Patterns of GI Tract Injury
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Study of Mucin Turnover in the Small Intestine by in Vivo Labeling Hannah Schneider, Thaher Pelaseyed, Frida Svensson & Malin E
www.nature.com/scientificreports OPEN Study of mucin turnover in the small intestine by in vivo labeling Hannah Schneider, Thaher Pelaseyed, Frida Svensson & Malin E. V. Johansson Mucins are highly glycosylated proteins which protect the epithelium. In the small intestine, the goblet Received: 23 January 2018 cell-secreted Muc2 mucin constitutes the main component of the loose mucus layer that traps luminal Accepted: 26 March 2018 material. The transmembrane mucin Muc17 forms part of the carbohydrate-rich glycocalyx covering Published: xx xx xxxx intestinal epithelial cells. Our study aimed at investigating the turnover of these mucins in the small intestine by using in vivo labeling of O-glycans with N-azidoacetylgalactosamine. Mice were injected intraperitoneally and sacrifced every hour up to 12 hours and at 24 hours. Samples were fxed with preservation of the mucus layer and stained for Muc2 and Muc17. Turnover of Muc2 was slower in goblet cells of the crypts compared to goblet cells along the villi. Muc17 showed stable expression over time at the plasma membrane on villi tips, in crypts and at crypt openings. In conclusion, we have identifed diferent subtypes of goblet cells based on their rate of mucin biosynthesis and secretion. In order to protect the intestinal epithelium from chemical and bacterial hazards, fast and frequent renewal of the secreted mucus layer in the villi area is combined with massive secretion of stored Muc2 from goblet cells in the upper crypt. Te small intestinal epithelium is constantly aiming to balance efective nutritional uptake with minimal damage due to exposure to ingested, secreted and resident agents. -

Endocrine Tumors of the Pancreas
Friday, November 4, 2005 8:30 - 10:30 a. m. Pancreatic Tumors, Session 2 Chairman: R. Jensen, Bethesda, MD, USA 9:00 - 9:30 a. m. Working Group Session Pathology and Genetics Group leaders: J.–Y. Scoazec, Lyon, France Questions to be answered: 12 Medicine and Clinical Pathology Group leader: K. Öberg, Uppsala, Sweden Questions to be answered: 17 Surgery Group leader: B. Niederle, Vienna, Austria Questions to be answered: 11 Imaging Group leaders: S. Pauwels, Brussels, Belgium; D.J. Kwekkeboom, Rotterdam, The Netherlands Questions to be answered: 4 Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging ENETS Guidelines Neuroendocrinology 2004;80:394–424 Endocrine Tumors of the Pancreas - gastrinoma Epidemiology The incidence of clinically detected tumours has been reported to be 4-12 per million inhabitants, which is much lower than what is reported from autopsy series (about 1%) (5,13). Clinicopathological staging (12, 14, 15) Well-differentiated tumours are the large majority of which the two largest fractions are insulinomas (about 40% of cases) and non-functioning tumours (30-35%). When confined to the pancreas, non-angioinvasive, <2 cm in size, with <2 mitoses per 10 high power field (HPF) and <2% Ki-67 proliferation index are classified as of benign behaviour (WHO group 1) and, with the notable exception of insulinomas, are non-functioning. Tumours confined to the pancreas but > 2 cm in size, with angioinvasion and /or perineural space invasion, or >2mitoses >2cm in size, >2 mitoses per 20 HPF or >2% Ki-67 proliferation index, either non-functioning or functioning (gastrinoma, insulinoma, glucagonoma, somastatinoma or with ectopic syndromes, such as Cushing’s syndrome (ectopic ACTH syndrome), hypercaliemia (PTHrpoma) or acromegaly (GHRHoma)) still belong to the (WHO group 1) but are classified as tumours with uncertain behaviour. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
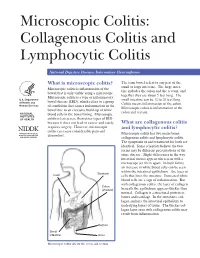
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -
Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #15 Seymour Katz, M.D., Series Editor Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease by Noel R. Fajardo and Darrell S. Pardi INTRODUCTION The prevalence of IBD, on the other hand, is higher nflammatory disorders of the intestines can be than microscopic colitis, reflecting the younger age of divided into those with macroscopic mucosal onset in patients with IBD. Ichanges (the traditional inflammatory bowel dis- In North America, the incidence of microscopic eases: ulcerative colitis and Crohn’s disease) and those colitis was 0.8/100,000 person-years from 1985 to with primarily microscopic changes. 1989, and this increased significantly to19.1/100,000 Microscopic colitis is a chronic diarrheal condi- from 1998 to 2001 (1). The incidence of collagenous tion that is separated into two main subtypes: collage- colitis and lymphocytic colitis was 5.1 and 9.8/100,000 nous colitis and lymphocytic colitis. These two condi- person-years, and the prevalence was 36 and tions have similar clinical and histologic features, but 64/100,000 persons, respectively (1). In Europe, the are distinguished by the presence or absence of a incidence of collagenous and lymphocytic colitis ranges thickened subepithelial collagen band. Inflammatory from 0.6 to 5.2/100,000 person-years with a prevalence bowel disease (IBD) is traditionally separated into two between 10 to 16/100,000 persons (2). The reason for distinct clinical entities: Crohn’s disease and ulcera- the significantly higher incidence and prevalence of MC tive colitis. Although there is considerable symptom in North America compared with Europe is not known, overlap between these diseases, there are several fea- though increasing recognition may play a role. -

Zollinger-Ellison Syndrome. Case Report
https://doi.org/10.15446/cr.v5n1.71686 ZOLLINGER-ELLISON SYNDROME. CASE REPORT Keywords: Gastrinoma; Zollinger-Ellison Sydrome; Multiple Endocrine Neoplasia Type 1. Palabras clave: Gastrinoma; Síndrome de Zollinger-Ellison; Neoplasia endocrina múltiple tipo 1. Juan Felipe Rivillas-Reyes Juan Leonel Castro-Avendaño Universidad Nacional de Colombia - Sede Bogotá - Facultad de Medicina - Programa de Medicina - Bogotá D.C. - Colombia. Héctor Fabián Martínez-Muñoz Universidad Nacional de Colombia - Sede Bogotá - Facultad de Medicina - Departamento de Cirugía - Bogotá D.C. - Colombia. Corresponding author Juan Felipe Rivillas-Reyes. Facultad de Medicina, Universidad Nacional de Colombia. Bogotá D.C. Colombia. Email: [email protected]. Received: 13/04/2018 Accepted: 20/11/2018 zollinger-ellison syndrome ABSTRACT RESUMEN 29 Introduction: The Zollinger-Ellison syndrome Introducción. El síndrome de Zollinger-Elli- (ZES) is a pathology caused by a neuroendo- son (SZE) es una patología producida por un crine tumor, usually located in the pancreas tumor neuroendocrino habitualmente localiza- or the duodenum, which is characterized by do a nivel duodenal o pancreático, el cual pro- elevated levels of gastrin, resulting in an ex- duce niveles elevados de gastrina, derivando cessive production of gastric acid. en hipersecreción de ácido gástrico. Case presentation: A 42-year-old female Presentación del caso. Paciente femenino patient with a history of longstanding peptic de 42 años con antecedente de enfermedad ulcer disease, who consulted due to persistent ulceropéptica de larga data, quién consulta por epigastric pain, melena and signs of peritoneal epigastralgia persistente y deposiciones meléni- irritation. Perforated peptic ulcer was suspect- cas y presenta signos de irritación peritoneal. Se ed, requiring emergency surgical intervention. -

Association of Helicobacter Pylori Infection and Chronic Atrophic
www.impactjournals.com/oncotarget/ Oncotarget, Vol. 7, No. 13 Association of helicobacter pylori infection and chronic atrophic gastritis with risk of colonic, pancreatic and gastric cancer: A ten-year follow-up of the ESTHER cohort study Xin-Zu Chen1,2,*, Ben Schöttker2,*, Felipe Andres Castro2, Hongda Chen2, Yan Zhang2, Bernd Holleczek2,3, Hermann Brenner2,4 1Department of Gastrointestinal Surgery, West China Hospital, Sichuan University, Chengdu, China 2Division of Clinical Epidemiology and Aging Research, German Cancer Research Center (DKFZ), Heidelberg, Germany 3Saarland Cancer Registry, Saarbrücken, Germany 4German Cancer Consortium (DKTK), Heidelberg, Germany *These authors contributed equally to this work Correspondence to: Hermann Brenner, e-mail: [email protected] Keywords: helicobacter pylori, chronic atrophic gastritis, colon cancer, pancreatic cancer, gastric cancer Received: November 21, 2015 Accepted: February 09, 2016 Published: March 06, 2016 ABSTRACT Objectives: To assess the association of H. pylori and chronic atrophic gastritis (AG) with colonic, pancreatic and gastric cancer in a population-based prospective cohort. Methods: Serum antibodies against H. pylori in general and specific to cytotoxin- associated gene A (CagA), as well as serum pepsinogen I and II were analyzed in 9,506 men and women, aged 50–75 years in a cohort study from Saarland, Germany. Incident cases of colonic, pancreatic and gastric cancer were ascertained by record linkage with data from the Saarland Cancer Registry. Results: During an average follow-up of 10.6 years, 108 colonic, 46 pancreatic and 27 gastric incident cancers were recorded. There was no association between H. pylori infection and colonic cancer (HR = 1.07; 95% CI 0.73–1.56) or pancreatic cancer (HR = 1.32; 0.73–2.39), regardless of either CagA seropositivity or AG status. -

Paneth Cell Α-Defensins HD-5 and HD-6 Display Differential Degradation Into Active Antimicrobial Fragments
Paneth cell α-defensins HD-5 and HD-6 display differential degradation into active antimicrobial fragments D. Ehmanna, J. Wendlera, L. Koeningera, I. S. Larsenb,c, T. Klaga, J. Bergerd, A. Maretteb,c, M. Schallere, E. F. Stangea, N. P. Maleka, B. A. H. Jensenb,c,f, and J. Wehkampa,1 aInternal Medicine I, University Hospital Tübingen, 72076 Tübingen, Germany; bQuebec Heart and Lung Institute, Department of Medicine, Faculty of Medicine, Cardiology Axis, Laval University, G1V 4G5 Quebec, QC, Canada; cInstitute of Nutrition and Functional Foods, Laval University, G1V 4G5 Quebec, QC, Canada; dElectron Microscopy Unit, Max-Planck-Institute for Developmental Biology, 72076 Tübingen, Germany; eDepartment of Dermatology, University Hospital Tübingen, 72076 Tübingen, Germany; and fNovo Nordisk Foundation Center for Basic Metabolic Research, Section for Metabolic Genomics, Faculty of Health and Medical Sciences, University of Copenhagen, 1165 Copenhagen, Denmark Edited by Lora V. Hooper, The University of Texas Southwestern, Dallas, TX, and approved January 4, 2019 (received for review October 9, 2018) Antimicrobial peptides, in particular α-defensins expressed by Paneth variety of AMPs but most abundantly α-defensin 5 (HD-5) and -6 cells, control microbiota composition and play a key role in intestinal (HD-6) (2, 17, 18). These secretory Paneth cells are located at the barrier function and homeostasis. Dynamic conditions in the local bottom of the crypts of Lieberkühn and are highly controlled by microenvironment, such as pH and redox potential, significantly af- Wnt signaling due to their differentiation and their defensin regu- fect the antimicrobial spectrum. In contrast to oxidized peptides, lation and expression (19–21). -
Familial Occurrence of Lymphocytic Colitis
BRIEF COMMUNICATION Familial occurrence of lymphocytic colitis Hugh J Freeman MD HJ Freeman. Familial occurrence of lymphocytic colitis. Can J Occurrence familiale de la colite Gastroenterol 2001;15(11):757-760. The familial occurrence lymphocytaire of lymphocytic colitis in a female parent and her two female children is reported. No other genetically based disorder, includ- RÉSUMÉ : On fait ici état de l’occurrence familiale de la colite lym- ing celiac disease, was evident. For both children, the age of phocytaire chez une patiente et ses deux filles. Aucune autre maladie diagnosis was more than two decades younger than the age of d’origine génétique, comme la maladie cæliaque, ne s’est manifestée. recognition of disease in the parent, and some clinical features, Pour les deux enfants, le diagnostic a été posé plus d’une vingtaine d’an- including the requirement for pharmacological agents in both nées avant l’âge qu’avait la mère au moment de son diagnostic et cer- taines caractéristiques cliniques, dont le traitement pharmacologique children, suggested that their disease severity was more signifi- chez les deux enfants, donnent à penser que leur maladie est plus grave cant than that of the involved parent. These characteristics of a que chez le parent atteint. Ces caractéristiques de la maladie familiale familial disease have been previously reported and labelled ont déjà été mentionnées et ont été appelées "anticipation génétique" ‘genetic anticipation’ in some monogenetic forms of neurologi- dans le cas de certaines formes monogénétiques de maladies neu- cal disease, as well as in other types of inflammatory bowel dis- rologiques, de même que dans d’autres types de maladies inflammatoires eases, including Crohn’s disease. -

In Patients with Crohn's Disease Gut: First Published As 10.1136/Gut.38.3.379 on 1 March 1996
Gut 1996; 38: 379-383 379 High frequency of helicobacter negative gastritis in patients with Crohn's disease Gut: first published as 10.1136/gut.38.3.379 on 1 March 1996. Downloaded from L Halme, P Karkkainen, H Rautelin, T U Kosunen, P Sipponen Abstract In a previous study we described upper gastro- The frequency of gastric Crohn's disease intestinal lesions characteristic of CD in 17% has been considered low. This study was of patients with ileocolonic manifestations of undertaken to determine the prevalence of the disease.10 Furthermore, 40% of these chronic gastritis and Helicobacter pylori patients had chronic, non-specific gastritis. infection in patients with Crohn's disease. This study aimed to determine the prevalence Oesophagogastroduodenoscopy was per- of chronic gastritis and that of H pylori infec- formed on 62 consecutive patients suffer- tion in patients with CD who had undergone ing from ileocolonic Crohn's disease. oesophagogastroduodenoscopy (OGDS) at the Biopsy specimens from the antrum and Fourth Department of Surgery, Helsinki corpus were processed for both histological University Hospital between 1989 and 1994. and bacteriological examinations. Hpylori antibodies of IgG and IgA classes were measured in serum samples by enzyme Patients and methods immunoassay. Six patients (9.70/o) were During a five year period from September 1989 infected with H pylorn, as shown by histo- to August 1994, OGDS was performed on 62 logy, and in five of them the infection consecutive patients with CD to establish the was also verified by serology. Twenty one distribution of their disease. During the study patients (32%) had chronic H pyloni period, the OGDS was repeated (one to seven negative gastritis (negative by both times) - on three patients because of anaemia histology and serology) and one of them and on five patients because of upper gastroin- also had atrophy in the antrum and corpus. -

Acute Diarrhea in Adults WENDY BARR, MD, MPH, MSCE, and ANDREW SMITH, MD Lawrence Family Medicine Residency, Lawrence, Massachusetts
Acute Diarrhea in Adults WENDY BARR, MD, MPH, MSCE, and ANDREW SMITH, MD Lawrence Family Medicine Residency, Lawrence, Massachusetts Acute diarrhea in adults is a common problem encountered by family physicians. The most common etiology is viral gastroenteritis, a self-limited disease. Increases in travel, comorbidities, and foodborne illness lead to more bacteria- related cases of acute diarrhea. A history and physical examination evaluating for risk factors and signs of inflammatory diarrhea and/or severe dehydration can direct any needed testing and treatment. Most patients do not require labora- tory workup, and routine stool cultures are not recommended. Treatment focuses on preventing and treating dehydra- tion. Diagnostic investigation should be reserved for patients with severe dehydration or illness, persistent fever, bloody stool, or immunosuppression, and for cases of suspected nosocomial infection or outbreak. Oral rehydration therapy with early refeeding is the preferred treatment for dehydration. Antimotility agents should be avoided in patients with bloody diarrhea, but loperamide/simethicone may improve symptoms in patients with watery diarrhea. Probiotic use may shorten the duration of illness. When used appropriately, antibiotics are effective in the treatment of shigellosis, campylobacteriosis, Clostridium difficile,traveler’s diarrhea, and protozoal infections. Prevention of acute diarrhea is promoted through adequate hand washing, safe food preparation, access to clean water, and vaccinations. (Am Fam Physician. 2014;89(3):180-189. Copyright © 2014 American Academy of Family Physicians.) CME This clinical content cute diarrhea is defined as stool with compares noninflammatory and inflamma- conforms to AAFP criteria increased water content, volume, or tory acute infectious diarrhea.7,8 for continuing medical education (CME). -

Gastrinoma: a Small Tumor with Big Symptoms
Case Report ISSN: 2574 -1241 DOI: 10.26717/BJSTR.2020.31.005159 Gastrinoma: A Small Tumor with Big Symptoms Hira Irfan1, Ahmed Imran Siddiqi1,2*, Waqas Shafiq1 and Umal Azmat1 1Department of Endocrinology, Shaukat Khanum memorial cancer hospital and research center, Lahore, Pakistan 2Department of Medicine Jersey General Hospital, Channel Islands UK *Corresponding author: Ahmed Imran Siddiqi, Department of Endocrinology, Shaukat Khanum memorial cancer hospital and research center, Lahore, Pakistan; Department of Medicine Jersey General Hospital, Channel Islands UK ARTICLE INFO ABSTRACT Received: November 04, 2020 Gastrinoma is rare gastrin secreting tumor and can be challenging to diagnose in the Published: November 11, 2020 absence of typical clinical features. Surgical resection remains the mainstay of treatment and can be curative, but the clinical presentation can compromise complete resection especially if the disease has already metastasized. We present here a 77-year-old lady Citation: Hira Irfan, Ahmed Imran Siddiqi, with abdominal pain and secretory diarrhea. Gastrinoma was diagnosed in a stepwise approach of investigations and then surgically removed. Following surgery, the patient Small Tumor with Big Symptoms. Biomed got prescribed octreotide for complete resolution of symptoms. Conservative treatment JWaqas Sci &Shafiq, Tech Umal Res Azmat.31(5)-2020. Gastrinoma: BJSTR. A is only recommended for patients unsuitable for surgery, with widespread metastasis and MS.ID.005159. on patients’ own choice. Abbreviations: NET: Neuroendocrine Tumors; ZES: Zollinger-Ellison Syndrome; MEN-1: Multiple Endocrine Neoplasia Type-1; SSTRs: Somatostatin Receptors; PTH: Parathyroid Hormone Introduction for a Gastrinoma (5). We report here a case of a 77-year-old lady Gastrinomas are functional neuroendocrine tumors (NET) diagnosed with a Gastrinoma. -

Autoimmune Diseases in Autoimmune Atrophic Gastritis
Acta Biomed 2018; Vol. 89, Supplement 8: 100-103 DOI: 10.23750/abm.v89i8-S.7919 © Mattioli 1885 Review Autoimmune diseases in autoimmune atrophic gastritis Kryssia Isabel Rodriguez-Castro1, Marilisa Franceschi1, Chiara Miraglia1, Michele Russo1, Antonio Nouvenne1, Gioacchino Leandro3, Tiziana Meschi1, Gian Luigi de’ Angelis1, Francesco Di Mario1 1 Endoscopy Unit, Department of Surgery, ULSS7-Pedemontana, Santorso Hospital, Santorso (VI), Italy; 2 Department of Me- dicine and Surgery, University of Parma, Parma, Italy; 3 National Institute of Gastroenterology “S. De Bellis” Research Hospital, Castellana Grotte, Italy Summary. Autoimmune diseases, characterized by an alteration of the immune system which results in a loss of tolerance to self antigens often coexist in the same patient. Autoimmune atrophic gastritis, characterized by the development of antibodies agains parietal cells and against intrinsic factor, leads to mucosal destruction that affects primarily the corpus and fundus of the stomach. Autoimmune atrophic gastritis is frequently found in association with thyroid disease, including Hashimoto’s thyroiditis, and with type 1 diabetes mellitus, Other autoimmune conditions that have been described in association with autoimmune atrophic gastritis are Ad- dison’s disease, chronic spontaneous urticaria, myasthenia gravis, vitiligo, and perioral cutaneous autoimmune conditions, especially erosive oral lichen planus. Interestingly, however, celiac disease, another frequent auto- immune condition, seems to play a protective role for