Study Protocol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Human Papillomavirus 9-Valent Vaccine, Recombinant), for Use In
tools Approved Drugs FDA has approved a supplemental new drug propelled, joystick-controlled, easy-to-use application (sNDA) for Xtandi® colonoscope system. • The Food and Drug Administration (FDA) (enzalutamide) capsules in advanced has approved a supplemental biologics prostate cancer. • Varian Medical Systems (varian.com) has license application (sBLA) for the use of received 510(k) clearance from the FDA to Arzerra® (ofatumumab) (Genmab A/S, market the Nexus DR, a high resolution genmab.com) in combination with Drugs in the News imaging system for X-ray imaging using a fludarabine and cyclophosphamide for the digital X-ray detector. treatment of patients with relapsed chronic • Genentech (gene.com) has received a lymphocytic leukemia (CLL). second breakthrough therapy designation Approved Genetic Tests & from the FDA for Alecensa® (alectinib) Assays • Amgen (amgen.com) announced that the for the treatment of adult patients with FDA has approved the sBLA for Blincyto® advanced ALK-positive NSCLC who have • AstraZeneca (astrazeneca-us.com) (blinatumomab) to include new data not received prior treatment with an ALK announced that the FDA has approved a supporting the treatment of pediatric patients inhibitor. blood-based companion diagnostic for with Philadelphia chromosome-negative (Ph-) Tagrisso® (osimertinib). relapsed or refractory B-cell precursor acute • AbbVie (abbvie.com) submitted an sNDA lymphoblastic leukemia (ALL). to the FDA for Imbruvica® (ibrutinib) to treat patients with marginal zone lymphoma, • Merck Sharp & Dohme Corp.’s (merck.com) a form of non-Hodgkin’s lymphoma. FDA Approves Two-Dose Keytruda® (pembrolizumab) has received Vaccination Regime FDA approval in first-line non-small cell lung • Fate Therapeutics, Inc. -

Combinations of Immunotherapy and Radiation Therapy in Head and Neck Squamous Cell Carcinoma: a Narrative Review
2585 Review Article on Synergy in Action: Novel Approaches to Combining Radiation Therapy and Immunotherapy Combinations of immunotherapy and radiation therapy in head and neck squamous cell carcinoma: a narrative review Thomas J. Hayman1, Aarti K. Bhatia2, Krishan R. Jethwa1, Melissa R. Young1, Henry S. Park1^ 1Department of Therapeutic Radiology, Yale School of Medicine, New Haven, CT, USA; 2Section of Medical Oncology, Department of Medicine, Yale School of Medicine, New Haven, CT, USA Contributions: (I) Conception and design: TJ Hayman, HS Park; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: TJ Hayman, HS Park; (V) Data analysis and interpretation: TJ Hayman, HS Park; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Henry S. Park, MD, MPH. Assistant Professor of Therapeutic Radiology, Yale School of Medicine, 35 Park Street, Lower Level, New Haven, CT 06520, USA. Email: [email protected]. Abstract: Radiation therapy and systemic therapy are the primary non-surgical treatment modalities for head and neck squamous cell carcinoma (HNSCC). Despite advances in our biologic understanding of this disease and the development of novel therapeutics, treatment resistance remains a significant problem. It has become increasingly evident that the innate and adaptive immune systems play a significant role in the modulation of anti-tumor responses to traditional cancer-directed therapies. By inducing DNA damage and cell death, radiation therapy appears to activate both innate and adaptive immune responses. Immunotherapies targeting programmed cell death protein 1 (PD-1) and programmed cell death ligand 1 (PD-L1) also have yielded promising results, particularly in the recurrent/metastatic setting. -

TECENTRIQ® (Atezolizumab) Injection, for Intravenous Use DOSAGE FORMS and STRENGTHS Initial U.S
of 4-6 cycles. Following completion of chemotherapy, TECENTRIQ 1200 HIGHLIGHTS OF PRESCRIBING INFORMATION mg IV, following by bevacizumab, every 3 weeks. These highlights do not include all the information needed to use TECENTRIQ safely and effectively. See full prescribing information for If the first infusion is tolerated, all subsequent infusions may be delivered over TECENTRIQ. 30 minutes. (2.2, 2.3) TECENTRIQ® (atezolizumab) injection, for intravenous use DOSAGE FORMS AND STRENGTHS Initial U.S. Approval: 2016 Injection: 1200 mg/20 mL (60 mg/mL) solution in a single-dose vial (3) RECENT MAJOR CHANGES CONTRAINDICATIONS Indications and Usage, Urothelial Carcinoma (1.1) 7/2018 None. (4) Indications and Usage, Non-Small Cell Lung Cancer (1.2) 12/2018 Dosage and Administration (2.3) 7/2018 WARNINGS AND PRECAUTIONS Warnings and Precautions, Pneumonitis (5.1) 12/2018 Immune-Mediated Pneumonitis: Withhold or permanently discontinue Warnings and Precautions, Hepatitis (5.2) 12/2018 based on severity of pneumonitis. (2.4, 5.1) Warnings and Precautions, Colitis (5.3) 12/2018 Immune-Mediated Hepatitis: Monitor for changes in liver function. Warnings and Precautions, Endocrinopathies (5.4) 12/2018 Withhold or permanently discontinue based on severity of transaminase or Warnings and Precautions, Infections (5.6) 12/2018 total bilirubin elevation. (2.4, 5.2) Warnings and Precautions, Infusion-Related Reactions (5.7) 12/2018 Immune-Mediated Colitis: Withhold or permanently discontinue based on severity of colitis. (2.4, 5.3) INDICATIONS AND USAGE Immune-Mediated Endocrinopathies (2.4, 5.4): TECENTRIQ is a programmed death-ligand 1 (PD-L1) blocking antibody o Hypophysitis: Withhold based on severity of hypophysitis. -

Genmab Announces Studies of Daratumumab in Combination with Atezolizumab in a Solid Tumor and Multiple Myeloma
Genmab Announces Studies of Daratumumab in Combination with Atezolizumab in a Solid Tumor and Multiple Myeloma Company Announcement Phase Ib studies of daratumumab in combination with Roche’s immune checkpoint inhibitor atezolizumab in a solid tumor and multiple myeloma to be started Studies conducted under a clinical trial collaboration agreement between Janssen and Roche Copenhagen, Denmark; March 21, 2016 – Genmab A/S (Nasdaq Copenhagen: GEN) announced today that daratumumab will be investigated in early stage clinical studies in combination with atezolizumab (anti-PD-L1 antibody), in a solid tumor and multiple myeloma. The studies will be conducted under a clinical trial collaboration agreement between Genmab’s licensing partner for daratumumab, Janssen Biotech, Inc., and Genentech, a member of the Roche Group. Atezolizumab is an investigational monoclonal antibody designed to bind to a protein called PD-L1, which is expressed on tumor cells and tumor-infiltrating immune cells. Janssen will conduct a Phase Ib study of daratumumab in combination with atezolizumab to treat a solid tumor. Genentech will amend an ongoing Phase Ib study to assess atezolizumab in combination with daratumumab, with daratumumab and lenalidomide, and with daratumumab and pomalidomide in relapsed/refractory multiple myeloma (NCT02431208). The studies are expected to start enrolling patients later this year and information about the studies will be posted on www.clinicaltrials.gov. “We are very excited about the start of the first study to investigate daratumumab in a solid tumor, potentially expanding its clinical utility beyond hematological cancers. We are equally excited about testing daratumumab in combination with an immune checkpoint inhibitor, such as Roche’s anti-PDL1, atezolizumab, in multiple myeloma. -

Antibody–Drug Conjugates
Published OnlineFirst April 12, 2019; DOI: 10.1158/1078-0432.CCR-19-0272 Review Clinical Cancer Research Antibody–Drug Conjugates: Future Directions in Clinical and Translational Strategies to Improve the Therapeutic Index Steven Coats1, Marna Williams1, Benjamin Kebble1, Rakesh Dixit1, Leo Tseng1, Nai-Shun Yao1, David A. Tice1, and Jean-Charles Soria1,2 Abstract Since the first approval of gemtuzumab ozogamicin nism of activity of the cytotoxic warhead. However, the (Mylotarg; Pfizer; CD33 targeted), two additional antibody– enthusiasm to develop ADCs has not been dampened; drug conjugates (ADC), brentuximab vedotin (Adcetris; Seat- approximately 80 ADCs are in clinical development in tle Genetics, Inc.; CD30 targeted) and inotuzumab ozogami- nearly 600 clinical trials, and 2 to 3 novel ADCs are likely cin (Besponsa; Pfizer; CD22 targeted), have been approved for to be approved within the next few years. While the hematologic cancers and 1 ADC, trastuzumab emtansine promise of a more targeted chemotherapy with less tox- (Kadcyla; Genentech; HER2 targeted), has been approved to icity has not yet been realized with ADCs, improvements treat breast cancer. Despite a clear clinical benefit being dem- in technology combined with a wealth of clinical data are onstrated for all 4 approved ADCs, the toxicity profiles are helping to shape the future development of ADCs. In this comparable with those of standard-of-care chemotherapeu- review, we discuss the clinical and translational strategies tics, with dose-limiting toxicities associated with the mecha- associated with improving the therapeutic index for ADCs. Introduction in antibody, linker, and warhead technologies in significant depth (2, 3, 8, 9). Antibody–drug conjugates (ADC) were initially designed to leverage the exquisite specificity of antibodies to deliver targeted potent chemotherapeutic agents with the intention of improving Overview of ADCs in Clinical Development the therapeutic index (the ratio between the toxic dose and the Four ADCs have been approved over the last 20 years (Fig. -

A Phase Ib/II Study Evaluating the Safety and Efficacy Of
Official Title: A Phase Ib/II Study Evaluating the Safety and Efficacy of Obinutuzumab in Combination With Atezolizumab Plus Polatuzumab Vedotin in Patients With Relapsed or Refractory Follicular Lymphoma and Rituximab in Combination With Atezolizumab Plus Polatuzumab Vedotin in Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma NCT Number: NCT02729896 Document Date: Protocol Version 8: 07-November-2018 PROTOCOL TITLE: A PHASE Ib/II STUDY EVALUATING THE SAFETY AND EFFICACY OF OBINUTUZUMAB IN COMBINATION WITH ATEZOLIZUMAB PLUS POLATUZUMAB VEDOTIN IN PATIENTS WITH RELAPSED OR REFRACTORY FOLLICULAR LYMPHOMA AND RITUXIMAB IN COMBINATION WITH ATEZOLIZUMAB PLUS POLATUZUMAB VEDOTIN IN PATIENTS WITH RELAPSED OR REFRACTORY DIFFUSE LARGE B-CELL LYMPHOMA PROTOCOL NUMBER: BO29561 VERSION NUMBER: 8 EUDRACT NUMBER: 2015-004845-25 IND NUMBER: 128036 TEST PRODUCT: Obinutuzumab (RO5072759) Rituximab (RO0452294) Atezolizumab (RO5541267) Polatuzumab vedotin (RO5541077) MEDICAL MONITOR: , Ph.D. SPONSOR: F. Hoffmann-La Roche Ltd DATE FINAL: Version 1: 12 November 2015 DATES AMENDED: Version 2: 14 January 2016 Version 3: 28 June 2016 Version 4: 17 November 2016 Version 5: 4 May 2017 Version 6: 21 December 2017 Version 7: 1 May 2018 Version 8: See electronic date stamp below. PROTOCOL AMENDMENT APPROVAL Approver's Name Title Date and Time (UTC) Company Signatory 07-Nov-2018 02:00:10 CONFIDENTIAL This clinical study is being sponsored globally by F. Hoffmann-La Roche Ltd of Basel, Switzerland. However, it may be implemented in individual countries by Roche’s local affiliates, including Genentech, Inc. in the United States. The information contained in this document, especially any unpublished data, is the property of F. -

Study Protocol
Official Title: A Randomized, Multicenter, Double-Blind, Placebo-Controlled Phase II Study Of The Efficacy And Safety Of Trastuzumab Emtansine In Combination With Atezolizumab Or Atezolizumab- Placebo In Patients With HER2-Positive Locally Advanced Or Metastatic Breast Cancer Who Have Received Prior Trastuzumab And Taxane Based Therapy NCT Number: NCT02924883 Document Date: Protocol Version 3: 09 Aug 2017 PROTOCOL TITLE: A RANDOMIZED, MULTICENTER, DOUBLE-BLIND, PLACEBO-CONTROLLED PHASE II STUDY OF THE EFFICACY AND SAFETY OF TRASTUZUMAB EMTANSINE IN COMBINATION WITH ATEZOLIZUMAB OR ATEZOLIZUMAB-PLACEBO IN PATIENTS WITH HER2-POSITIVE LOCALLY ADVANCED OR METASTATIC BREAST CANCER WHO HAVE RECEIVED PRIOR TRASTUZUMAB AND TAXANE BASED THERAPY PROTOCOL NUMBER: WO30085 VERSION NUMBER: 3 EUDRACT NUMBER: 2015-004189-27 IND NUMBER: 71,072 TEST PRODUCT: Trastuzumab Emtansine (RO5304020) Atezolizumab (RO5541267) MEDICAL MONITOR: , M.D. , Ph.D. SPONSOR: F. Hoffmann-La Roche Ltd DATE FINAL: Version 1: 14 April 2016 DATE AMENDED: Version 2: 21 December 2016 Version 3: See electronic date stamp below. PROTOCOL AMENDMENT APPROVAL Approver's Name Title Date and Time (UTC) Company Signatory 09-Aug-2017 16:54:13 CONFIDENTIAL This clinical study is being sponsored globally by F. Hoffmann-La Roche Ltd of Basel, Switzerland. However, it may be implemented in individual countries by Roche’s local affiliates, including Genentech, Inc. in the United States. The information contained in this document, especially any unpublished data, is the property of F. Hoffmann-La Roche Ltd (or under its control) and therefore is provided to you in confidence as an investigator, potential investigator, or consultant, for review by you, your staff, and an applicable Ethics Committee or Institutional Review Board. -

Cyramza® (Ramucirumab)
Cyramza® (ramucirumab) (Intravenous) -E- Document Number: MODA-0405 Last Review Date: 07/01/2021 Date of Origin: 09/03/2019 Dates Reviewed: 09/2019, 10/2019, 01/2020, 04/2020, 07/2020, 10/2020, 01/2021, 04/2021, 07/2021 I. Length of Authorization Coverage will be provided for 6 months and may be renewed. II. Dosing Limits A. Quantity Limit (max daily dose) [NDC Unit]: • Cyramza 100 mg/10 mL: 4 vials per 14 days • Cyramza 500 mg/50 mL: 2 vials per 14 days B. Max Units (per dose and over time) [HCPCS Unit]: Gastric, Gastroesophageal, HCC, and Colorectal Cancer: • 180 billable units every 14 days NSCLC: • 240 billable units every 14 days III. Initial Approval Criteria 1 Coverage is provided in the following conditions: • Patient is at least 18 years of age; AND Universal Criteria 1 • Patient does not have uncontrolled severe hypertension; AND • Patient must not have had a surgical procedure within the preceding 28 days or have a surgical wound that has not fully healed; AND Gastric, Esophageal, and Gastro-esophageal Junction Adenocarcinoma † Ф 1-3,5-7,14,17,2e,5e • Used as subsequent therapy after fluoropyrimidine- or platinum-containing chemotherapy; AND • Used as a single agent OR in combination with paclitaxel; AND o Used for one of the following: Moda Health Plan, Inc. Medical Necessity Criteria Page 1/27 Proprietary & Confidential © 2021 Magellan Health, Inc. – Patient has unresectable locally advanced, recurrent, or metastatic disease; OR – Used as palliative therapy for locoregional disease in patients who are not surgical candidates -

1 Oncologic Drugs Advisory Committee (ODAC)
Oncologic Drugs Advisory Committee (ODAC) Meeting April, 27, 2021 BLA# 761034/Supplement 18 Drug name: TECENTRIQ® (atezolizumab) Applicant: Genentech, Inc. Combined FDA and Applicant ODAC Briefing Document Advisory Committee Briefing Materials: Available For Public Release 1 DISCLAIMER STATEMENT The attached package contains background information prepared by the Applicant and the Food and Drug Administration (FDA) for the panel members of the advisory committee. The package contains assessments and/or conclusions and recommendations written by individual FDA reviewers. Such conclusions and recommendations do not necessarily represent the final position of the individual reviewers, nor do they necessarily represent the final position of the Review Division or Office. We have brought the drug TECENTRIQ® (also known as atezolizumab) to this Advisory Committee in order to gain the Committee’s insights and opinions, and the background package may not include all issues relevant to the final regulatory recommendation and instead is intended to focus on issues identified by the Agency for discussion by the advisory committee. The FDA will not issue a final determination on the issues at hand until input from the advisory committee process has been considered and all reviews have been finalized. The final determination may be affected by issues not discussed at the advisory committee meeting. 2 Table of Contents Table of Tables ......................................................................................................................... -
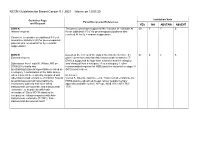
NCCN Guidelines for Breast Cancer V.1.2021 – Interim on 12/01/20
NCCN Guidelines for Breast Cancer V.1.2021 – Interim on 12/01/20 Guideline Page Institution Vote Panel Discussion/References and Request YES NO ABSTAIN ABSENT BINV-K The panel consensus supported the inclusion of “consider AI 20 4 1 6 Internal request: for an additional 3-5 y” for premenopausal patients who received AI for 5y + ovarian suppression. Comment to consider an additional 3-5 y of aromatase inhibitors (AI) for premenopausal patients who received AI for 5y + ovarian suppression? BINV-R Based on the review of the data in the noted reference, the 23 0 2 6 External request: panel consensus was that Ado-trastuzumab emtansine (T- DM1) is supported by high-level evidence and the category Submission from Linda W. Wilson, MD on was changed from a category 2A to a category 1, other 07/08/20 to clarify why recommended regimen for HER2-positive recurrent or stage IV tucatinib/trastuzumab/capecitabine is listed as (M1) breast cancer. a category 1 combination in the table above when it has not been directly compared with Reference: Ado-trastuzumab emtansine (T-DM1)? Should Verma S, Miles D, Gianni L, et al. Trastuzumab emtansine for tucatinib/trastuzumab/capecitabine be HER2-positive advanced breast cancer [supplementary reserved for patients that have failed appendix available online]. N Engl J Med 2012;367:1783- trastuzumab, pertuzumab, and trastuzumab 1791. emtansine, or in patients with brain metastases? Does NCCN stand by its category one rating compared with Ado- trastuzumab emtansine (T-DM1), Fam- trastuzumab deruxtecan-nxki? NCCN Guidelines for Breast Cancer V.1.2021 – Interim on 12/01/20 BINV-R Based on the FDA approval, and the data in the noted 18 2 5 6 Internal request: reference, the panel consensus was that atezolizumab + albumin-bound paclitaxel is supported by high-level evidence. -

Rituxan® (Rituximab)
Rituxan® (rituximab) (Intravenous) Document Number: IC-0109 Last Review Date: 03/04/2019 Date of Origin: 7/20/2010 Dates Reviewed: 09/2010, 12/2010, 02/2011, 03/2011, 05/2011, 06/2011, 09/2011, 12/2011, 03/2012, 06/2012, 09/2012, 12/2012, 03/2013, 06/2013, 09/2013, 12/2013, 03/2014, 06/2014, 09/2014, 12/2014, 03/2015, 05/2015, 08/2015, 11/2015, 02/2016, 05/2016, 08/2016, 10/2016, 02/2017, 05/2017, 08/2017, 10/2017, 02/2018, 05/2018, 07/2018, 09/2018, 12/2018, 03/2019 I. Length of Authorization Coverage will be provided for 6 months (12 months initially for pemphigus vulgaris) and may be renewed unless otherwise specified. Maintenance therapy for oncology indications (excluding ALL) may be renewed for up to a maximum of 2 years. Acute lymphoblastic leukemia (ALL) may not be renewed. Relapse therapy for pemphigus vulgaris must be at least 16 weeks past a prior infusion II. Dosing Limits A. Quantity Limit (max daily dose) [Pharmacy Benefit]: Rituxan 100 mg/10 mL injection: 12 vials per 28 day supply Rituxan 500 mg/50 mL injection: 8 vials per 28 day supply B. Max Units (per dose and over time) [Medical Benefit]: Oncology Indications Chronic Lymphocytic Leukemia (CLL)/Small Lymphocytic Leukemia (SLL): Initial therapy: o Loading dose: 100 units x 1 dose o Subsequent doses: 130 units every 28 days x 5 doses per 6 months Renewal therapy: 100 units per dose every 8 weeks x 4 doses per 6 months Immunotherapy Toxicity Treatment: 100 units per dose weekly x 4 doses in a 6 month period All other oncology indications: Initial therapy: 100 units per dose weekly x 8 doses per 6 months Renewal therapy: 100 units per dose every 8 weeks x 4 doses per 6 months Non-Oncology Indications Rheumatoid Arthritis (RA): 100 units per dose every 14 days x 2 doses in a 16 week period Proprietary & Confidential © 2019 Magellan Health, Inc. -

Genmab Announces That Janssen Will Stop Studies of Daratumumab in Combination with Anti-PD-(L)1
Genmab Announces that Janssen Will Stop Studies of Daratumumab in Combination with Anti-PD-(L)1 Company Announcement • Based on a recent planned review, the Data Monitoring Committee (DMC) recommends Phase Ib/II study of daratumumab plus atezolizumab (anti PD-L1 antibody) in patients with previously treated non-small cell lung cancer to be terminated. • Phase I MMY2036 study of daratumumab plus JNJ-63723283 (anti PD-1 antibody) in patients with multiple myeloma, discontinued • Health Authorities have been informed about these events and Janssen has contacted its partner companies conducting daratumumab and anti-PD-(L)1 combination studies to discuss ceasing enrollment and dosing of the combination while the data is being further investigated Copenhagen, Denmark; May 26, 2018 – Genmab A/S (Nasdaq Copenhagen: GEN) announced today that following a planned review, the DMC has recommended that the Phase Ib/II study (CALLISTO/LUC2001) of daratumumab in combination with atezolizumab versus atezolizumab monotherapy in patients with previously treated advanced or metastatic non-small cell lung cancer should be terminated. In addition the phase I MMY2036 study of daratumumab plus JNJ- 63723283, an anti PD-1 antibody in patients with multiple myeloma will be discontinued. The DMC determined that there was no observed benefit within the combination treatment arm, daratumumab plus atezolizumab, over atezolizumab monotherapy, and recommended termination of the study. In addition to the lack of benefit, the DMC noted a numerical increase in mortality-related events in the combination arm. Based on these findings, Janssen has made the decision also to discontinue the MMY2036 study, which was evaluating a combination of daratumumab and anti-PD-1 (JNJ-63723283) in patients with Multiple Myeloma.