Acute and Short Term Hyperoxemia: How About Hemorheology And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HANDOUT #1 CONCEPT INTRODUCTION PRESENTATION: PERFUSION Topic Description Definition of Perfusion the Passage of Oxygenated Capi
HANDOUT #1 CONCEPT INTRODUCTION PRESENTATION: PERFUSION Topic Description Definition of Perfusion The passage of oxygenated capillary blood through body tissues. Peripheral perfusion is passage (flow) of blood to the extremities of the body. Central perfusion is passage (flow) of blood to major body organs, including the heart and lungs. Scope of Perfusion Perfusion can be viewed on a continuum as adequate on one end and inadequate, decreased, or impaired on the other. Decreased Perfusion can range from minimal to severe. Ischemia refers to decreased Perfusion, while infarction is complete tissue death due to severe decreased Perfusion. Risk Factors/Populations at Risk for Examples of risk factors or populations at risk Impaired Perfusion for impaired Perfusion can be categorized as modifiable (can be changed) and nonmodifiable (cannot be changed) Modifiable factors include: • Obesity • Lack of physical activity/sedentary lifestyle • Smoking Nonmodifiable factors include age, gender, and race/ethnicity. Groups at risk for impaired Perfusion include those who are of advanced age (due to less elastic arterial vessels as a result of aging) and those who are African American and Hispanic. These racial/ethnic groups are most at risk for chronic diseases that can affect Perfusion such as diabetes mellitus, hypertension, hyperlipidemia, and peripheral vascular disease. The cause of these variations is not known, but dietary and environmental factors may contribute to the higher incidence of chronic disease in these groups. Newborns and infants who have congenital heart anomalies are also at risk for impaired central Perfusion. Many of these defects can be surgically repaired to regain adequate Perfusion. Physiologic Consequences of Impaired Consequences of impaired Perfusion vary Perfusion depending on the degree of impairment. -

What Are the Health Effects from Exposure to Carbon Monoxide?
CO Lesson 2 CARBON MONOXIDE: LESSON TWO What are the Health Effects from Exposure to Carbon Monoxide? LESSON SUMMARY Carbon monoxide (CO) is an odorless, tasteless, colorless and nonirritating Grade Level: 9 – 12 gas that is impossible to detect by an exposed person. CO is produced by the Subject(s) Addressed: incomplete combustion of carbon-based fuels, including gas, wood, oil and Science, Biology coal. Exposure to CO is the leading cause of fatal poisonings in the United Class Time: 1 Period States and many other countries. When inhaled, CO is readily absorbed from the lungs into the bloodstream, where it binds tightly to hemoglobin in the Inquiry Category: Guided place of oxygen. CORE UNDERSTANDING/OBJECTIVES By the end of this lesson, students will have a basic understanding of the physiological mechanisms underlying CO toxicity. For specific learning and standards addressed, please see pages 30 and 31. MATERIALS INCORPORATION OF TECHNOLOGY Computer and/or projector with video capabilities INDIAN EDUCATION FOR ALL Fires utilizing carbon-based fuels, such as wood, produce carbon monoxide as a dangerous byproduct when the combustion is incomplete. Fire was important for the survival of early Native American tribes. The traditional teepees were well designed with sophisticated airflow patterns, enabling fires to be contained within the shelter while minimizing carbon monoxide exposure. However, fire was used for purposes other than just heat and cooking. According to the historian Henry Lewis, Native Americans used fire to aid in hunting, crop management, insect collection, warfare and many other activities. Today, fire is used to heat rocks used in sweat lodges. -

Oxygen Toxicity in Neonatal Rats: the Effect of Endotoxin Treatment on Survival During and Post-02 Exposure
0031-3998/87/2102-0 I 09$02.00/0 PEDIATRIC RESEARCH Vol. 21. No.2, 1987 Copyright© 1987 International Pediatric Research Foundation, Inc. Printed in U.S.A. Oxygen Toxicity in Neonatal Rats: The Effect of Endotoxin Treatment on Survival during and post-02 Exposure LEE FRANK Department ofMedicine, Pulmonary Research Labora10ry, University of Miami School of Medicine, Miami, Florida 33136 ABSTRACT. Neonatal rats were treated with low doses of monary 0 2 toxicity (I, 2). However, there are unique pulmonary bacterial lipopolysaccharide (endotoxin) to test for a pro complications associated with prolonged hyperoxic exposure in tective effect of endotoxin against 02 toxicity and the the neonatal animal which could importantly influence both severe inhibition of normal lung development which occurs short and long-term survival post-02 exposure. These complica during prolonged exposure to hyperoxia. The rationale for tions relate to the known inhibitory action of hyperoxia on lung the prophylactic use of endotoxin included its marked biosynthetic processes (1, 3, 4), and the morphological conse protective effect against pulmonary 0 2 toxicity in adult quences this inhibitory action has on the rapidly growing and rats and its lung growth-promoting effect in experimental differentiating newborn (animal) lung. Several studies have now pulmonary stress models. Neonatal rats (4-5 days old) demonstrated that early postnatal exposure to hyperoxia is as survived a 14-day exposure to >95% 0 2 equally well sociated with marked inhibition of the normal septation process whether treated with saline (39/51 = 76%) or with endo by which the large saccular airspaces characteristic of the new toxin (41/51 = 80%). -

Chronic Lung Disease (Bronchopulmonary Dysplasia)
Intensive Care Nursery House Staff Manual Chronic Lung Disease (Bronchopulmonary Dysplasia) was first described in 1967 as severe chronic lung disease (CLD) in preterm infants with severe Respiratory Distress Syndrome (RDS) who received treatment with 100% O2, high inspiratory ventilator pressures and no PEEP. With antenatal glucocorticoids, surfactant treatment and improved ventilatory techniques, CLD has almost disappeared in larger preterm infants and now affects very preterm infants with or without antecedent RDS. DEFINITION: CLD is defined as a need for increased oxygen: • Infants <32 weeks gestation: oxygen requirement at 36 weeks gestational age (GA) or at discharge (whichever comes first) • Infants ≥32 weeks GA: oxygen requirement at age >28 d or at discharge (whichever comes first) INCIDENCE of CLD is inversely related to birth weight and GA: Birth weight (g) Incidence of CLD* 501-750 34% *UCSF 1998-2002 751-1,000 20% 1,001-1,250 5% 1,251-1,500 3% PATHOLOGY includes areas of atelectasis and emphysema, hyperplasia of airway epithelium and interstitial edema. Late changes include interstitial fibrosis and hypertrophy of airway smooth muscle and pulmonary arteriolar musculature. ETIOLOGICAL FACTORS include: • Lung immaturity with (a) ↑ susceptibility to damage from oxygen, barotrauma and volutrauma, (b) surfactant deficiency and (c) immature antioxidant defenses. • Oxygen toxicity • Barotrauma and volutrauma • Pulmonary edema (excessive fluid administration, patent ductus arteriosus) • Inflammation (multiple associated biochemical -

Routine Adult Brain Perfusion
Adult Brain Perfusion CT Protocols Version 2.0 3/1/2016 DISCLAIMER: TO THE EXTENT ALLOWED BY LOCAL LAW, THIS INFORMATION IS PROVIDED TO YOU BY THE AMERICAN ASSOCIATION OF PHYSICISTS IN MEDICINE, A NON-PROFIT ORGANIZATION ORGANIZED TO PROMOTE THE APPLICATION OF PHYSICS TO MEDICINE AND BIOLOGY, ENCOURAGE INTEREST AND TRAINING IN MEDICAL PHYSICS AND RELATED FIELDS ("AAPM"), 'AS IS' WITHOUT WARRANTIES OR CONDITIONS OF ANY KIND, WHETHER ORAL OR WRITTEN, EXPRESS OR IMPLIED. AAPM SPECIFICALLY DISCLAIMS ANY IMPLIED WARRANTIES OR CONDITIONS OF MERCHANTABILITY, SATISFACTORY QUALITY, NONINFRINGEMENT AND FITNESS FOR A PARTICULAR PURPOSE. SOME JURISDICTIONS DO NOT ALLOW EXCLUSIONS OF IMPLIED WARRANTIES OR CONDITIONS, SO THE ABOVE EXCLUSION MAY NOT APPLY TO YOU. YOU MAY HAVE OTHER RIGHTS THAT VARY ACCORDING TO LOCAL LAW. TO THE EXTENT ALLOWED BY LOCAL LAW, IN NO EVENT WILL AAPM OR ITS SUBSIDIARIES, AFFILIATES OR VENDORS BE LIABLE FOR DIRECT, SPECIAL, INCIDENTAL, CONSEQUENTIAL OR OTHER DAMAGES (INCLUDING LOST PROFIT, LOST DATA, OR DOWNTIME COSTS), ARISING OUT OF THE USE, INABILITY TO USE, OR THE RESULTS OF USE OF THE PROVIDED INFORMATION, WHETHER BASED IN WARRANTY, CONTRACT, TORT OR OTHER LEGAL THEORY, AND WHETHER OR NOT ADVISED OF THE POSSIBILITY OF SUCH DAMAGES. YOUR USE OF THE INFORMATION IS ENTIRELY AT YOUR OWN RISK. THIS INFORMATION IS NOT MEANT TO BE USED AS A SUBSTITUTE FOR THE REVIEW OF SCAN PROTOCOL PARAMETERS BY A QUALIFIED AND CERTIFIED PROFESSIONAL. USERS ARE CAUTIONED TO SEEK THE ADVICE OF A QUALIFIED AND CERTIFIED PROFESSIONAL BEFORE USING ANY PROTOCOL BASED ON THE PROVIDED INFORMATION. AAPM IS NOT RESPONSIBLE FOR A USER'S FAILURE TO VERIFY OR CONFIRM APPROPRIATE PERFORMANCE OF THE PROVIDED SCAN PARAMETERS. -

MEDICAL STATEMENT Participant Record (Confidential Information) Please Read Carefully Before Signing
MEDICAL STATEMENT Participant Record (Confidential Information) Please read carefully before signing. This is a statement in which you are informed of some potential risks established safety procedures are not followed, however, there are involved in scuba diving and of the conduct required of you during the increased risks. scuba training program. Your signature on this statement is required for To scuba dive safely, you should not be extremely overweight or you to participate in the scuba training program offered out of condition. Diving can be strenuous under certain conditions. Your respiratory and circulatory systems must be in good health. All body air by_____________________________________________________and spaces must be normal and healthy. A person with coronary disease, a Instructor current cold or congestion, epilepsy, a severe medical problem or who is under the influence of alcohol or drugs should not dive. If you have _______________________________________________located in the asthma, heart disease, other chronic medical conditions or you are tak- Facility ing medications on a regular basis, you should consult your doctor and the instructor before participating in this program, and on a regular basis city of_______________________, state/province of _______________. thereafter upon completion. You will also learn from the instructor the important safety rules regarding breathing and equalization while scuba Read this statement prior to signing it. You must complete this diving. Improper use of scuba equipment can result in serious injury. You Medical Statement, which includes the medical questionnaire section, to must be thoroughly instructed in its use under direct supervision of a enroll in the scuba training program. If you are a minor, you must have qualified instructor to use it safely. -

Carbon Monoxide Poisoning: Neurologic Aspects by K K Jain MD (Dr
Carbon monoxide poisoning: neurologic aspects By K K Jain MD (Dr. Jain is a consultant in neurology and has no relevant financial relationships to disclose.) Originally released June 6, 1997; last updated April 5, 2016; expires April 5, 2019 Introduction This article includes discussion of carbon monoxide poisoning: neurologic aspects and CO poisoning. The foregoing terms may include synonyms, similar disorders, variations in usage, and abbreviations. Overview Carbon monoxide can produce several nonspecific symptoms and can mimic several diseases. Most of the signs and symptoms are due to hypoxia, which affects mainly the brain. The most significant neurologic and psychiatric manifestations of carbon monoxide poisoning are seen as subacute or late sequelae, often following a period of complete recovery from an acute episode. There is a possible interaction between nitric oxide, a ubiquitous molecule in the human body, and carbon monoxide. Carbon monoxide exposure initiates processes including oxidative stress that triggers activation of N-methyl-D-aspartate neuronal nitric oxide synthase, and these events are necessary for the progression of carbon monoxide–mediated neuropathology. The most important diagnostic test for carbon monoxide poisoning is the direct spectroscopic measurement of carboxyhemoglobin level in the blood. Brain imaging findings frequently correlate with clinical manifestations. Hyperbaric oxygen plays an important role in the management of carbon monoxide poisoning. Key points • Carbon monoxide poisoning can produce several nonspecific symptoms and can mimic several diseases. • Most of the effects are due to hypoxia. • Neurologic sequelae are significant and may be delayed in onset. • Hyperbaric oxygen plays an important role in management of carbon monoxide poisoning. -
Power Equation for Predicting the Risk of Central Nervous System Oxygen Toxicity at Rest
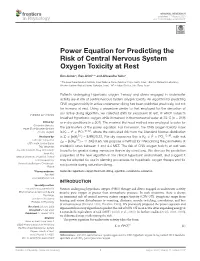
fphys-11-01007 August 17, 2020 Time: 14:44 # 1 ORIGINAL RESEARCH published: 17 August 2020 doi: 10.3389/fphys.2020.01007 Power Equation for Predicting the Risk of Central Nervous System Oxygen Toxicity at Rest Ben Aviner1, Ran Arieli1,2* and Alexandra Yalov3 1 The Israel Naval Medical Institute, Israel Defense Forces Medical Corps, Haifa, Israel, 2 Eliachar Research Laboratory, Western Galilee Medical Center, Nahariya, Israel, 3 HP – Indigo Division, Nes Ziona, Israel Patients undergoing hyperbaric oxygen therapy and divers engaged in underwater activity are at risk of central nervous system oxygen toxicity. An algorithm for predicting CNS oxygen toxicity in active underwater diving has been published previously, but not for humans at rest. Using a procedure similar to that employed for the derivation of our active diving algorithm, we collected data for exposures at rest, in which subjects breathed hyperbaric oxygen while immersed in thermoneutral water at 33◦C(n = 219) Edited by: or in dry conditions (n = 507). The maximal likelihood method was employed to solve for Costantino Balestra, Haute École Bruxelles-Brabant the parameters of the power equation. For immersion, the CNS oxygen toxicity index 2 10:93 (HE2B), Belgium is KI = t × PO2 , where the calculated risk from the Standard Normal distribution 0:5 2 12:99 Reviewed by: is ZI = [ln(KI ) – 8.99)]/0.81. For dry exposures this is KD = t × PO2 , with risk Enrico M. Camporesi, 0:5 ZD = [ln(KD ) – 11.34)]/0.65. We propose a method for interpolating the parameters at USF Health, United States Thijs Wingelaar, metabolic rates between 1 and 4.4 MET. -

FACTORS INFLUENCING CLINICAL OXYGEN TOXICITY John W. Bean
FACTORS INFLUENCING CLINICAL OXYGEN TOXICITY John W. Bean Department of Physiology, University of Michigan Ann Arbor, Mich. Introduction Since the early work of Priestley1 and Lavoisier? it has been recognized, though questioned by many,Ythat breathing increased concentrations of 02 may have adverse as well as therapeutic effects on animal organisms. The exact mechanism of causation of these adverse reactions-which for want of a better name have been referred to as those of O2 poisoning-is not known. But there are numerous factors which influence its occurrence and severity. If the clinical use of O2 in increased concentrations, especially at high pressure, is to achieve the success which it certainly seems to promise, recognition of its potential dangers and limitations, as well as knowledge of the more important factors which contribute to O2 toxicity, is imperative. Fundamental Factors Influencing 03Toxicity Fundamentally, the occurrence of this phenomenon is determined by: (1) an intensity factor, i.e., the O2 concentration and (2) a duration factor or length of exposure, and both of these depend on (3) the inconstant and frequently un- predictable susceptibility of the subject. Manifestation of O2 poisoning induced by increased concentrations of O2 at normal atmospheric pressure (OAP) and at higher pressures (OHP), i.e., partial pressures in excess of pure O2 at normal atmospheric pressure (hyperbaric 02)have many features in common, but in OHP there are additional manifestalions of CNS involvement not usually seen in OAP. Nevertheless, for brevity and convenience, here we shall draw no sharp line of demarcation. Pulnionnr>l Changes in 02Toxicity The first toxic effects of O2 to be observed were those noted by Priestley‘ and described by Lavoisier’ as an “incendiary” action on the lungs of animals breath- ing 02at atmospheric pressure. -

Oxygen Toxicity and Mitochondrial Metabolism
University of Louisville ThinkIR: The University of Louisville's Institutional Repository Electronic Theses and Dissertations 12-2003 Oxygen toxicity and mitochondrial metabolism. Jian Li 1974- University of Louisville Follow this and additional works at: https://ir.library.louisville.edu/etd Recommended Citation Li, Jian 1974-, "Oxygen toxicity and mitochondrial metabolism." (2003). Electronic Theses and Dissertations. Paper 822. https://doi.org/10.18297/etd/822 This Doctoral Dissertation is brought to you for free and open access by ThinkIR: The University of Louisville's Institutional Repository. It has been accepted for inclusion in Electronic Theses and Dissertations by an authorized administrator of ThinkIR: The University of Louisville's Institutional Repository. This title appears here courtesy of the author, who has retained all other copyrights. For more information, please contact [email protected]. OXYGEN TOXICITY AND MITOCHONDRIAL METABOLISM By Jian Li M.D., Tianjin Medical University, 1997 M.S., Peking Union Medical College, 2000 M.S., University of Louisville, 2002 A Dissertation Submitted to the Faculty of the Graduate School of the University of Louisville in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy Department of Pharmacology and Toxicology University of Louisville Louisville, Kentucky December 2003 OXYGEN TOXICITY AND MITOCHONDRIAL METABOLISM By Jian Li M.D., Tianjin Medical University, 1997 M.S., Peking Union Medical College, 2000 M.S., University of Louisville, 2002 A Dissertation Approved on November 14, 2003 by the following Dissertation Committee: ___________________________________ Dissertation Director ___________________________________ ___________________________________ ___________________________________ ___________________________________ ii ACKNOWLEDGEMENTS I wish to acknowledge Dr. John W. Eaton, for his valuable counsel and comprehensive leadership throughout this project. -
Oxygen Toxicity in the Neonate Q1 3
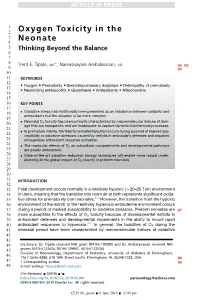
1 2 Oxygen Toxicity in the 3 4 Neonate 5 Thinking Beyond the Balance 6 7 8 Trent E. Tipple, MD*, Namasivayam Ambalavanan, MD Q2 Q3 9 Q4 10 11 KEYWORDS 12 Oxygen Prematurity Bronchopulmonary dysplasia Retinopathy of prematurity 13 14 Necrotizing enterocolitis Glutathione Antioxidants Mitochondria 15 16 KEY POINTS 17 18 Oxidative stress has traditionally been presented as an imbalance between oxidants and 19 antioxidants but the situation is far more complex. 20 Neonatal O2 toxicity has been primarily characterized by macromolecular indices of dam- 21 age that are nonspecific and are inadequate to capture dynamic biochemical processes. 22 In premature infants, the fetal to neonatal transition occurs during a period of marked sus- 23 ceptibility to oxidative stressors caused by deficits in antioxidant defenses and impaired endogenous antioxidant response activation. 24 The molecular effects of O on subcellular compartments and developmental pathways 25 2 are poorly understood. 26 State-of-the-art oxidation-reduction biology techniques will enable more robust under- 27 standing of the global impact of O2 toxicity in preterm neonates. 28 29 30 31 INTRODUCTION 32 33 Fetal development occurs normally in a relatively hypoxic (w20–25 Torr) environment 34 in utero, meaning that the transition into room air at birth represents significant oxida- 35 tive stress for prematurely born neonates.1,2 However, the transition from the hypoxic 36 environment of the womb to the relatively hyperoxic extrauterine environment occurs 37 during a period of marked susceptibility to oxidative stressors. Preterm neonates are Q7 38 more susceptible to the effects of O2 toxicity because of developmental deficits in 39 antioxidant defenses and developmental impairments in the ability to mount rapid 3–7 40 antioxidant responses to hyperoxia. -

Hemorheology: Ling Societies Focus E Flows of Biofluids
The News and Information Publication of The Society of Rheology Volume 73 Number 2 July 2004 Biorheology/ Hemorheology: ling Societies Focus e Flows of Biofluids Also Inside: Macosko Awarded Bingham Medal Denn Wraps up as JOR Editor Technical Program for Lubbock Executive Committee Table of Contents President Susan J. Muller Chris Macosko 2004 Vice President Bingham Medalist 4 Andrew M. Kraymk Macosko is recognized for his contributions to rheometry, reactive polymer processing, Secretary and more. A. Jeffrey Giacomin Treasurer End of an Era: Mort Denn Montgomery T. Shaw Steps Down as JOR Editor 6 Only the 7th editor in the history of the Editor Journal of Rheology, Mort Denn will Morton M. Denn complete his service in 2005. Past-President | William B. Rüssel Biofluid Rheology 8 Two societies provide a home for Members-at-Large rheologists interested in rheology of ;Wesley R. Burghardt blood and of other biofluids. Timothy R Lodge Lynn M. Walker Technical Program for Lubbock 2005 12 The 76th Annual Meeting of The Society of Rheology will take place in The Cover shows February 2005 in Lubbock, Texas USA an illustration of red blood cells flowing in an arteriol. The cells Rheology News 14 deform to orient themselves to ICR2004 next month; BSR publishes the streamlines to reduce flow Rheology Reviews 2004; other news resistance. The figure is from Schmid-Schönbein, H., Grunau, G. and Brauer, H. Exempla Society Business 16 hämorheologica 'Das strömende JOR editor search commences; Organ Blut', Albert-Roussel Minutes of the Spring ExecCom meeting; Pharma GmbH, Wiesbaden, Treasurer's Report for year-end 2003.