Ocular Emergencies & Red
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Summary Benchmarks for Preferred Practice Pattern® Guidelines
SUMMARY BENCHMARKS FOR PREFERRED PRACTICE PATTERN® GUIDELINES TABLE OF CONTENTS Summary Benchmarks for Preferred Practice Pattern Guidelines Introduction . 1 Glaucoma Primary Open-Angle Glaucoma (Initial Evaluation) . 3 Primary Open-Angle Glaucoma (Follow-up Evaluation) . 5 Primary Open-Angle Glaucoma Suspect (Initial and Follow-up Evaluation) . 6 Primary Angle-Closure Disease (Initial Evaluation and Therapy) . 8 Retina Age-Related Macular Degeneration (Initial and Follow-up Evaluation) . 10 Age-Related Macular Degeneration (Management Recommendations) . 11 Diabetic Retinopathy (Initial and Follow-up Evaluation) . 12 Diabetic Retinopathy (Management Recommendations) . 13 Idiopathic Epiretinal Membrane and Vitreomacular Traction (Initial Evaluation and Therapy) . 14 Idiopathic Macular Hole (Initial Evaluation and Therapy) . 15 Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration (Initial and Follow-up Evaluation) . 17 Retinal and Ophthalmic Artery Occlusions (Initial Evaluation and Therapy) . 18 Retinal Vein Occlusions (Initial Evaluation and Therapy) . 19 Cataract/Anterior Segment Cataract (Initial and Follow-up Evaluation) . 20 Cornea/External Disease Bacterial Keratitis (Initial Evaluation) . 22 Bacterial Keratitis (Management Recommendations) . 23 Blepharitis (Initial and Follow-up Evaluation) . 24 Conjunctivitis (Initial Evaluation) . 25 Conjunctivitis (Management Recommendations) . 26 Corneal Ectasia (Initial Evaluation and Follow-up) . 27 Corneal Edema and Opacification (Initial Evaluation) . 28 Corneal Edema -

Repair of Open Globe Injury
Advances in Ophthalmology & Visual System Case Report Open Access Case report: repair of open globe injury Abstract Volume 3 Issue 1 - 2015 Globe rupture is a common sight-threatening ophthalmic emergency. We present a twelve-year-old girl with ocular trauma by sharp object resulting in corneal laceration, Nader Hussein Fouad Hassan Department of Ophthalmology, Benha University Hospital, hyphema, traumatic cataract and iris prolapse. This case illustrates the importance of early Egypt diagnosis, proper wound repair of ruptured globe as well as management of post-operative complications and value of early post-operative visual rehabilitation. Correspondence: Nader Hussein Fouad Hassan, Ophthalmology department, Benha University Hospital, Keywords: globe rupture, open globe injury, corneal laceration Kaliyobeya, Egypt, Tel +201224727982, Email Received: October 16, 2015 | Published: October 19, 2015 Abbreviations: FB, foreign body; VA, visual acuity; CT scan, patient then was given tetanus immunization, antiemetics, analgesics computerized tomography; RD, retinal detachment; INR, international and intravenous broad spectrum antibiotics and prepared for globe normalized ratio; GA, general anesthesia; D, diopter rupture repair under GA. Laboratory tests included a full blood count, liver function tests, INR, prothrombin time, partial thromboplastin Introduction time, kidney function tests, all were within normal. Ruptured Globe is a common ophthalmic emergency. It is a leading cause of blindness. Early examination with high level of suspicion is recommended in any patient with ocular trauma. Many signs may obscure detection of globe rupture, so the ophthalmologist should examine the patient thoroughly and treat the patient as early as impossible including early visual rehabilitation for young patients to prevent amblyopia. Globe rupture may be associated with traumatic hyphema, traumatic cataract, lens dislocation, vitreous hemorrhage, retinal detachment, uveal prolapse, scleral wound, orbital wall fractures, or optic nerve damage. -

Why Is This Important? Phone Triage) and Physical Exam
Goals Diagnostic Dilemmas Learn which features of the history and 1. What is the cause of this patient’s red eye? physical examination are most useful 2. Does this patient have a pathologic headache? Use risk scores and clinical decision tools 3. Does this patient have endocarditis? Distinguish benign from potentially serious 4. What is the cause of this patient’s back pain? conditions Identify clinical pearls and pitfalls What is the Cause of this Patient’s Mr. Ira Tatedi Red Eye? 32 year old man with one day h/o mild redness of OD, pain, and photophobia. Physical exam shows circumcorneal injection, and visual acuity is 20/80. Key Elements of History (including Why is this Important? Phone Triage) and Physical Exam Most cases of red eye are caused by viral History and Triage Physical Examination conjunctivitis, which does not generally Is vision affected? Visual acuity require any treatment Is there a foreign Pupil size/reactivity Some cases are caused by bacterial or allergic body sensation? Discharge conjunctivitis, for which specific treatment is Is there Pattern of redness indicated photophobia? Foreign body A minority of cases are caused by other Was there trauma? Hypopyon/hyphema conditions, which require urgent or emergent Are patient a contact referral to an ophthalmologist lens wearer? It is essential to be able to distinguish them Is there discharge from one another throughout the day? Anatomy/Differential Diagnosis Conjunctivitis Viral Conjunctivitis – Erythema with co-existing URI – Watery, serous discharge -

Multipurpose Conical Orbital Implant in Evisceration
Ophthalmic Plastic and Reconstructive Surgery Vol. 21, No. 5, pp 376–378 ©2005 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. Multipurpose Conical Orbital Implant in Evisceration Harry Marshak, M.D., and Steven C. Dresner, M.D. Doheny Eye Institute, Keck School of Medicine, University of Southern California, Los Angeles, California, U.S.A. Purpose: To evaluate the safety and efficacy of the porous polyethylene multipurpose conical orbital implant for use in evisceration. Methods: A retrospective review of 31 eyes that underwent evisceration and received the multipurpose conical orbital implant. The orbits were evaluated at 1 week, 1 month, and 6 months after final prosthetic fitting for implant exposure, superior sulcus deformity, and prosthetic motility. Results: There were no cases of extrusion, migration, or infection. All patients had a good cosmetic result after final prosthetic fitting. Prosthetic motility was good in all patients. Exposure developed in one eye (3%) and a superior sulcus deformity developed in one eye (3%). Conclusions: Placement of an multipurpose conical orbital implant in conjunction with evisceration is a safe and effective treatment for blind painful eye that achieves good motility and a good cosmetic result. visceration has proved to be effective for the treat- forms anteriorly to the sclera to be closed over it, without Ement of blind painful eye from phthisis bulbi or crowding the fornices, and extends posteriorly through endophthalmitis. By retaining the sclera in its anatomic the posterior sclerotomies, providing needed volume to natural position, evisceration has the advantage of allow- the posterior orbit. ing the insertions of the extraocular muscles to remain intact, promoting better motility. -

URGENT/EMERGENT When to Refer Financial Disclosure
URGENT/EMERGENT When to Refer Financial Disclosure Speaker, Amy Eston, M.D. has a financial interest/agreement or affiliation with Lansing Ophthalmology, where she is employed as a ophthalmologist. 58 yr old WF with 6 month history of decreased vision left eye. Ache behind the left eye for 2-3 months. Using husband’s contact lens solution made it feel better. Seen by two eye care professionals. Given glasses & told eye exam was normal. No past ocular history Medical history of depression Takes only aspirin and vitamins 20/20 OD 20/30 OS Eye Pressure 15 OD 16 OS – normal Dilated fundus exam & slit lamp were normal Pupillary exam was normal Extraocular movements were full Confrontation visual fields were full No red desaturation Color vision was slightly decreased but the same in both eyes Amsler grid testing was normal OCT disc – OD normal OS slight decreased RNFL OCT of the macula was normal Most common diagnoses: Dry Eye Optic Neuritis Treatment - copious amount of artificial tears. Return to recheck refraction Visual field testing Visual Field testing - Small defect in the right eye Large nasal defect in the left eye Visual Field - Right Hemianopsia. MRI which showed a subacute parietal and occipital lobe infarct. ANISOCORIA Size of the Pupil Constrictor muscles innervated by the Parasympathetic system & Dilating muscles innervated by the Sympathetic system The Sympathetic System Begins in the hypothalamus, travels through the brainstem. Then through the upper chest, up through the neck and to the eye. The Sympathetic System innervates Mueller’s muscle which helps to elevate the upper eyelid. -

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Peripapillary Retinal Vascular Involvement in Early Post-COVID-19 Patients
Journal of Clinical Medicine Article Peripapillary Retinal Vascular Involvement in Early Post-COVID-19 Patients 1,2, 1,2, 1,2, Alfonso Savastano y , Emanuele Crincoli y , Maria Cristina Savastano * , Saad Younis 3, Gloria Gambini 1,2, Umberto De Vico 1,2 , Grazia Maria Cozzupoli 1,2 , Carola Culiersi 1,2 , Stanislao Rizzo 1,2,4 and Gemelli Against COVID-19 Post-Acute Care Study Group 2 1 Ophthalmology Unit, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00196 Rome, Italy; [email protected] (A.S.); [email protected] (E.C.); [email protected] (G.G.); [email protected] (U.D.V.); [email protected] (G.M.C.); [email protected] (C.C.); [email protected] (S.R.) 2 Department of Ophthalmology, Catholic University of “Sacro Cuore”, 00168 Rome, Italy 3 Department of Ophthalmology, Western Eye Hospital, Imperial College Healthcare NHS Trust, London NW1 5QH, UK; [email protected] 4 Neuroscience Institute, Consiglio Nazionale delle Ricerche, Istituto di Neuroscienze, 56124 Pisa, Italy * Correspondence: [email protected]; Tel.: +39-063-015-4928 These authors contributed equally to this work. y Received: 5 August 2020; Accepted: 3 September 2020; Published: 8 September 2020 Abstract: The ability of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-20s) to cause multi-organ ischemia and coronavirus-induced posterior segment eye diseases in mammals gave concern about potential sight-threatening ischemia in post coronavirus disease 2019 patients. The radial peripapillary capillary plexus (RPCP) is a sensitive target due to the important role in the vascular supply of the peripapillary retinal nerve fiber layer (RNFL). -
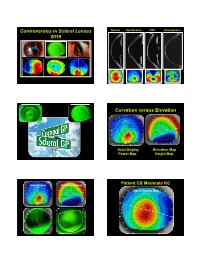
Controversies in Scleral Lenses 2019 Curvature Versus Elevation
Controversies in Scleral Lenses Normal Keratoconus PMD Keratoglobus 2019 Curvature versus Elevation Axial Display Elevation Map Power Map Height Map Axial Display Elevation Display Patient CB Moderate KC Axial Display Map +180um +180 +379 +379um Elevation Display -110 - 276 Elevation Map 655 Above the 290 microns Micron Sphere Height -276um Differential Depression Below the -110um Sphere N = 87 Patients 127 CL Fits Less than 350um Greater than 350um Patients with 350um or less of corneal elevation difference (along the greatest meridian of change) have an 88.2% chance of success with a corneal GP lens. The Re-Birth of Scleral Lenses Glass Scleral Lenses 1887 Molding Glass Scleral Lenses Average 8.5 High DK Scleral Materials Traditional Corneal / Scleral • Menicon Z Dk = 163 Shape • B & L, Boston XO2 DK = 141 • Contamac, Optimum Extreme DK = 125 • B & L, Boston XO DK = 100 • Paragon HDS 100 DK = 100 • Contamac, Optimum Extra DK = 100 • Lagado, Tyro -97 DK = 97 Scleral Shape Cone Angle Circa 1948 Klaus Pfortner New Understandings Argentina Scleral Lens Fitting Objectives Anatomy of a Scleral Lens 1. Central Vault Zone (250 to 400 microns) 2. Peripheral Lift Zone 4 3 2 1 2 3 4 3. Limbal Lift Zone 4. Scleral Landing Zone Ocular Surface Disease Scleral Lens Indications Scleral Irregular Astigmatism Lens • Keratoconus Indications • Pellucid Marginal Degeneration • Post Corneal Trauma • Post keratoplasty • Post K-Pro • Post Refractive Surgery RK, PRK and LASIK • Post HSV and HZV • Athletes • GP stability (rocking) issues Corneal Irregularity -

Treatment of Congenital Ptosis
13 Review Article Page 1 of 13 Treatment of congenital ptosis Vladimir Kratky1,2^ 1Department of Ophthalmology, Queen’s University, Kingston, Canada; 21st Medical Faculty, Charles University, Prague, Czech Republic Correspondence to: Vladimir Kratky, BSc, MD, FRCSC, DABO. Associate Professor of Ophthalmology, Director of Ophthalmic Plastic and Orbital Surgery, Oculoplastics Fellowship Director, Queen’s University, Kingston, Canada; 1st Medical Faculty, Charles University, Prague, Czech Republic. Email: [email protected]. Abstract: Congenital ptosis is an abnormally low position of the upper eyelid, with respect to the visual axis in the primary gaze. It can be present at birth or manifest itself during the first year of life and can be bilateral or unilateral. Additionally, it may be an isolated finding or part of a constellation of signs of a specific syndrome or systemic associations. Depending on how much it interferes with the visual axis, it may be considered as a functional or a cosmetic condition. In childhood, functional ptosis can lead to deprivation amblyopia and astigmatism and needs to be treated. However, even mild ptosis with normal vision can lead to psychosocial problems and correction is also advised, albeit on a less urgent basis. Although, patching and glasses can be prescribed to treat the amblyopia, the mainstay of management is surgical. There are several types of surgical procedure available depending on the severity and etiology of the droopy eyelid. The first part of this paper will review the different categories of congenital ptosis, including more common associated syndromes. The latter part will briefly cover the different surgical approaches, with emphasis on how to choose the correct condition. -

The Simplified Trachoma Grading System, Amended Anthony W Solomon,A Amir B Kello,B Mathieu Bangert,A Sheila K West,C Hugh R Taylor,D Rabebe Tekeraoie & Allen Fosterf
PolicyPolicy & practice & practice The simplified trachoma grading system, amended Anthony W Solomon,a Amir B Kello,b Mathieu Bangert,a Sheila K West,c Hugh R Taylor,d Rabebe Tekeraoie & Allen Fosterf Abstract A simplified grading system for trachoma was published by the World Health Organization (WHO) in 1987. Intended for use by non-specialist personnel working at community level, the system includes five signs, each of which can be present or absent in any eye: (i) trachomatous trichiasis; (ii) corneal opacity; (iii) trachomatous inflammation—follicular; (iv) trachomatous inflammation—intense; and (v) trachomatous scarring. Though neither perfectly sensitive nor perfectly specific for trachoma, these signs have been essential tools for identifying populations that need interventions to eliminate trachoma as a public health problem. In 2018, at WHO’s 4th global scientific meeting on trachoma, the definition of one of the signs, trachomatous trichiasis, was amended to exclude trichiasis that affects only the lower eyelid. This paper presents the amended system, updates its presentation, offers notes on its use and identifies areas of ongoing debate. Introduction (ii) corneal opacity; (iii) trachomatous inflammation—fol- licular; (iv) trachomatous inflammation—intense; and (v) tra- Trachoma is the most important infectious cause of blindness.1 chomatous scarring.19 Trachomatous inflammation—follicular Repeated conjunctival infection2 with particular strains of and trachomatous inflammation—intense are signs of active Chlamydia trachomatis3–5 -

Olivia Steinberg ICO Primary Care/Ocular Disease Resident American Academy of Optometry Residents Day Submission
Olivia Steinberg ICO Primary Care/Ocular Disease Resident American Academy of Optometry Residents Day Submission The use of oral doxycycline and vitamin C in the management of acute corneal hydrops: a case comparison Abstract- We compare two patients presenting to clinic with an uncommon complication of keratoconus, acute corneal hydrops. Management of the patients differs. One heals quickly, while the other has a delayed course to resolution. I. Case A a. Demographics: 40 yo AAM b. Case History i. CC: red eye, tearing, decreased VA x 1 day OS ii. POHx: (+) keratoconus OU iii. PMHx: depression, anxiety, asthma iv. Meds: Albuterol, Ziprasidone v. Scleral CL wearer for approximately 6 months OU vi. Denies any pain OS, denies previous occurrence OU, no complaints OD c. Pertinent Findings i. VA cc (CL’s)- 20/25 OD, 20/200 PH 20/60+2 OS ii. Slit Lamp 1. Inferior corneal thinning and Fleisher ring OD, central scarring OD, 2+ diffuse microcystic edema OS, Descemet’s break OS (photos and anterior segment OCT) 2. 2+ diffuse injection OS 3. D&Q A/C OU iii. Intraocular Pressures: deferred OD due to CL, 9mmHg OS (tonopen) iv. Fundus Exam- unremarkable OU II. Case B a. Demographics: 39 yo AAM b. Case History i. CC: painful, red eye, tearing, decreased VA x 1 day OS ii. POHx: unremarkable iii. PMHx: hypertension iv. Meds: unknown HTN medication v. Wears Soflens toric CL’s OU; reports previous doctor had difficulty achieving proper fit OU; denies diagnosis of keratoconus OU vi. Denies any injury OS, denies previous occurrence OU, no complaints OD c. -

Ophthalmic Management of Facial Nerve Palsy
Eye (2004) 18, 1225–1234 & 2004 Nature Publishing Group All rights reserved 0950-222X/04 $30.00 www.nature.com/eye 1 2 3 Ophthalmic V Lee , Z Currie and JRO Collin REVIEW management of facial nerve palsy Abstract The facial nerve travels with the eighth cranial nerve through the internal auditory canal and The ophthalmologist plays a pivotal role in the through the internal fallopian canal in the evaluation and rehabilitation of patients with petrous temporal bone for the longest facial nerve palsy. It is crucial to recognize and interosseus course of any cranial nerve (30 mm). treat the potentially life-threatening The fibres for the pterygopalatine ganglion underlying causes. The immediate ophthalmic leave at the geniculate ganglion as the greater priority is to ensure adequate corneal superficial petrosal nerve. The nerve to the protection. The medium to long-term stapedius and the chorda tympani (innervation management consists of treatment of epiphora, to the salivary glands) leave prior to the nerve hyperkinetic disorders secondary to aberrant exiting through the stylomastoid foramen as a regeneration and poor cosmesis. Patients purely motor nerve to the muscles of facial should be appropriately referred for general expression.2 Within the substance of the parotid 1 facial re-animation. This review aims to Central Eye Service gland, it divides into the five main Central Middlesex Hospital provide a guide to the management of this branchesFthe temporal, zygomatic, buccal, Acton Lane complex condition. Park Royal mandibular, and cervical branches. Facial nerve Eye (2004) 18, 1225–1234. doi:10.1038/sj.eye.6701383 Acton London, UK lesions above the geniculate ganglion classically Published online 16 April 2004 cause more severe ophthalmic symptoms 2Department of because lacrimal secretion and orbicularis Keywords: gold weight; tarsorrhapy; facial Ophthalmology closure are involved.