Health Systems Strengthening Quarterly Report April-June 2014 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Ppr) Infection in Sindh Province of Pakistan- a One Year Study
ALI ET AL (2019), FUUAST J.BIOL., 9(1): 149-157 PREVALENCE OF PESTE DES PETITS RUMINANTS (PPR) INFECTION IN SINDH PROVINCE OF PAKISTAN- A ONE YEAR STUDY SYED NOMAN ALI1,2, SHAHID ALI KHAN3, MASOOD VANDIAR4, RIASAT WASEE ULLAH5AND SHAHANA UROJ KAZMI6 1Livestock Department, Government of the Sindh 2Department of Agriculture & Agribusiness Management, University of Karachi, Pakistan. 3Food and Agriculture Organization of the United Nations, Islamabad Pakistan. ([email protected]). 4Central Veterinary Diagnostics Laboratory, Tando Jam. ([email protected]) 5Veterinary Research Institute, Lahore ([email protected]) 6Department of Microbiology and Immunology, Dadabhoy University (DIHE) & the University of Karachi, Pakistan ([email protected]) Corresponding author email: [email protected] الخہص وموجدہۺررسیچۺاپاتسکنۺےکۺوصہبۺدنسھۺںیمۺرکبویںۺاورۺڑیھبوںۺںیمۺاپےئۺوایلۺامیبریۺاکاٹ (PPR) یکۺوموجدیگ،ۺاابسبۺاورۺرٹنکولۺرکےنۺےکۺاکرۺآدمۺرطےقیۺولعممۺرکےنۺےکۺ ےئلۺیکۺیئگۺےہ۔ۺسجۺےکۺدورانۺایسۺامیبریۺیکۺ۷۴۸ۺۺوابء (Outbreaks)اکۺاجزئہۺایلۺایگۺوجۺوصہبۺدنسھۺےکۺ۹۲ۺںیمۺےسۺ۶۲االضعۺںیمۺاپیئۺیئگۺبسۺےسۺزایدہۺوابءۺ۱۵.۷۲ۺدصیفۺایٹمریۺعلضۺ ںیمۺاورۺبسۺےسۺمکۺرعےصۺیکۺوابءۺرمعۺوکٹۺعلضۺںیمۺراکیرڈۺیکۺیئگۺوجۺہکۺ ۵ۺدنۺیھتۺاسۺےکۺالعوہۺےبملۺرعہصۺیکۺامیبریۺﻻڑاکہنۺںیمۺاپیئۺیئگۺوجہک ۶۲ۺدنۺیھت۔ۺۺامیبریۺیکۺاشنوینںۺںیمۺمسجۺےکۺ درہجۺرحاتۺںیمۺااضہفF ۶ .۷۰۱ےسF ۲ .۲۰۱راکیرڈۺایکۺایگ۔ۺآوھکنںۺیکۺوسزش،ۺآوھکنںۺاورۺانکۺےسۺاگڑیۺرموطتب،ۺاھکیسنۺاورۺدتسۺاپےئۺےئگ،ۺہنمۺںیمۺوسمڑوںۺرپۺﻻلۺوسنجۺ ےکۺاشننۺےکۺاسھتۺزابنۺاورۺاگولںۺرپۺیھبۺوسنجۺاورۺزمخۺےکۺاشننۺاپےئۺےئگ۔ ELISAےکۺےجیتنۺرپ ANOVA -

National Plantation Drive QUICK FACTS Cities and Villages
level of air pollution in the National Plantation Drive QUICK FACTS cities and villages. Pakistan is one of the youngest and fastest Duration: 2020 - 2021 Implementing partners: Daraz Pakistan , Shan Foods developing countries of the world. Pvt Limited Karachi is among the most polluted cities in the Location: Karachi, Sindh world. The air of the city is polluted with high Funding partners: Daraz Pakistan, Shan Foods levels of lead and cadmium that pose a grave [email protected] risk to public health, says a recent study that also points out that the average concentration of these trace metals found in residential areas of Karachi is higher than those found in Delhi and Beijing. In another environmental study, the research team has found that Karachi, Pakistan, holds the world’s title for ozone. Of the nearly 300 measurements collected over 1 year, roughly a third exceeded what the researchers considered a “harmful” threshold for ozone, which can lead to smog. UNAP is planning a project of plantation and forestation in the province of Sindh. It will be a contribution to SDG 13 (Climate Action) which aims to conserve and restore the use of terrestrial ecosystems such as forests, wetlands, drylands and mountains by 2020. Halting deforestation is also vital to mitigating the impact of climate change. It calls for action to reduce the high Page | 1 UNAP partners with people at all levels of society to help build nations that can withstand crisis, and drive and sustain the kind of growth that improves the quality of life for everyone. Programme Outputs • Considering the land and forest situation in Sindh, especially the urban area of Karachi, a plantation project is planned to improve the environment and ecosystem of Karachi and Umerkot District, which is currently under the threat of a major environment threatening factor: air By 2020, ensure the conservation, pollution. -

SEF Assisted Schools (SAS)
Sindh Education Foundation, Govt. of Sindh SEF Assisted Schools (SAS) PRIMARY SCHOOLS (659) S. No. School Code Village Union Council Taluka District Operator Contact No. 1 NEWSAS204 Umer Chang 3 Badin Badin SHUMAILA ANJUM MEMON 0333-7349268 2 NEWSAS179 Sharif Abad Thari Matli Badin HAPE DEVELOPMENT & WELFARE ASSOCIATION 0300-2632131 3 NEWSAS178 Yasir Abad Thari Matli Badin HAPE DEVELOPMENT & WELFARE ASSOCIATION 0300-2632131 4 NEWSAS205 Haji Ramzan Khokhar UC-I MATLI Matli Badin ZEESHAN ABBASI 0300-3001894 5 NEWSAS177 Khan Wah Rajo Khanani Talhar Badin HAPE DEVELOPMENT & WELFARE ASSOCIATION 0300-2632131 6 NEWSAS206 Saboo Thebo SAEED PUR Talhar Badin ZEESHAN ABBASI 0300-3001894 7 NEWSAS175 Ahmedani Goth Khalifa Qasim Tando Bago Badin GREEN CRESCENT TRUST (GCT) 0304-2229329 8 NEWSAS176 Shadi Large Khoski Tando Bago Badin GREEN CRESCENT TRUST (GCT) 0304-2229329 9 NEWSAS349 Wapda Colony JOHI Johi Dadu KIFAYAT HUSSAIN JAMALI 0306-8590931 10 NEWSAS350 Mureed Dero Pat Gul Mohammad Johi Dadu Manzoor Ali Laghari 0334-2203478 11 NEWSAS215 Mureed Dero Mastoi Pat Gul Muhammad Johi Dadu TRANSFORMATION AND REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 12 NEWSAS212 Nabu Birahmani Pat Gul Muhammad Johi Dadu TRANSFORMATION & REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 13 NEWSAS216 Phullu Qambrani Pat Gul Muhammad Johi Dadu TRANSFORMATION AND REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 14 NEWSAS214 Shah Dan Pat Gul Muhammad Johi Dadu TRANSFORMATION AND REFLECTION FOR RURAL DEVELOPMENT (TRD) 0334-0455333 15 RBCS002 MOHAMMAD HASSAN RODNANI -

PAKISTAN-SINDH August 2019 – Projection Until December 2019 Report # 0001 | Issued in September 2019
IPC ACUTE MALNUTRITION ANALYSIS PAKISTAN-SINDH August 2019 – Projection until December 2019 Report # 0001 | Issued in September 2019 Key Figures August 2019 SAM* 365,209 Number of cases 1,000,458 MAM* Number of 6-59 months children acutely 635,249 Number of cases malnourished IN NEED OF TREATMENT GAM* 1,000,458 Number of cases How Severe, How Many and When – Acute malnutrition is a major public health problem in all the 8 drought affected districts in the Sindh province. Two districts in the province have extremely critical levels (IPC AMN Phase 5) of acute malnutrition– i.e. about every third child in these districts is suffering from acute malnutrition. Six other districts have critical levels (IPC AMN Phase 4) of acute malnutrition. Although the 6 districts are classified as in IPC AMN Phase 4, 2 of them have acute malnutrition closer to IPC AMN Phase 5. Where – Among the 8 drought affected districts notified by Govt. of Sindh in 2018, the districts with extremely critical levels of acute malnutrition are namely Tharparkar and Umerkot. Six other districts such as Jamshoro, Kambar Shahdadkot, Badin, Dadu, Sanghar, and Thatta are classified as being in IPC AMN Phase 4. Of these 6 districts, 2 of them, i.e. Kambar Shahdadkot and Badin, have acute malnutrition levels very close to IPC AMN Phase 5. Why – The major factors contributing to acute malnutrition include very poor quality and quantity of food, high food insecurity, poor sanitation coverage, and high incidence of low birthweight. Additionally, exclusive breastfeeding and access to safe drinking water are also of concern in several districts. -

COVID-19 EMERGENCY RESPONSE Daily Situation Report
COVID-19 EMERGENCY RESPONSE Daily Situation Report- April 13, 2020 Sindh Rural Support Organizaiton (SRSO) SRSO Complex, Shikarpur Road, Sukkur (Sindh), Pakistan, Ph.#: 071-56271820 Website: www.srso.org.pk Daily Situation Report – April 13, 2020 All the cities of Sindh are locked down. Daily wagers faced much difficulties to meet their ends. In such a pandemic and lockdown situation poor people of the community cannot afford their basic needs of life. In this situation, the Community didn’t leave alone to the poor daily wagers and elderly people of their communities. SRSO through representatives of community institutions (CIs) and staff are responding COVID-19 emergency within its outreach areas through Community Savings, Ration and Vegetables Distribution, Linkages Development, Identification of deserving HHs, delivering awareness sessions on precautionary measures to fight COVID-19 and Registration of needy and poor families under the Govt. of Pakistan Ehsaas Emergency Cash Programme. Households and individuals are being supported with Cash, Ration and capitalizing LSO linkages for relief activities in their concerned areas. SRSO well trained human capital is engaged in Government relief activities through identification of deserving beneficiaries, distribution of ration bags, conducting awareness sessions on preventive measures to combat COVID-19 SRSO is also facilitating the Government of Sindh in the identification of deserving families and distribution of food items in most needy households. SRSO outreach and scale of response -

Health Systems Strengthening Quarterly Report January-March 2014 2
USAID’s MCH Program Component 5: Health Systems Strengthening Quarterly Report January-March 2014 Cooperative Agreement No. AID-391-A-13-00002 This Report has been submitted to the United States Agency for International Development for consideration and approval. It was submitted by JSI Research & Training Institute, Inc. and prepared by JSI Research & Training Institute, Inc. in collaboration with Contech, Rural Support Programmes Network, and Heartfile. USAID’s MCH Program Component 5: Health Systems Strengthening Quarterly Report January-March 2014 Cooperative Agreement No. AID-391-A-13-00002 Disclaimer: “This study/report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of JSI Research & Training Institute, Inc. and do not necessarily reflect the views of USAID or the United States Government.” Component 5: Health Systems Strengthening Quarterly Report January-March 2014 2 Contents Acronyms 4 I. Executive Summary 5 II. Health Systems Strengthening Component’s Vision of Success 6 III. Activities and Results 8 IR 3.1 Increased Accountability and Transparency of Health System 8 IR 3.2 Improved Management Capacity at Provincial and District levels within the 21 Health Department IR 3.3 Strengthened Public Private Partnerships 25 IV. Coordination 29 V. Monitoring, Evaluation, and Reporting 30 VI. Issues and Challenges 35 VII. Activities Planned for Next Quarter 35 VIII. Annexes Annex 1: District-wise Details of Private -
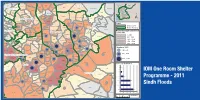
Building Back Stronger
IOM One Room Shelters - 2011 Sindh Floods Response uc, manjhand odero lal village kamil hingoro jhando mari Punjab sekhat khirah Balochistan dasori San gha r ismail jo goth odero lal station khan khahi bilawal hingorjo Matiari roonjho khokhrapar matiari mirabad balouchabad tando soomro chhore bau khan pathan piyaro lund turk ali mari mirpurkhas-05 Sindh shaikh moosa daulatpur shadi pali tajpur pithoro shah mardan shah dhoro naro i m a khan samoon sabho kaplore jheluri Tando Allahpak singhar Yar mosu khatian ii iii iv missan tandojam dhingano bozdar hingorno khararo syed umerkot mirpur old haji sawan khan satriyoon Legend atta muhammad palli tando qaiser araro bhurgari began jarwar mir ghulam hussain Union Council bukera sharif tando hyder dengan sanjar chang mirwah Ume rkot District Boundary hoosri gharibabad samaro road dad khan jarwar girhore sharif seriHyd erabmoolan ad Houses Damaged & Destroyed tando fazal chambar-1 chambar-2 Mirpur Khas samaro kangoro khejrari - Flood 2011 mir imam bux talpur latifabad-20 haji hadi bux 1 - 500 kot ghulam muhammad bhurgari mir wali muhammad latifabad-22 shaikh bhirkio halepota faqir abdullah seri 501 - 1500 ghulam shah laghari padhrio unknown9 bustan manik laghari digri 1501 - 2500 khuda dad kunri 2501 - 3500 uc-iii town t.m. khan pabban tando saindad jawariasor saeedpur uc-i town t.m. khan malhan 3501 - 5000 tando ghulam alidumbalo shajro kantio uc-ii town t.m. khan phalkara kunri memon Number of ORS dilawar hussain mir khuda bux aahori sher khan chandio matli-1 thari soofan shah nabisar road saeed -

Pakistan Multi-Sectoral Action for Nutrition Program
SFG3075 REV Public Disclosure Authorized Pakistan Multi-Sectoral Action for Nutrition Program Public Disclosure Authorized Environmental and Social Management Framework (ESMF) Directorate of Urban Policy & Strategic Planning, Planning & Public Disclosure Authorized Development Department, Government of Sindh Final Report December 2016 Public Disclosure Authorized Environmental and Social Management Framework Final Report Executive Summary Local Government and Housing Town Planning Department, GOS and Agriculture Department GOS with grant assistance from DFID funded multi donor trust fund for Nutrition in Pakistan are planning to undertake Multi-Sectoral Action for Nutrition (MSAN) Project. ESMF Consultant1 has been commissioned by Directorate of Urban Policy & Strategic Planning to fulfil World Bank Operational Policies and to prepare “Environmental and Social Management Framework (ESMF) for MSAN Project” at its inception stage via assessing the project’s environmental and social viability through various environmental components like air, water, noise, land, ecology along with the parameters of human interest and mitigating adverse impacts along with chalking out of guidelines, SOPs, procedure for detailed EA during project execution. The project has two components under Inter Sectoral Nutrition Strategy of Sindh (INSS), i) the sanitation component of the project aligns with the Government of Sindh’s sanitation intervention known as Saaf Suthro Sindh (SSS) in 13 districts in the province and aims to increase the number of ODF villages through certification while ii) the agriculture for nutrition (A4N) component includes pilot targeting beneficiaries for household production and consumption of healthier foods through increased household food production in 20 Union Councils of 4 districts. Saaf Suthro Sindh (SSS) This component of the project will be sponsored by Local Government and Housing Town Planning Department, Sindh and executed by Local Government Department (LGD) through NGOs working for the Inter-sectoral Nutrition Support Program. -

Umerkot Status
Rainfall Status of Tharparkar and Umerkot Districts August 25, 2020 Monsoon rains have created disaster in district Tharparkar and Umerkot, especially in Thar two Taluka Diplo and Mithi and Taluka Umerkot and Kunri in Umerkot district. The rain was started from 23 August 2020 and has been remained continue till today 2 5 August 2020 (3pm). Deputy Commissioner Office of Tharparkar and Umerkot declared emergency in risky areas. In Umerkot, All principals and other teaching and non teaching staff has been directed to remain in their school and make necessary arrangement to rescue rain affected people and provide them residency in school premises. District authority along with NGOs made contingency plans to meet the emergency situation. (District wise) Status of Rainfall: Tharparkar Status Umerkot Status # Taluka Name Rainfall in (mm) 23-08-2020 to 25-08-2020 # Taluka Name Rainfall in (mm) 01 Chachro 252 24-08-2020 to 25-08-2020 (3pm) 02 Dahli 216 03 Nangarparkar 367 01 Umerkot 214 04 Diplo 426 02 Kunri 272 05 Mithi 447 03 Samaro 144 06 Islam Kot 320 04 Pithoro 154 07 Kaloe 215 Losses and Damages: (District wise) Tharparkar and Umerkot (Report as of August 25, 2020 3pm) . One camel died in Chelhar town . Lightening damaged many trees in both districts . Seven Goats died in Village Phararo of Diplo Tehsil . One woman died in Village Batayinoon Soomra of Tehsil Diplo . One boy Allah Bux Wassan died in Village Nohato of Tharparkar District . One father and his son died due to sky lightening in Village Dhori of Mithi Tehsil . Two goats died near the police station of Kaloi . -

Weekly Epidemiological Bulletin Disease Early Warning System and Response in Pakistan
Weekly Bulletin Epidemiological Disease early warning system and response in Pakistan Volume 3, Issue 11, Wednesday 21 March 2012 Highlights Priority diseases under surveillance Epidemiological week no. 11 (11 to 17 March 2012) in DEWS Acute (Upper) Respiratory Infection • In week 11, 2012, total 85 districts including 3 agencies provided surveillance data to the Pneumonia DEWS on weekly basis from around 1,947 health facilities. Data from mobile teams is reported Suspected Diphtheria through sponsoring BHU or RHC. Suspected Pertussis Acute Watery Diarrhoea Bloody diarrhoea • A total of 689,606 consultations were reported through DEWS of which 23% were acute Other Acute Diarrhoea respiratory infections (ARI); 6% were acute diarrhoea; 4% were suspected malaria; while 4% were Suspected Enteric/Typhoid Fever Skin disease. Suspected Malaria Suspected Meningitis Suspected Dengue fever • A total of 204 alerts with 30 outbreaks were reported/identified in week 11, 2012: Alto‐ Suspected Viral Hemorrhagic Fever gether 89 alerts for Measles; 22 for Typhoid; 21 for Leishmaniasis; 17 for ARI; 10 for NNT and Pyrexia of Unknown Origin tetanus; 9 Pertussis; 7 for Scabies; 6 for AWD; 5 for AD; 4 for DF; 3 each for AJS, BD and Malaria; Suspected Measles Suspected Acute Viral Hepatitis 2 each for Diphtheria and Unexplained fever; while 1 for Rabies. Chronic Viral Hepatitis Neonatal Tetanus • As of 15 March 2012, the total number of polio cases confirmed by the laboratory is 14 Acute Flaccid Paralysis from 10 districts/towns/tribal agencies and areas. Scabies Cutaneous Leishmaniasis Others Figure‐1: Weekly trend of Acute diarrhoea, Bloody diarrhoea, ARI and Suspected malaria in Pakistan, Week‐1, 2011 to week‐11, 2012. -

Development Statistics of Sindh 2017
DEVELOPMENT STATISTICS OF SINDH 201 7 BUREAU OF STATISTICS PLANNING & DEVELOPMENT DEPARTMENT GOVERNMENT OF SINDH KARACHI-75600 FOR OFFICIAL USE ONLY DDEEVVEELLOOPPMMEENNTT SSTTAATTIISSTTIICCSS OOff SSIINNDDHH 22001177 PREFACE Sindh Bureau of Statistics has been annually releasing “Development Statistics of Sindh” since 1971. It provides latest and important statistical data on socio-economic sectors (Climate, Population, Agriculture, Fishery, Forestry, Livestock, Food, Grain, Manufacturing, Electricity, Gas, Mining, Public Finance, Financial Institutions, Transport & Communication, Education, Health and Crime) of the Sindh province with district-wise breakdown. Information relating to National Accounts, Banking and Foreign Trade has been given at national level. Bureau of Statistics is extremely thankful to the line Departments Government of Sindh, autonomous bodies and corporations functioning at federal and provincial level for cooperation in Providing requisite data for this publication. We look forward to their cooperation in future as well. It is hoped that data contained in this publication will be of immense use for administrators, planners, policy makers, research scholars and other users. I would like to convey my deep appreciation to the officers/ officials of technical section of this Bureau for the hard work put in to bringing out this publication, which I feel will provide the best avenue for planning & decision making in Sindh. For convenience and easy accessibility of the data, the publication is always available on the official website of this Bureau of statistics www.sindhbos.gov.pk Further suggestions from users for the improvement of format and contents of this publication will be highly appreciated and incorporated in neat issue. Dr. NAEEEMUZ-ZAFAR Director General BUREAU OF STATISTICS Government of Sindh, P.O. -

Weekly Epidemiological Bulletin Disease Early Warning System and Response in Pakistan
Weekly Bulletin Epidemiological Disease early warning system and response in Pakistan Volume 3, Issue 10, Wednesday 14 March 2012 Highlights Priority diseases under surveillance Epidemiological week no. 10 (4 to 10 March 2012) in DEWS Acute (Upper) Respiratory Infection • In week 10, 2012, total 84 districts including 2 agencies provided surveillance data to the Pneumonia DEWS on weekly basis from around 1,878 health facilities. Data from mobile teams is reported Suspected Diphtheria through sponsoring BHU or RHC. Suspected Pertussis Acute Watery Diarrhoea Bloody diarrhoea • A total of 672,038 consultations were reported through DEWS of which 23% were acute Other Acute Diarrhoea respiratory infections (ARI); 6% were acute diarrhoea; 4% were suspected malaria; while 5% were Suspected Enteric/Typhoid Fever Skin disease. Suspected Malaria Suspected Meningitis Suspected Dengue fever • A total of 203 alerts with 12 outbreaks were reported in week 10, 2012: Altogether 94 alerts Suspected Viral Hemorrhagic Fever for Measles; 22 for Leishmaniasis; 17 for Typhoid; 14 for Pertussis; 12 for ARI; 11 for NNT and Pyrexia of Unknown Origin Tetanus; 9 for AWD; 8 for Scabies; 5 for AD; 3 for Bloody diarrhoea; while 2 each for AJS, DF, Suspected Measles Suspected Acute Viral Hepatitis Diptheria and Malaria. Chronic Viral Hepatitis Neonatal Tetanus • As of 10 March 2012, the total number of polio cases confirmed by the laboratory is 13 Acute Flaccid Paralysis from 10 districts/towns/tribal agencies and areas. Scabies Cutaneous Leishmaniasis Others Figure‐1: Weekly trend of Acute diarrhoea, Bloody diarrhoea, ARI and Suspected malaria in Pakistan, Week‐1, 2011 to week‐10, 2012.