HI 240 HFO-A/LO (mmHg) 2 160 PaO 80 H PL PSI 1 2 3 4 5 6 7 Time (hours) & McCulloch et al. -

Mechanical Ventilation – Educational Reinforcement Material
Educational Reinforcement Material Critical Care Fundamentals: Mechanical Ventilation Table of Contents Pre-Test Questions ………………………………..……………………………………………… Page 3 Manual (blanks) ……,………,……………………………………………………………………. Page 11 Reinforcement Game …………………………………….……………………………………… Page 17 Post- Test Questions ……………………………………………………………………………. Page 18 Pre-Test Questions with answers ……………………………………………………………… Page 25 Post- Test Questions with answers ……………………………………………………………. Page 33 2 Critical Care Fundamentals: Mechanical Ventilation Pre-Test Questions 1. Which of the following is not the main goal of mechanical ventilation in the ICU? a. Optimize patient comfort b. Optimize exchange of carbon dioxide and oxygen c. Get them through surgery with less discomfort d. Decrease work of breathing 2. What are ways to maximize patient comfort on the ventilator? a. Optimize ventilation settings b. Sedation c. Paralytics d. All of the above 3. What is the optimal type of breath? a. Spontaneous b. Controlled c. Assisted d. None of the above 4. Will all patients have perfect carbon dioxide and oxygen levels? a. Yes b. No 5. What should the carbon dioxide goal be with traumatic brain injury? a. High to allow increased cerebral blood flow b. High to prevent increased cerebral blood flow c. Normal to prevent increased cerebral blood flow d. Normal to allow increased cerebral blood flow 6. Which of the following is not a toxicity with mechanical intubation? a. Hypercarbia b. Barotrauma c. Volutrauma d. Atelactotrauma e. Oxygen toxicity 7. What percent of oxygen can lead to oxygen toxicity (even if only a short period of time)? a. >50 % b. >60% c. >70% d. >80% 8. What is the volume of gas in the lungs at the end of expiration, but prior to inhalation? a. -

Should Our Patients with ALI Or ARDS Be Ventilated at Higher PEEP Levels?
netherlands journal of critical care Copyright ©2008, Nederlandse Vereniging voor Intensive Care. All Rights Reserved. Received July 2008 ; Accepted July 2008 e d i t o r i a l Should our patients with ALI or ARDS be ventilated at higher PEEP levels? D Gommers Department of Intensive Care, Erasmus Medical Center, Rotterdam, The Netherlands In patients with the acute respiratory syndrome (ARDS), the lung is maximum plateau pressure to above 30 cm H2O [5]. In the ExPress atelectatic or consolidated, particularly in dependent regions, so that trial, no recruitment manoeuvres were performed. For both studies, it cannot participate in gas exchange. During mechanical ventilation, the primary outcome was the effect on mortality in comparison with the less affected lung regions must therefore accommodate most of the the established low-tidal volume strategy from ARDS network trials. tidal volume, with the risk of tidal hyperinflation. The ARDS network In both studies, the 28-day mortality rate was 28% in the trial established the importance of hyperinflation by demonstrating intervention group and 32% in the controls, but this difference that ventilation using lower tidal volumes (6 versus 12 mL/kg) and was not significant [4,5]. The intervention group appeared to have maintaining a plateau pressure of no more than 30 cm H2O, improves improved secondary endpoints in both trials, such as oxygenation survival [1]. In a second trial of the ARDS network group, the ALVEOLI and less use of rescue therapies. Moreover, the recruitment ventilation trial, it was shown that application of higher positive end-expiratory strategy in the ExPress trial resulted in more ventilator-free days and pressure (PEEP) levels improved oxygenation but did not have an organ failure-free days [5]. -

Clinical Research Protocol
Study Title: A randomized controlled trial of respiratory function monitoring during stabilization of preterm infants at birth Short Title: MONITOR Trial NCT Number: NCT03256578 Document IRB Approval Date: February 14, 2019 MONITOR TRIAL (Monitoring Neonatal Resuscitation Trial) A multi-center randomized controlled trial of respiratory function monitoring during stabilization of preterm infants at birth Local Principal Investigator (1) Elizabeth Foglia MD MSCE1 Division of Neonatology 3400 Spruce St. Ravdin 8 215-662-3228 [email protected] Coordinating Site Principal Investigator (2) Arjan te Pas2 C.Omar Kamlin3 Prof Maximo Vento4 Gianluca Lista5 Kajsa Bohlin7 Co-Investigators (3) Henriette van Zanten2 Prof Colin Morley3 Enrico Lopriore2 Prof Peter G Davis3 Marta Thio3 Charles Christopher Röhr2 Marta Aguar4 Francesco Cavigioli5 Erik van Zwet6 1. Hospital of the University of Pennsylvania, Philadelphia, United States 2. Leiden University Medical Center, Leiden, the Netherlands 3. Department of Newborn Research, Royal Women’s Hospital, Melbourne, Australia 4. Maternal & Children’s University Hospital La Fe, Valencia, Spain 5. Neonatal Intensive Care Unit, V.Buzzi Children's Hospital, Milan, Italy 6. Department of Medical Statistics, Leiden University Medical Center, Leiden, the Netherlands 7. Karolinska University Hospital Huddinge, Stockholm, Sweden Protocol Version: UPenn MONITOR Protocol Version 3.0 February 5, 2019 IRB Number: 826695 Coordinating Site Protocol Version: Protocol 12.295 v5 December 8, 2017 Netherlands Trial Registry: