Annamalai University Department of Economics (Ugc-Sap-Drs I)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Calendar-2017-2018.Pdf
3 PRAYER FOR THE COLLEGE O Thou, who in days past didst put it into the hearts of good men to found this College; for the imparting of sound learning, the building of character and the spread of spiritual truth and knowledge of Thyself. Bless our College and Schools; may love, unity and brotherhood be learnt here; may industry, uprightness and courage grow here; and from this place may there be sent forth continually a stream of men and women who shall serve Thee faithfully in Thy world. Amen. PRAYER FOR THE ALUMNI O God, of whose gift alone it cometh that Thy faithful people do unto Thee true and faithful service. We pray Thee to follow with Thy blessing those students who have gone out from amongst us to serve in the wider arena of life outside these College walls. Strengthen them to meet victoriously all temptations, enable them for the faithful performance of their life-work and may they ever without fear of man follow steadfastly where duty, right and honour lead. Amen. 4 A BRIEF HISTORY OF MADRAS CHRISTIAN COLLEGE Madras Christian College traces its origin to the General Assembly School founded by the Rev. John Anderson, a Missionary from the Church of Scotland on 3rd April 1837. Anderson was a pioneer in introducing English medium education in South India. He was ably assisted by Rev. Johnston, Rev. Braidwood and Margaret Locher Anderson. Rev. William Miller who arrived in 1862 upgraded the school to a college by adding F.A. and B.A., courses in 1865 and 1867. -

Curriculum Vitae
Dr. N. SETHURAMAN Head i/c, P.G. Department of Social Work, Assistant Professor, Post Graduate and Research Department of History, Periyar Arts College, Cuddalore – 607 001, Tamil Nadu, India. Member, IQAC Coordinator, Nehru Youth Club Editorial Board Member, Tamil Nadu History Congress Proceedings Mobile: 9865381281, 9442428826 Landline: 04142-223281 (Res.) Email: [email protected] [email protected] https://www.youtube.com/c/HISTORIANSETHURAMAN Dr. N. Sethuraman is working as Assistant Professor of History in the Post Graduate and Research Department of History of Periyar Arts College in Cuddalore since 2009. He is also the Head in-charge of the P.G. Department of Social Work. Previously, as Guest Lecturer, he has taught in the Department of History, Bharathidasan University, Tiruchirappalli. He has studied B.A. History in Bishop Heber College, Tiruchirappalli and completed M.A. in History in the Department of History, Bharathidasan University, Tiruchirappalli. He did his Ph.D. on “Indo-U.S. Relations: Strategic Importance and Security Issues” from Bharathidasan University, Tiruchirappalli under the guidance of Professor N. Rajendran, who is at present the Vice-Chancellor of Alagappa University, Karaikudi. Dr. N. Sethuraman is a research supervisor in History and at present, guiding four research scholars. He has authored two books and edited one book and published many numbers of research articles in journals, edited books, and conference proceedings. He is also serving as the Editorial Board Member of the Tamil Nadu History Congress Proceedings since 2013. He has organised many national seminars, workshops, conferences and lectures. He is a member of U.G. and P.G. -
Bharathiar University, Coimbatore - 641 046 Part - Time Ph.D
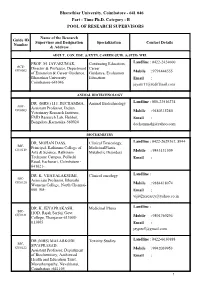
Bharathiar University, Coimbatore - 641 046 Part - Time Ph.D. Category - B POOL OF RESEARCH SUPERVISORS Name of the Research Guide ID Supervisor and Designation Specialization Contact Details Number & Address ADULT . CON. EDU. & EXTN. CAREER GUID. & STUD. WEL PROF. M. JAYAKUMAR, Continuing Education, Landline : 0422-2424600 ACE- Director & Professor, Department Career GU0002 of Extension & Career Guidance, Guidance, Evaluation Mobile : 9791444555 Bharathiar University Education Email : Coimbatore-641046 [email protected] ANIMAL BIOTECHNOLOGY DR. (MRS.) H.J. DECHAMMA, Animal Biotechnology Landline : 080-23516274 ABT- Assistant Professor, Indian GU0003 Veterinary Research Institute, Mobile : 9480315280 FMD Research Lab, Hebbal, Email : Bangalore,Karnataka-560024 [email protected] BIOCHEMISTRY DR. MOHAN DASS, Clinical Toxicology, Landline : 0422-2629367, 8944 BIC- Principal, Rathinam College of MedicinalPlants, GU0119 Arts & Science, Rathinam Metabolic Disorders Mobile : 9843131509 Techzone Campus, Pollachi Email : Road, Eachanari, Coimbatore - 641021- DR. K. VIJAYALAKSHMI, Clinical oncology Landline : BIC- Associate Professor, Bharathi GU0120 Womens College, North Chennai- Mobile : 9884418074 600 108- Email : [email protected] DR. K. JEYAPRAKASH, Medicinal Plants Landline : BIC- HOD, Rajah Serfoji Govt. GU0121 College, Thanjavur-613005- Mobile : 9894769294 613005 Email : [email protected] DR.(MRS) MALARKODI Toxicity Studies Landline : 0422-6630888 BIC- SIVAPRASAD, GU0122 Assistant Professor, Department Mobile : 9942039953 of Biochemistry, Aashirwad Email : Health and Education Trust, Mavuthampathy, Navakkarai, Coimbatore -641105 1 DR. P. SUMATHI, Clinical Bio-Chemistry Landline : 044-27454863 BIC- Assistant Professor, Govt. GU0123 College for Women, Krishnagiri- Mobile : 9444151677 635001 Email : DR. M. JEYARAJ, Plant Bio-Chemistry Landline : BIC- Lecturer, Dept. of Biochemistry, GU0124 Government of Arts College, Mobile : 9787059193 Paramakudi , Ramnad Dt., Email : Tamilnadu-623707 [email protected] [email protected] DR. -

Details of Programmes Organized by Tnteu Teaching
DETAILS OF PROGRAMMES ORGANIZED BY TNTEU TEACHING FACULTY AND TNTEU TEACHING FACULTY AS RESOURCE PERSON Sl. No. Date of the No. of Topic / Title of the Organized by Programme Days Webinar/Seminar/Video/ Programme including Resource Person 1. 18/12/2017 4 Benchmark Training Course Tamil Nadu Teachers Education to for Administrative Officers and University & Ministry of Education, 21/12/2017 Teachers, Ministry of Malaysia. Education, Malaysia 2. 07/12/2017 1 Inauguration of Youth Red Dr. P. C. NagaSubramani, Cross (YRC) in TNTEU AssociateProfessor, Department of Pedagogical Sciences,TNTEU. 3. 11/01/2018 1 One Day Awareness Youth Red Cross Programme on “Health Dr. P. C. NagaSubramani, Awareness and Screening AssociateProfessor, Department Camp” of Pedagogical Sciences,TNTEU. 4. 23/01/2018 3 Three Days Workshop on Department of Educational to “Revisiting the TNTEU B.Ed. Planning and Administration, 25/01/2018 Practical Components” at TNTEU. Tamil Nadu Teachers Education University. 5. 04/04/2018 2 Workshop on “Development of Department of Value Education, to Positive Thinking” TNTEU. 05/04/2018 6. 18/04/2018 2 National Colloquium on Department of Educational to “Mechanics of Thesis Writing” Planning and Administration, 19/04/2018 TNTEU. 7. 24/04/2018 2 Workshop on “Tamil Department of Curriculum to Computing” Planning and Evaluation, 25/04/2018 TNTEU. 8. 26/04/2018 2 Workshop on “Statistical Department of Pedagogical to Package for the Social Sciences, TNTEU. 27/04/2018 Sciences (SPSS)” 9. 08/05/2018 1 One Day Blood Donation Youth Red Cross Camp Dr. P. C. NagaSubramani, AssociateProfessor, Department of Pedagogical Sciences, TNTEU. -

Department of Microbiology Profile
BHARATHIDASAN UNIVERSITY Tiruchirappalli – 620 024, Tamil Nadu, India DEPARTMENT OF MICROBIOLOGY PROFILE 2 National Recognitions UGC Non-SAP DST FIST (Leve-lI) DST-PURSE MHRD RUSA National Repository for Microalgae & Cyanobacteria – Freshwater (Sponsored by DBT, Govt. of India) 3 FACULTY MEMBERS Dr. N. Thajuddin Professor and Head Dr. K. Natarajaseenivasan Professor Dr. V. Rajesh Kannan Associate Professor Dr. D. Dhanasekaran Assistant Professor Dr. G. Muralitharan Assistant Professor Dr. P. Thiyagarajan Assistant Professor Dr. C. Nithya DST-INSPIRE Faculty 4 Department of Microbiology PREFACE This brochure is intended to provide an insight into the Department of Microbiology, Bharathidasan University for the benefit of prospective students, alumni, industries and the public. We hope this would convey the versatile dynamism and the infective enthusiasm of the young and active Microbiology Department. As a result of emphasis on research that erases the traditional academic boundaries, we collaborate closely with other departments of Bharathidasan University as well as other universities, institutions and industries within and outside the country. The department is reverberating with active research in both basic and applied aspects of microbiology encompassing wide areas such as biodiversity; ecobiology; & molecular taxonomy including DNA fingerprinting of bacteria, cyanobacteria, fungi, actinomycetes and microalgae; establishment of microbial repository; development of pharmaceuticals, nutraceuticals and bioenergy from various microbes. We work also on microbial nanoparticles; leptospirosis; molecular diagnostics; metagenomics; probiotics; marine bacterial endosymbionts and rhizosphere biology. The department is unique in having a host of faculty trained in advanced areas of research in different countries around the world. They are now engaged in developing the required manpower on modern microbiology, molecular biology and biotechnology in this country. -

Curriculum Vitae
CURRICULUM VITAE Name : Dr. M. SENAPATHY Sex : Male Nationality : Indian Permanent Address : 9, Veera Kovil Street, Kalvi Nagar, Rajambadi (PO), Madurai - 625 021, Tamil Nadu, India Contact Phone & E-mail : +251 982053540 (Ethiopia Mobile) & [email protected] Envision an academic world where the new knowledge thrives and sustain for global VISION development. The scientific mission is to make more productive, resilient and authentic research on MISSION development of the academic community as well as the societal improvement. ACADEMIC QUALIFICATIONS Examination passed Name of the Institution / Year of % of Marks & with Subjects University Passing Ranks B.Sc. (Rural P.M.Thevar College, Usilampatti, Development Science) 66% Madurai District. Madurai Kamaraj 1983-86 Specialization: University II Rank University AGRICULTURE M.Sc.(Rural Arul Anandar College, Karumathur, Development Science) 74 % Madurai District. Madurai Kamaraj 1986-88 Specialization: University II Rank University AGRICULTURE M.A. Sociology Madurai Kamaraj University 2000 57% Dept. of Rural Development, M.Phil. in Micro-Level Gandhigram Rural University, 1988-89 66% Planning (M.L.P.) Tamilnadu, India Dept. of Rural Development Ph.D. in Rural Thesis Gandhigram Rural University, 2005 Development Awarded Tamilnadu, India 1 TECHNICAL QUALIFICATIONS Subjects Institution Year of Passing and % Dept. of Technical Education, Type Writing English Lower May 1982 Chennai Post Graduate Diploma in Madurai Kamaraj May 1991 Computer Application (P.G.D.C.A) University, Tamil Nadu, India Bachelor of Library & Information Madurai Kamaraj University, May 1993 and 68% Science (B.L.I.Sc.) Tamil Nadu, India Master of Library & Information Madurai Kamaraj University, May 1994 and 64% Science (M.L.I.Sc.) Tamil Nadu, India Ph.D. -

Curriculum Vitae
Curriculum Vitae 1. Name : Dr.V.S.Gowri 2. Designation : Technical Assistant (Special Grade) 3. Educational Qualification : M.Sc, M.Phil, Ph.D PG Diploma (Bioinformatics) 4. Research / Teaching Experience : 20 years 5. Travel or Study abroad : U.K. in 1999 (Univ. of NewCastle upon Tyne) Germany in 2002 (Centre for Tropical Marine Ecology, Bremen) EXPERIENCE IN RESEARCH AND TRAINING DATE DEGREE & INSTITUTION SUBJECT ________________________________________________________________________ 1986 to Ph.D., Institute for Ocean Management Coastal Marine Pollution continuing Anna University Remote sensing and GIS Chennai - 600 025. Data Base Management Water Quality Studies Instrumentation 1980-1981 M.Phil, Dept. of Zoology Parasitology, Pathobiology Madras University Marine Biology, Reproductive Biology Neurobiology, Research Methodologies 1978-1980 M.Sc, Madras University Invertebrate & Chordate Madras Christian College Phylogenies, Genetics, East Tambaram, Madras University Embryology, Ecology Madras - 600 052. Entomology 1975-1978 B.Sc, Madras University Zoology, Botany and Madras - 600 052. Chemistry ________________________________________________________________________ AWARDS DATE VENUE PURPOSE June 1999 University of Newcastle Three weeks training - “Train the upon Tyne, UK Trainers in Coastal Zone Management” November 2002 Bremen, Germany One week training – “Training / Education / Research in the field of management of coastal and marine resources ________________________________________________________________________ PUBLICATIONS (IN BOOK): 1. Krishnamoorthy, R., S.Sundaramoorthy, D.Mohan, V.S.Gowri and S.Ramachandran. 1994. Status of Mangroves along Tamilnadu coast and their spectral properties - A remote sensing Approach. In: Remote Sensing and Geographical Information Systems for Environmental Planning . I.V.MuraliKrishna (Ed). Tata McGraw-Hill Publishing Company Ltd. New Delhi. 397-409 pp. 2. Gowri,V.S. and S.Ramachandran. 2001. Coastal Pollution Management. In: Coastal Environment and Management. -

Annual Day Report 2016 – 2017
COLLEGE DAY REPORT 2016- 17 25/03/17 BIDECENNIAL CELEBRATIONS: 20 YEARS OF EXCELLENCE IN EDUCATION : Kumararani Meena Muthiah College of Arts and Science celebrated 20 years of success in the field of education on September 1st at Kamaraj Arangam. Dr.(Mrs). Meena Muthiah, Secretary and Correspondent, Kumararani of Chettinad, presided over the function. Guests of Honour included Dr. G. Viswanathan, Chancellor, VIT, Col. Dr. G. Thiruvasagam, Vice Chancellor, AMET University, Dr. Preetha Reddy, Executive Vice Chairperson, Apollo Hospitals Enterprise Ltd., and Dr. P. David Jawahar, Registrar, University of Madras. A Centre for Business Excellence was officially launched and installed by Dr.Mrs.Meena Muthiah, Secretary and Correspondent of the college. The Centre for Business Excellence is a knowledge hub and has partnered with South Indian bank and has established a simulated bank inside the college premises. It provides practical exposure to students to acquire knowledge in Business and managerial skills. The centre has also collaborated with Finmark to provide practical exposure in capital market sector. The capital market sector in the centre for business excellence provides practical exposure to students to trade in stock exchange ACADEMICS: The following students secured centum in the university papers. ✓ S.Lathik Lekha Bcom(A&F) Secured Centum In ✓ K.Prabhakaran, T.Venkatesan, M.Deepika , J.Ramya , S.Sangeetha, K. Thilagavathy & D.Thulsi Kharel B.Com (C.S) Secured 100% In Institutionaltraining: ✓ Sriram M.ScIT Secured Centum In Project. ✓ P. Gowtham Raj, K. Jagathratchagan, N.Karthik, Roshan Choudry,S. Santhosh Kumar, Johra Jabeen, K. Keerthana, M. Anupriya,C. Srivignesh,K. Megala,R. Mohanapriya ,N.Priyadharshini,M.Vinitha,Vellala Sumithra of BBA Secured Centum In Project. -
Nehru Arts and Science College, Coimbatore • R.V.S
• Nehru Arts and Science College, Coimbatore • R.V.S. College of Arts and Science, Coimbatore • C.B.M. College Sakethapuri, Coimbatore • Chikkanna Government Arts College, Coimbatore • Emerald Heights College for Women, Udhagamandalam • Govt. Arts College (Autonomous), Coimbatore • Govt. Arts College, Udagamandalam • Govt. Arts College, Udumalpet • Kongunadu Arts and Science College, Coimbatore • L.R.G. Govt. Arts College for Women, Tiruppur • Nallamuthu Gounder Mahalingam College (Autonomous), Pollachi • Nirmala College for Women, Coimbatore • P.S.G. College of Arts and Science (Autonomous), Coimbatore • P.S.G.R. Krishnamal College for Women, Coimbatore • Providence College for Women, Udhagamandalam • Sri G.V.G. Visalakshi College for Women (Autonomous), Udumalpet • Sri Ramakrishna Mission Vidyalaya College of Arts and Science (Autonomous), Coimbatore • Thavathiru Santhalinga Adigallar Arts and Science, Coimbatore • A.J.K. College of Arts and Science, Coimbatore • Angappa College of Arts and Science, Coimbatore • Avinashilingam University for Women (Avinashilingam Institute for Home Science and Higher Education for Women), Coimbatore • Bishop Ambrose College, Coimbatore • C.M.S. College of Science and Commerce, Coimbatore • C.S.I. Bishop Appasamy College of Arts and Science, Coimbatore • Cherran College For Women, Tirupur • Dr. G.R. Damodaran College of Science, Coimbatore • Dr. N.G.P. Arts and Science College, Coimbatore • Dr. R.V. Arts and Science College, Coimbatore • Dr. S.N.S. Rajalakshmi College of Arts and Science, Coimbatore • -
1 Name of the Department 2 Year Of
NAAC Reaccreditation - Evaluative Report School of Life Sciences Department of Zoology 1 Name of the Department Department of Zoology 2 Year of establishment 1927 3 Is the Department part of a YES, School of Life Sciences School/Faculty of the university? 4 Names of programmes offered (UG, M.Sc. (Zoology) PG, M.Phil., Ph.D., Integrated M. Phil. (Zoololgy) Masters; Integrated Ph.D., D.Sc., Ph.D. D.Litt., etc.) Diploma: 1. P.G. Dip. in Immunotechnology 2. P.G. Dip. in Stem Cell Technology and Tissue Engineering 5 Interdisciplinary programmes and a) UGC-UPE Programme involving departments involved Departments of Life Sciences and Basic Medical Sciences b) UGC-CPEPA Programme involving School of Life Sciences 6 Courses in collaboration with other a) Post Graduate Diploma in universities, industries, foreign Immunotechnology in collaboration institutions, etc. with M/S Mediclone Biotech Pvt. Ltd., Chennai. b) Post Graduate Diploma in Stem Cell Biology and Tissue Engineering in collaboration with Frontier Lifeline Hospitals, Chennai. 7 Details of programmes discontinued, M.Sc. Ocean Science and Technology – if any, with reasons 2009 8 Examination System: Annual/ Choice Based Credit System Semester/ Trimester/Choice Based Credit System 9 Participation of the department in a) Microbiology offered by CAS in the courses offered by other Botany, University of Madras, departments Guindy, Chennai – 600 025. 1 NAAC Reaccreditation - Evaluative Report School of Life Sciences Department of Zoology b) Genetics offered by Department of Genetics, University of Madras, Taramani Campus, Chennai – 600 113. c) Biostatistics offered by Department of Statistics, University of Madras, Chepauk, Chennai -600 005. 10. Number of teaching posts sanctioned, filled and actual (Professors/Associate Professors/Asst. -

Visiting Faculty
STELLA MARIS COLLEGE (Autonomous), Chennai Postgraduate Certificate in International Business VISITING FACULTY Professor of Finance and the Chairperson of Ph. D. Programme at LIBA, Chennai Prof. Anthuvan is the Research Director at LIBA. He has over 40 years of experience in teaching and reserch and has held senior positions in various academic capacities. He has published over 70 research papers in several national and international journals and delivered keynote addresses at more than 100 conferences and seminars. He has also published books focusing on issues pertaining to globalization and Global Finance. He has guided many Ph.D. scholars, who received their degrees from the Bharathidasan University and the University of Madras. Prof. Anthuvan teaches Finance verticals at LIBA. He has been addressing teachers &students of StockHolm University, Sweden for many years. He has coordinated a research project on ‘Industrial Clusters’, in collaboration with Sacro Cuore Catholic University of Milan, Milan, Italy. He was a guest faculty of Katholische Universität Eichstätt-Ingolstadt. Currently, he leads the Women Entrepreneurship Project funded by CARE at LIBA. Professor L. S. Ganesh, Department of Management Studies, Indian Institute of Technology Madras, Chennai Prof. L.S.Ganesh served as the Head of the Department of Management Studies at IIT Madras from July 2004 till July 2008. He also coordinated the establishment of strategic academic relationships through MoUs between IIT Madras and leading national and multinational institutions (Indian School of Business at Hyderabad; Universities of Mannheim, Passau, and Bremen in Germany; Management Center at Innsbruck in Austria; State University of New York, Binghamton) to mention a few. -

Chennai District Origin of Chennai
DISTRICT PROFILE - 2017 CHENNAI DISTRICT ORIGIN OF CHENNAI Chennai, originally known as Madras Patnam, was located in the province of Tondaimandalam, an area lying between Pennar river of Nellore and the Pennar river of Cuddalore. The capital of the province was Kancheepuram.Tondaimandalam was ruled in the 2nd century A.D. by Tondaiman Ilam Tiraiyan, who was a representative of the Chola family at Kanchipuram. It is believed that Ilam Tiraiyan must have subdued Kurumbas, the original inhabitants of the region and established his rule over Tondaimandalam Chennai also known as Madras is the capital city of the Indian state of Tamil Nadu. Located on the Coromandel Coast off the Bay of Bengal, it is a major commercial, cultural, economic and educational center in South India. It is also known as the "Cultural Capital of South India" The area around Chennai had been part of successive South Indian kingdoms through centuries. The recorded history of the city began in the colonial times, specifically with the arrival of British East India Company and the establishment of Fort St. George in 1644. On Chennai's way to become a major naval port and presidency city by late eighteenth century. Following the independence of India, Chennai became the capital of Tamil Nadu and an important centre of regional politics that tended to bank on the Dravidian identity of the populace. According to the provisional results of 2011 census, the city had 4.68 million residents making it the sixth most populous city in India; the urban agglomeration, which comprises the city and its suburbs, was home to approximately 8.9 million, making it the fourth most populous metropolitan area in the country and 31st largest urban area in the world.