Iraq Rapid Response Deterioration of Protection and Human Rights Environment 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Iraq- Baghdad Governorate, Abu Ghraib District ( ( (
( ( ( ( ( ( ( ( Iraq- Baghdad Governorate, Abu Ghraib District ( ( ( ( ( ( Idressi Hay Al Askari - ( - 505 Turkey hoor Al basha IQ-P08985 Hamamiyat IQ-P08409 IQ-P08406 Mosul! ! ( ( Erbil ( Syria Iran Margiaba Samadah (( ( ( Baghdad IQ-P08422 ( IQ-P00173 Ramadi! ( ( !\ Al Hay Al Qaryat Askary ( Hadeb Al-Ru'ood Jordan Najaf! IQ-P08381 IQ-P00125 IQ-P00169 ( ( ( ( ( Basrah! ( Arba'at AsSharudi Arabia Kuwait Alef Alf (14000) Albu Khanfar Al Arba' IQ-P08390 IQ-P08398 ( Alaaf ( ( IQ-P00075 ( Al Gray'at ( ( IQ-P08374 ( ( 336 IQ-P08241 Al Sit Alaaf ( (6000) Sabi' Al ( Sabi Al Bur IQ-P08387 Bur (13000) - 12000 ( ( Hasan Sab'at ( IQ-P08438 IQ-P08437 al Laji Alaaf Sabi' Al ( IQ-P00131 IQ-P08435 Bur (5000) ( ( IQ-P08439 ( Hay Al ( ( ( Thaman Alaaf ( Mirad IQ-P08411 Kadhimia District ( as Suki Albu Khalifa اﻟﻛﺎظﻣﯾﺔ Al jdawil IQ-P08424 IQ-P00074 Albu Soda ( Albo Ugla ( (qnatir) ( IQ-P00081 village ( IQ-P00033 Al-Rufa ( IQ-D040 IQ-P00062 IQ-P00105 Anbar Governorate ( ( ( اﻻﻧﺑﺎر Shimran al Muslo ( IQ-G01 Al-Rubaidha IQ-P00174 Dayrat IQ-P00104 ar Rih ( IQ-P00120 Al Rashad Al-Karagul ( Albu Awsaj IQ-P00042 IQ-P00095 IQ-P00065 ( ( ( Albo Awdah Bani Zaid Al-Zuwayiah ( Ad Dulaimiya ( Albu Jasim IQ-P00060 Hay Al Halabsa - IQ-P00117 IQ-P00114 ( IQ-P00022 Falluja District ( ( ( - Karma Uroba Al karma ( Ibraheem ( IQ-P00072 Al-Khaleel اﻟﻔﻠوﺟﺔ Al Husaiwat IQ-P00139 IQ-P00127 ) ( ( Halabsa Al-Shurtan IQ-P00154 IQ-P00031 Karma - Al ( ( ( ( ( ( village IQ-P00110 Ash Shaykh Somod ( ( IQ-D002 IQ-P00277 Hasan as Suhayl ( IQ-P00156 subihat Ibrahim ( IQ-P08189 Muhammad -
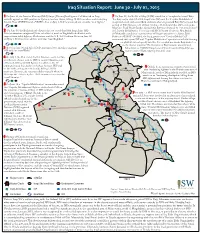
Iraq SITREP 2015-5-22
Iraq Situation Report: June 30 - July 01, 2015 1 On June 30, the Interior Ministry (MoI) Suqur [Falcons] Intelligence Cell directed an Iraqi 7 On June 29, Asa’ib Ahl al-Haq (AAH) stated that it “completely cleared” Baiji. airstrike against an ISIS position in Qa’im in western Anbar, killing 20 ISIS members and destroying e Baiji mayor stated that IA, Iraqi Police (IP), and the “Popular Mobilization” Suicide Vests (SVESTs) and a VBIED. Also on July 1, DoD announced one airstrike “near Qa’im.” recaptured south and central Baiji and were advancing toward Baiji Renery and had arrived at Albu Juwari, north of Baiji. On June 30, Federal Police (FP) commander Maj. Gen. Raed Shakir Jawdat claimed that Baiji was liberated by “our armed forces” 2 On June 30, the Baghdadi sub-district director stated that 16th Iraqi Army (IA) and Popular Mobilization Commission (PMC) Deputy Chairman Abu Mahdi Division members recaptured Jubba sub-district, north of Baghdadi sub-district, with al-Muhandis stated that “security forces will begin operations to cleanse Baiji support from tribal ghters, IA Aviation, and the U.S.-led Coalition. Between June 30 Renery of [ISIS].” On July 1, the Iraqi government “Combat Media Cell” and July 1, DoD announced four airstrikes “near Baghdadi.” announced that a joint ISF and “Popular Mobilization” operation retook the housing complex but did not specify whether the complex was inside Baiji district or Dahuk on the district outskirts. e liberation of Baiji remains unconrmed. 3 Between June 30 and July 1 DoD announced two airstrikes targeting Meanwhile an SVBIED targeted an IA tank near the Riyashiyah gas ISIS vehicles “near Walid.” Mosul Dam station south of Baiji, injuring the tank’s crew. -

Weekly Explosive Incidents Flas
iMMAP - Humanitarian Access Response Weekly Explosive Incidents Flash News (26 MAR - 01 APR 2020) 79 24 26 13 2 INCIDENTS PEOPLE KILLED PEOPLE INJURED EXPLOSIONS AIRSTRIKES DIYALA GOVERNORATE ISIS 31/MAR/2020 An Armed Group 26/MAR/2020 Injured a Military Forces member in Al-Ba'oda village in Tuz Khurmatu district. Four farmers injured in an armed conflict on the outskirts of the Mandali subdistrict. Iraqi Military Forces 01/APR/2020 ISIS 27/MAR/2020 Launched an airstrike destroying several ISIS hideouts in the Al-Mayta area, between Injured a Popular Mobilization Forces member in a clash in the Naft-Khana area. Diyala and Salah Al-Din border. Security Forces 28/MAR/2020 Found two ISIS hideouts and an IED in the orchards of Shekhi village in the Abi Saida ANBAR GOVERNORATE subdistrict. Popular Mobilization Forces 26/MAR/2020 An Armed Group 28/MAR/2020 Found an ISIS hideout containing fuel tanks used for transportation purposes in the Four missiles hit the Al-Shakhura area in Al-Barra subdistrict, northeast of Baqubah Nasmiya area, between Anbar and Salah Al-Din. district. Security Forces 30/MAR/2020 Popular Mobilization Forces 28/MAR/2020 Found and cleared a cache of explosives inside an ISIS hideout containing 46 homemade Bombarded a group of ISIS insurgents using mortar shells in the Banamel area on the IEDs, 27 gallons of C4, and three missiles in Al-Asriya village in Ramadi district. outskirts of Khanaqin district. ISIS 30/MAR/2020 Popular Mobilization Forces 28/MAR/2020 launched an attack killing a Popular Mobilization Forces member and injured two Security Found and cleared an IED in an agricultural area in the Hamrin lake vicinity, 59km northeast Forces members in Akashat area, west of Anbar. -
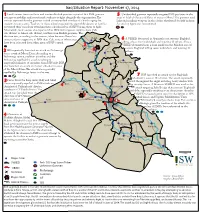
2014-11-17 Situation Report
Iraq Situation Report: November 17, 2014 1 Local sources from southern and western Kirkuk province reported that ISIS gunmen 5 Unidentied gunmen reportedly targeted ISIS positions in the attempt to mobilize and recruit male students to ght alongside the organization. e areas of Islah al-Zerai and Refai of western Mosul. e gunmen used sources reported that the gunmen visited an unspecied number of schools urging the light and medium weapons in the clashes that lasted for half an hour. students to carry arms. Teachers in these schools rejected this step while dozens of families A causality gure was not reported. prevented their sons from attending their schools in fear of ISIS forcing them to ght. Meanwhile, local sources also reported that ISIS shifted power supplies from Zab sub-district to Abassi sub-district, southwestern Kirkuk province. is decision was, according to the sources, taken because Abassi has Dahuk 6 more residents supportive of ISIS than Zab, some of whom may A VBIED detonated in Amiriyah area, western Baghdad, have been relocated from other areas of ISIS control. killing at least four individuals and injuring 13 others. Also, a Mosul2 Dam VBIED detonated near a local market in the Mashtal area of 2 5 eastern Baghdad killing seven individuals and injuring 22 ISIS reportedly launched an attack on Peshmerga Mosul Arbil others. forces south of Mosul Dam. According to a Peshmerga source, coalition airstrikes and the Peshmerga repelled the attack resulting in As Sulaymaniyah unspecied number of casualties from ISIS side. ISIS also launched an attack on Zumar sub-district, west Kirkuk of the Mosul Dam. -

Iraq Protection Cluster
Iraq Protection Cluster: Anbar Returnee Profile - March 2017 24 April 2017 Amiriyat Al- Protection Concerns Ramadi Heet Falluja/Garma Haditha Rutba Khaldiyah High Fallujah Reported Violations of principles relating to return movements (including non-discrimination in the right of return, as well as voluntariness, safety and dignity of return movements) Medium Security incidents resulting in death/injury in return area (including assault, murder, conflict-related casualties) Explosive Remnants of War (ERW)/ Improvised Explosive Device (IED) contamination in return area by District by Low Reported Rights violations by state or non-state military/security actors (including abduction, arbitrary arrest/detention, disproportionate restrictions on freedom of movement) Protection Risk Matrix Risk Protection Concerns relating to inter-communal relations and social cohesion MODM Returnee Figures Returnee Families (Registered and non-registered) District Families Falluja 53,218 Ramadi 82,242 Ramadi 51,293 Falluja/Garma 48,557 Ru'ua Heet 11,321 Heet 19,101 Haditha Haditha 3,936 Rutba 2,356 Ka'im Haditha 2,147 Heet 35,600 Baghdad 18,056 Rutba 1,825 Ana 31,299 Anbar 79,211 22,640 Anbar Displacements Erbil Ramadi 14,331 and Returns Falluja 13,341 Total Families Still Kirkuk 8,729 Displaced 12,472 Sulaymaniyah Total Families Rutba 6,500 Returned 4,440 Other 283 759 Babylon 474 IDP Information Center: 22% of calls received from Anbar were from returnees. The most popular issues flagged: 43% Governmental issues (grants, compensation on damaged properties, ..etc) 29% Cash assistance Data Sources: Disclaimer: 14% Other issues * IOM-DTM as of 30 March 2017 The boundaries and names shown and the designations used on this map * MoDM 18 April 2017 do not imply official endorsement or acceptance by the United Nations. -

Thi-Qar April 2014
IOM IRAQ GOVERNORATE PROFILE: THI-QAR APRIL 2014 KEY ISSUES FACING ANBAR CRISIS IDPS1 POPULATION FIGURES 4 60% of sites did not have adequate healthcare for 150 IDPs due to the Anbar 1,308 Iraqi returnees from Syria IDP women crisis2 20,560 IDPs post-20063 69,756 total returnees5 70% of sites where IDP children were not attending primary school 1.75 million total population6 of sites where IDPs did not have sufficient cash 60% RECENT DISPLACEMENT AND RETURNS IN THI-QAR7 75% of sites had IDPs living in rented houses Iraqi returnee families from Syria Al-Rifa’i 19 Families displaced 20% of sites where IDPs did not have 2 or more sets of due to Anbar Crisis clothing appropriate to the climate 0-168 Al-Shatra 169-803 OVERVIEW8 66 Thi-Qar, one of Iraq’s southernmost governorates, is a predominately 804-2091 Nassriya agricultural governorate that has seen a substantial wave of returnees from Suq al-Shuyokh Syria in recent months. As of the end of February, at least 260 families had 2092-7727 115 returned to Thi-Qar due to the conflict in Syria. Returnees, whether from 16 2 Syria or other countries, are considered a vulnerable population due to Al-Chibayish difficulties with the registration process and a very high unemployment 7728-16652 rate. Additionally, a small number of IDP families from Anbar have arrived to the governorate and are living in the Al-Shatra, Nassriya, and Suq al- Shuyokh districts. The number of informal settlements is growing in Thi- Sites identified as hosting Anbar IDPs Qar, as families are increasingly moving to government-owned lands. -

English Copy
IRAQ OPERATIONAL UPDATE JUNE 2016 In Iraq, the humanitarian situation continues to deteriorate, as people displaced from their homes by violence face their third summer living in harsh conditions. Meanwhile more people are being forced to flee their homes as a result of renewed fighting. The humanitarian crisis is being fuelled by the conflict in the region, and magnified by political instability and a severe economic crisis, which is further eroding Iraq’s fragile infrastructure and crumbling services, already weakened by years of violence. The number of people affected by the ongoing conflict continues to rise, with more than 3.3 million Iraqis now displaced throughout the country, causing an increasing strain on already destitute host communities. In addition to this, Iraqi Kurdistan is hosting a further 250,000 refugees who fled Syria from 2012 onwards. People’s humanitarian needs are most urgent in the areas outside Iraqi Kurdistan, but the international response in these areas is severely hampered by a very volatile security situation. In addition, state actors have mainly focused on carrying out military – rather than humanitarian – interventions, resulting in yet more people being displaced from densely populated areas. In those areas which have been retaken by Iraqi forces, including Tikrit, Diyala, Ramadi and parts of Ninewa governorate, displaced people are being encouraged to return to their homes. However, most towns and villages suffered high levels of destruction during the conflict and now basic services are only partially covered, while reconstruction is not yet underway. For displaced people living in unstable areas, often close to the frontlines, accessing healthcare is becoming increasingly difficult. -

Iraqi Red Crescent Organization
Iraqi Red Crescent Organization The Internally Displaced People in Iraq Update 30 27 January 2008 For additional information, please contact: In Iraq: 1. Iraqi Red Crescent Organization, President- Dr. Said Hakki, email: [email protected] 2. Iraqi Red Crescent Organization, Vice President- Dr. Jamal Karboli, email: [email protected] 3. International Relation Department manager [email protected]; Mobile phone: +964 7901669159; Telephone: +964 1 5372925/24/23 4. Disaster Management Department manager [email protected]; Mobile phone: +964 7703045043; Telephone: +964 1 5372925/24/23 In Jordan: Amman Coordination Office: [email protected]; Mobile phone (manager):+962 796484058; Mobile phone (deputy manager): +962 797180940 Also, visit the Iraqi Red Crescent Organization web site: iraqiredcrescent.org The Internally Displaced People in Iraq; update 30; 27 January 2008 Table of contents BACKGROUND..................................................................................................................................... 2 REFUGEES IN IRAQ................................................................................................................................ 2 RETURNEES FROM SYRIA ...................................................................................................................... 3 THE TURKISH BOMBARDMENT IN THE NORTH OF IRAQ .......................................................................... 3 THE INTERNALLY DISPLACED PEOPLE (IDP)........................................................................................ -

Highlights Situation Overview
Iraq: Humanitarian Crisis Situation Report No. 59 (26 August – 1 September 2015) This report is produced by OCHA Iraq in collaboration with humanitarian partners. Due to the dynamic situation, it is possible that the numbers and locations listed in this report may no longer be accurate. The next report will be issued on or around 11 September. Highlights IDPs in Kirkuk Governorate fear forced return to Diyala Governorate following Government announcement More than 71,000 IDPs return to Diyala in August despite ongoing insecurity; interagency mission to assess returnee needs on the ground Peshmerga advances result in close to 10,000 new IDPs in southwest Kirkuk Inter-cluster mission to Debaga undertaken; livelihood support and provision of services recommended Reference map. The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the UN. 8.6 m 5.6 m 3.2 m 2.9 m 3.2 m 0.25 m people in need targeted for internally displaced displaced people affected people in Syrian refugees assistance people live outside camps host communities Situation Overview Pressure is increasing on internally displaced persons (IDPs) in Kirkuk Governorate to return to their places of origin,particularly Diyala Governorate. According to the International Organization for Migration (IOM)’s Displacement Tracking Matrix (DTM), Kirkuk currently hosts 410,754 IDPs, or the fourth largest IDP population in the country after Anbar, Baghdad, and Dahuk governorates. This accounts for 13 per cent of Iraq’s 3.2 million displaced. Of the IDPs in Kirkuk, 142,740 individuals originate from Salah al-Din (35 per cent), followed by Anbar (126,396 IDPs/31 per cent), Kirkuk (80,238 IDPs/20 per cent), Ninewa (35,196 IDPs/9 per cent), as well as Diyala, Baghdad and Babylon governorates (combined total of 26,184 IDPs/6 per cent). -

Lead IG for Overseas Contingency Operations
LEAD INSPECTOR GENERAL FOR OVERSEAS CONTINGENCY OPERATIONS OPERATION INHERENT RESOLVE REPORT TO THE UNITED STATES CONGRESS OCTOBER 1, 2016‒DECEMBER 31, 2016 LEAD INSPECTOR GENERAL MISSION The Lead Inspector General for Overseas Contingency Operations will coordinate among the Inspectors General specified under the law to: • develop a joint strategic plan to conduct comprehensive oversight over all aspects of the contingency operation • ensure independent and effective oversight of all programs and operations of the federal government in support of the contingency operation through either joint or individual audits, inspections, and investigations • promote economy, efficiency, and effectiveness and prevent, detect, and deter fraud, waste, and abuse • perform analyses to ascertain the accuracy of information provided by federal agencies relating to obligations and expenditures, costs of programs and projects, accountability of funds, and the award and execution of major contracts, grants, and agreements • report quarterly and biannually to the Congress and the public on the contingency operation and activities of the Lead Inspector General (Pursuant to sections 2, 4, and 8L of the Inspector General Act of 1978) FOREWORD We are pleased to publish the Lead Inspector General (Lead IG) quarterly report on Operation Inherent Resolve (OIR). This is our eighth quarterly report on the overseas contingency operation (OCO), discharging our individual and collective agency oversight responsibilities pursuant to sections 2, 4, and 8L of the Inspector General Act of 1978. OIR is dedicated to countering the terrorist threat posed by the Islamic State of Iraq and the Levant (ISIL) in Iraq, Syria, the region, and the broader international community. The U.S. -
Protracted Displacement in Iraq: District of Origin Profiles
PROTRACTED DISPLACEMENT IN IRAQ: DISTRICT OF ORIGIN PROFILES AUGUST 2021 IOM IRAQ The opinions expressed in the report are those of the authors and do not necessarily reflect the views of the International Organization for Migration (IOM). The designations employed and the presentation of material throughout the report do not imply the expression of any opinion whatsoever on the part of IOM concerning the legal status of any country, territory, city or area, or of its authorities, or concerning its frontiers or boundaries. IOM is committed to the principle that humane and orderly migration benefits migrants and society. As an intergovernmental organization, IOM acts with its partners in the international community to: assist in meeting the operational challenges of migration; advance understanding of migration issues; encourage social and economic development through migration; and uphold the human dignity and well-being of migrants. The information contained in this report is for general information purposes only. Names and boundaries on DTM information products do not imply official endorsement or acceptance by IOM. The information in the DTM portal and in this report is the result of data collected by IOM field teams and complements information provided and generated by governmental and other entities in Iraq. IOM Iraq endeavors to keep this information as up to date and accurate as possible, but makes no claim —expressed or implied— on the completeness, accuracy and suitability of the information provided through this report. Challenges that should be taken into account when using DTM data in Iraq include the fluidity of the displaced population movements along with repeated emergencies and limited or no access to parts of the country. -

Iraq CRISIS Situation Report No. 49 (17 June – 23 June 2015)
Iraq CRISIS Situation Report No. 49 (17 June – 23 June 2015) This report is produced by OCHA Iraq in collaboration with humanitarian partners. It covers the period from 17 – 23 June. Due to the rapidly changing situation it is possible that the numbers and locations listed in this report may no longer be accurate. The next report will be issued on or around 3 July. Highlights More than 1,500 families return to Tikrit. Returnees need humanitarian assistance Close to 300,000 individuals displaced from Ramadi since 8 April NGOs respond to Sulaymaniyah checkpoint closures Concern over humanitarian conditions in Ameriyat al-Fallujah and Habbaniya Insufficient funding continues to limit humanitarian response capacity The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. Map created 25 June 2015. Situation Overview More than 1,500 families (approximately 9,000 individuals) returned to Tikrit City and surrounding areas between 14 and 23 June, after the area was retaken by Iraqi Security Forces in April, according to the Displacement Tracking Matrix (DTM) of the International Organization for Migration (IOM). Most of those who returned were Government civil servants who were requested to return. Approximately 80 per cent of Government employees have gone back to the area, local authorities report. Returnees reportedly were required to submit to ID checks, body and vehicle searches before being allowed through manned checkpoints. Authorities have reportedly dismantled 1,700 improvised explosive devices (IEDs) and cleared more than 200 booby-trapped houses. The recent returns brings the estimated total number of returnees in Tikrit District to 16,384 families (over 98,000 individuals), according to a partner NGO.