Obstetrics & Gynecology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Analysis of Adnexal Mass Managed During Cesarean Section
Original papers Analysis of adnexal mass managed during cesarean section Cheng Yu*1,2,B–D, Jie Wang*1,B–D, Weiguo Lu1,C,E, Xing Xie1,A,E, Xiaodong Cheng1,B,C, Xiao Li1,A,B,F 1 Women's Hospital, Zhejiang University School of Medicine, Hangzhou, China 2 Hangzhou Women's Hospital, China A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation; D – writing the article; E – critical revision of the article; F – final approval of the article Advances in Clinical and Experimental Medicine, ISSN 1899–5276 (print), ISSN 2451–2680 (online) Adv Clin Exp Med. 2019;28(4):447–452 Address for correspondence Abstract Xiao Li E-mail: [email protected] Background. Pregnancy with an adnexal mass is one of the most common complications during pregnancy * Cheng Yu and Jie Wang contributed equally and clinicians are sometimes caught in a dilemma concerning the decision to be made regarding clinical to this article. management. Funding sources Objectives. The objective of this study was to outline and discuss the clinical features, management and This study was funded by the projects of Zhejiang outcomes of adnexal masses that were encountered during a cesarean section (CS) at a university-affiliated Province Natural Scientific Foundation for Distin- hospital in China. guished Young Scientists (grant No. LR15H160001) and by Foundation of Science and Techno logy Material and methods. The medical records of the patients with an adnexal mass observed during Department of Zhejiang Province, China (grant No. 2012C13019-3). a CS were retrospectively collected at Women's Hospital, Zhejiang University School of Medicine, Hangzhou, China, from January 1991 to December 2011. -

American Family Physician Web Site At
Diagnosis and Management of Adnexal Masses VANESSA GIVENS, MD; GREGG MITCHELL, MD; CAROLYN HARRAWAY-SMITH, MD; AVINASH REDDY, MD; and DAVID L. MANESS, DO, MSS, University of Tennessee Health Science Center College of Medicine, Memphis, Tennessee Adnexal masses represent a spectrum of conditions from gynecologic and nongynecologic sources. They may be benign or malignant. The initial detection and evaluation of an adnexal mass requires a high index of suspicion, a thorough history and physical examination, and careful attention to subtle historical clues. Timely, appropriate labo- ratory and radiographic studies are required. The most common symptoms reported by women with ovarian cancer are pelvic or abdominal pain; increased abdominal size; bloating; urinary urgency, frequency, or incontinence; early satiety; difficulty eating; and weight loss. These vague symptoms are present for months in up to 93 percent of patients with ovarian cancer. Any of these symptoms occurring daily for more than two weeks, or with failure to respond to appropriate therapy warrant further evaluation. Transvaginal ultrasonography remains the standard for evaluation of adnexal masses. Findings suggestive of malignancy in an adnexal mass include a solid component, thick septations (greater than 2 to 3 mm), bilaterality, Doppler flow to the solid component of the mass, and presence of ascites. Fam- ily physicians can manage many nonmalignant adnexal masses; however, prepubescent girls and postmenopausal women with an adnexal mass should be referred to a gynecologist or gynecologic oncologist for further treatment. All women, regardless of menopausal status, should be referred if they have evidence of metastatic disease, ascites, a complex mass, an adnexal mass greater than 10 cm, or any mass that persists longer than 12 weeks. -

Congenital Uterine Anomalies: the Role of Surgery Maria Carolina Fernandes Lamouroux Barroso M 2021
MESTRADO INTEGRADO EM MEDICINA Congenital uterine anomalies: the role of surgery Maria Carolina Fernandes Lamouroux Barroso M 2021 Congenital uterine anomalies: the role of surgery Dissertação de candidatura ao grau de Mestre em Medicina, submetida ao Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto Maria Carolina Fernandes Lamouroux Barroso Aluna do 6º ano profissionalizante de Mestrado Integrado em Medicina Afiliação: Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto Endereço: Rua de Jorge Viterbo Ferreira nº228, 4050-313 Porto Endereço eletrónico: [email protected]; [email protected] Orientador: Dra. Márcia Sofia Alves Caxide e Abreu Barreiro Diretora do Centro de Procriação Medicamente Assistida e do Banco Público de Gâmetas do Centro Materno-Infantil do Norte Assistente convidada, Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto. Afiliação: Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto Endereço: Largo da Maternidade de Júlio Dinis 45, 4050-651 Porto Endereço eletrónico: [email protected] Coorientador: Prof. Doutor Hélder Ferreira Coordenador da Unidade de Cirurgia Minimamente Invasiva e Endometriose do Centro Materno- Infantil do Norte Professor associado convidado, Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto. Afiliação: Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto Endereço: Rua Júlio Dinis 230, B-2, 9º Esq, Porto Endereço eletrónico: [email protected] Junho 2021 Porto, junho de 2021 ____________________________________ (Assinatura da estudante) ____________________________________ (Assinatura da orientadora) ____________________________________ (Assinatura do coorientador) ACKNOWLEDGEMENTS À Dra. Márcia Barreiro, ao Dr. Luís Castro e ao Prof. Doutor Hélder Ferreira, por toda a disponibilidade e empenho dedicado à realização deste trabalho. Aos meus pais, irmão e avós, pela participação que desde sempre tiveram na minha formação, e pelo carinho e apoio incondicional. -

Sl.No CGHS Treatment Procedure/Investigation List Rates for Non NABH Rates for NABH CGHS Bengaluru Rate List
CGHS Bengaluru Rate List Sl.No CGHS Treatment Procedure/Investigation Rates for Non Rates for List NABH NABH 1 Consultation OPD 135 135 2 Consultation- for Inpatients 270 270 3 Dressings of wounds 45 52 4 Suturing of wounds with local anesthesia 108 124 5 Aspiration Plural Effusion - Diagnostic 120 138 6 Aspiration Plural Effusion - Therapeutic 174 200 7 Abdominal Aspiration - Diagnostic 330 380 8 Abdominal Aspiration - Therapeutic 414 476 9 Pericardial Aspiration 342 393 10 Joints Aspiration 285 329 11 Biopsy Skin 207 239 12 Removal of Stitches 36 41 13 Venesection 124 143 14 Phimosis Under LA 1180 1357 15 Sternal puncture 173 199 16 Injection for Haemorrhoids 373 428 17 Injection for Varicose Veins 315 363 18 Catheterisation 425 500 19 Dilatation of Urethra 450 518 20 Incision & Drainage 378 435 21 Intercostal Drainage 125 144 22 Peritoneal Dialysis 1319 1517 TREATMENT PROCEDURE SKIN 23 Excision of Moles 311 357 24 Excision of Warts 279 321 25 Excision of Molluscum contagiosum 117 135 26 Excision of Veneral Warts 144 166 27 Excision of Corns 126 145 28 I/D Injection Keloid 97 112 29 Chemical Cautery (s) 99 114 TREATMENT PROCEDURE OPTHALMOLOGY 30 66 76 eyes Subconjunctival/subtenon’s injections in one 31 132 152 eyes 32 PterygiumSubconjunctival/subtenon’s Surgery injections in both 5550 6325 33 Conjunctival Peritomy 58 67 34 Conjunctival wound repair or exploration 3300 3795 following blunt trauma 35 Removal of corneal foreign body 115 132 36 Cauterization of ulcer/subconjunctival injection 69 79 in one eye 37 Cauterization of ulcer/subconjunctival -
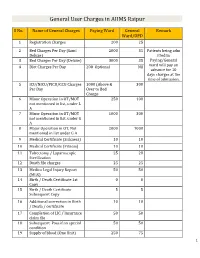
General User Charges in AIIMS Raipur
General User Charges in AIIMS Raipur S No. Name of General Charges Paying Ward General Remark Ward/OPD 1 Registration Charges 200 25 2 Bed Charges Per Day (Sami 2000 35 Patients being adm Deluxe) itted in 3 Bed Charges Per Day (Deluxe) 3000 35 Paying/General 4 Diet Charges Per Day 200 Optional Nil ward will pay an advance for 10 days charges at the time of admission. 5 ICU/NICU/PICU/CCU Charges 1000 (Above & 300 Per Day Over to Bed Charge 6 Minor Operation in OT/MOT 250 100 not mentioned in list, under L A 7 Minor Operation in OT/MOT 1000 300 not mentioned in list, under G A 8 Major Operation in OT, Not 2000 1000 mentioned in list under G A 9 Medical Certificate (Sickness) 10 10 10 Medical Certificate (Fitness) 10 10 11 Tubectomy / Laparoscopic 25 20 Sterilization 12 Death file charges 25 25 13 Medico Legal Injury Report 50 50 (MLR) 14 Birth / Death Certificate 1st 0 0 Copy 15 Birth / Death Certificate 5 5 Subsequent Copy 16 Additional correction in Birth 10 10 / Death / certificate 17 Completion of LIC / Insurance 50 50 claim file 18 Subsequent Pass if on special 50 50 condition 19 Supply of blood (One Unit) 250 75 1 20 Medical Board Certificate 500 500 On Special Case User Charges for Investigations in AIIMS Raipur S No. Name of Investigations Paying General Remark Ward Ward/OPD Anaesthsia 1 ABG 75 50 2 ABG ALONGWITH 150 100 ELECTROLYTES(NA+,K+)(Na,K) 3 ONLY ELECTROLYTES(Na+,K+,Cl,Ca+) 75 50 4 ONLY CALCIUM 50 25 5 GLUCOSE 25 20 6 LACTATE 25 20 7 UREA. -

Theca Lutein Cyst Rupture - an Unusual Cause of Acute Abdomen : a Case Report P Dasari, K Prabhu, T Chitra
The Internet Journal of Gynecology and Obstetrics ISPUB.COM Volume 13 Number 1 Theca lutein cyst rupture - an unusual cause of acute abdomen : a case report P Dasari, K Prabhu, T Chitra Citation P Dasari, K Prabhu, T Chitra. Theca lutein cyst rupture - an unusual cause of acute abdomen : a case report. The Internet Journal of Gynecology and Obstetrics. 2009 Volume 13 Number 1. Abstract A 20 year old illiterate woman who had a spontaneous first trimester abortion followed by instrumental evacuation, presented 4 days later with sudden onset of pain and distension of abdomen along with difficulty in breathing. On examination, she was tachypnoeic, icteric with tachycardia. Abdominal examination revealed guarding and rigidity along with free fluid and vague mass in lower abdomen. Gynaecological examination showed purulent discharge through os with bogginess in all fornices. USG revealed echogenic fluid with bilateral large ovarian masses containing multiple small cysts. Laparotomy was performed with a provisional diagnosis of ruptured theca leutein cysts after 24 hrs of administration of broad spectrum antibiotics. There were bilateral theca leutein cysts of more than 10X15 cm, the left of which has ruptured and the right on the verge of rupture. Bilateral partial cystectomy was performed and histopathological examination confirmed theca lutein cysts with inflammatory infiltrate. INTRODUCTION performed for the same. She suffered from fever with chills The causes of distension of abdomen in the post-abortal from the next day and had diarrhoea and vomiting for 3 days period include peritonitis secondary to sepsis, perforation of for which she had over the counter medicines. All these uterus, intestinal obstruction, paralytic ileus, torsion of a symptoms subsided in 4 days. -

Shirodkar's Extended Manchester Repair
International Journal of Recent Trends in Science And Technology, ISSN 2277-2812 E-ISSN 2249-8109, Volume 10, Issue 2, 2014 pp 263-266 Shirodkar’s Extended Manchester Repair: A Conservative Vaginal Surgery for Genital Prolapse in Young Women and Reinforcement of Weak Uterosacral Ligaments with Merselene Tape: Retrospective and Prospective Study Roohi Shaikh 1, Suman Sardesai 2* 1Assistant Professor, Department of OBGY, Indian Institute of Medical Science and Research, Warudi, Badnapur, Jalna Maharashtra INDIA. 2Professor and HOD, Department of OBGY, Dr. V. M. Medical College, Solapur, INDIA. *Corresponding Address: *[email protected], #[email protected] Research Article Abstract: The aim of this study was to evaluate the results of ligaments to the anterior aspect of what remains of the Shirodkar Extended Manchester Repair operation for uterine cervix, an anterior colporrphaphy and perineorhhapy is prolapse in young women interested in retaining future done. This time honoured technique has various childbearing and menstrual function. Materials and Methods: 30 patients with II or III degree utero-vaginal prolapse with or without shortcomings i.e. cervical stenosis, infertility, cervical cystoenterorectocoele and with normal uterocervical length (i.e. no incompetence, cervical dystocia during labour, cervical elongation) in child-bearing age group (i.e. less than 35 dyspareunia and recurrence of prolapse after pregnancy or years) interested in preserving future fertility or menstrual function otherwise was also reported to the extent of 20-25% were operated and followed-up. In patients with weak uterosacral (Shaw 1933).An ideal conservative method should ligament, reinforcement with merselene tape was done. Results: In preserve menstruation, restore the fertility and should not this study, 79% of the patients were below the age of 30 years. -
Development and Validation of a Model for Individualized Prediction
Wu et al. Reproductive Biology and Endocrinology (2021) 19:6 https://doi.org/10.1186/s12958-020-00693-x RESEARCH Open Access Development and validation of a model for individualized prediction of cervical insufficiency risks in patients undergoing IVF/ICSI treatment Yaoqiu Wu1,2, Xiaoyan Liang1, Meihong Cai3, Linzhi Gao1, Jie Lan2 and Xing Yang1* Abstract Background: Women who conceived with in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) are more likely to experience adverse pregnancy outcomes than women who conceived naturally. Cervical insufficiency (CI) is one of the important causes of miscarriage and premature birth, however there is no published data available focusing on the potential risk factors predicting CI occurrence in women who received IVF/ICSI treatment. This study aimed to identify the risk factors that could be integrated into a predictive model for CI, which could provide further personalized and clinically specific information related to the incidence of CI after IVF/ICSI treatment. Patients and methods: This retrospective study included 4710 patients who conceived after IVF/ICSI treatment from Jan 2011 to Dec 2018 at a public university hospital. The patients were randomly divided into development (n = 3108) and validation (n = 1602) samples for the building and testing of the nomogram, respectively. Multivariate logistic regression was developed on the basis of pre-pregnancy clinical covariates assessed for their association with CI occurrence. Results: A total of 109 patients (2.31%) experienced CI among all the enrolled patients. Body mass index (BMI), basal serum testosterone (T), gravidity and uterine length were associated with CI occurrence. The statistical nomogram was built based on BMI, serum T, gravidity and uterine length, with an area under the curve (AUC) of 0.84 (95% confidence interval: 0.76–0.90) for the developing cohort. -

Fallopian Tubes
Joy of GettinG PreGnant Your Complete Guide To Overcome Infertility author / editor / Copyright © Dr. Rupal N. Shah, M.D., D.G.O., Diploma in Reproductive Medicine (Kiel), Germany Contact: [email protected] Publisher: Pugmarks Mediaa, 119, Swami Vivekanand Marg, Allahabad - 211003 (UP) first edition : 2013 Second edition : 2017 Concept / Layout Pugmarks Mediaa & Team IVF India available at: BlOSSOM FeRTIlITY & TeST TUBe BABY CeNTRe Sutaria Building, Near Bahumali Building, Nanpura, Surat - 395001, Gujarat, India Phone : 0261-2470333, 2470444, +91 99799 46222 email : info@blossomivfindia.com Website: www.blossomivfindia.com Cover: Raj Bhagat Printing: Vavo Prints, Bai-ka-Bagh, Allahabad iSBn: 978-81-932743-3-0 Price: Rs 250/- note: Contents of this booklet cannot be published elsewhere. The Opinions and contents of this booklet belongs to the doctor himself, and they are being published just to create awareness in the people. It should not be used by the patients for self diagnosis without medical advice. New therapeutics are updated due to technology and the contents of this booklet may be old or incomplete or with some errors and omissions. But purpose of this booklet is only public awareness and without Medical Ad - vice, no content of this booklet should be followed, as the composition of each patient is different, hence, it is not necessary that the content of this booklet is fit for your purpose. The patient will be responsible if this book is followed without any medical advice. If the content of this booklet is found with error or any injustice is found to be done by any one, he may kindly draw attention. -

Genetics of Recurrent and Spontaneous Miscarriage
Research and Reviews Journal of Medical and Health Science ISSN: 2319-9865 Genetics of Recurrent and Spontaneous Miscarriage Arka Dutta Gupta1* and Akash Baid2 1 Department of Human Genetics, Institute of Genetic Engineering, Madhyamgram, Badu, Itkhola, Kolkata, West Bengal 2 Department of Biotechnology, Institute of Genetic Engineering, Madhyamgram, Badu, Itkhola, Kolkata, West Bengal Research Article Received: 01/03/2017 ABSTRACT Revised: 20/03/2017 Accepted: 27/03/2017 The aim was to find out the genetic basis of recurrent spontaneous abortion (RSA) from the past pregnancies and ensure a more favourable *For Correspondence outcome in the current or future pregnancy. Pregnancy loss has always been Gupta AD, Department of Human a devastating experience for the mothers and the clinician of concern. One Genetics, Institute of Genetic out of four pregnancies ends in miscarriage. It is estimated that 50-60% of Engineering, Madhyamgram, all first trimester pregnancy losses are the cause of chromosomal Badu, Itkhola, Kolkata, West abnormality. Bengal, Tel: 8978764411. 8 couples were selected with the history of Recurrent Spontaneous fetal loss and were suggested ultrasound scan while no such abnormalities Keywords: Recurrent were found, hence further we asked for cytogenetic procedure for detection spontaneous miscarriage, Bad of chromosomal abnormalities by the method karyotyping. Obstetric History, chromosomal We discovered 45;X/46;XX, 45;X/46;XY and 46;XX/46;XY in female abnormalities partners and 46;XX/46;XY, 46;XY/47;XXY mosaicism in male partners. Two unique balanced translocations in females such as 46;XX,t(5q35:8q24) E-mail: and46;XX,t(14q:21q) and a single balanced translocation in male partner [email protected] 46;XY,t(6q:8p) with reproductive failure. -

UNMH Obstetrics and Gynecology Clinical Privileges Name
UNMH Obstetrics and Gynecology Clinical Privileges Name:____________________________ Effective Dates: From __________ To ___________ All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective April 28, 2017: Initial Privileges (initial appointment) Renewal of Privileges (reappointment) Expansion of Privileges (modification) INSTRUCTIONS: Applicant: Check off the “requested” box for each privilege requested. Applicants have the burden of producing information deemed adequate by the Hospital for a proper evaluation of current competence, current clinical activity, and other qualifications and for resolving any doubts related to qualifications for requested privileges. Department Chair: Check the appropriate box for recommendation on the last page of this form. If recommended with conditions or not recommended, provide condition or explanation. OTHER REQUIREMENTS: 1. Note that privileges granted may only be exercised at UNM Hospitals and clinics that have the appropriate equipment, license, beds, staff, and other support required to provide the services defined in this document. Site-specific services may be defined in hospital or department policy. 2. This document defines qualifications to exercise clinical privileges. The applicant must also adhere to any additional organizational, regulatory, or accreditation requirements that the organization is obligated to meet. --------------------------------------------------------------------------------------------------------------------------------------- -

Hyperreactio Luteinalis: Benign Disorder Masquerading As an Ovarian Malignancy
International Journal of Research in Medical Sciences Kaur PP et al. Int J Res Med Sci. 2018 May;6(5):1815-1817 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20181784 Case Report Hyperreactio luteinalis: benign disorder masquerading as an ovarian malignancy Kaur P. P.1, Ashima1, Isaacs R.1, Goyal S.2* 1Department of Pathology, 2Department of Obstetrics and Gynecology, Christian Medical College and Hospital, Ludhiana Received: 21 December 2017 Revised: 13 March 2018 Accepted: 28 March 2018 *Correspondence: Dr. Goyal S., E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Hyperreactio luteinalis (HL) refers to pregnancy related moderate to marked enlargement of the ovaries due to multiple benign theca lutein cysts. It is caused due to elevated Human chorionic gonadotropins leading to maternal complications such as preeclampsia and preterm delivery may result. We report case of a 24 years old lady, G3P1A1L1 with spontaneous twin pregnancy at 13 weeks + 4 days gestation presented with chief complaint of lower abdominal pain on exertion for 5 days. Ultrasonography (USG) showed a large left ovarian mass in Pouch of Douglas pushing uterus up and extending into the left side of midline upto costal cartilage. It showed multiple thick septations with vascularity pointing towards malignancy. CA-125 was elevated to 193U/ml.