Revised Wells Denial Template
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

3843 Pocketguide 08.Qxd
INDEX INDEX 1 Contents in Detail 3 2 Mild Steel and Iron Powder Electrodes 27 3 Hydrogen Controlled Electrodes 39 4 Stainless Steel and Special Electrodes 55 5 Cobalarc Hardfacing Consumables 71 6 Gas Metal Arc Welding (MIG) Wires 103 7 Flux Cored Arc Welding (FCAW) Wires 127 8 Submerged Arc Wires and Fluxes 171 9 Gas and TIG Welding Consumables 179 10 Solders and Fluxes 211 11 Miscellaneous Products 223 12 Technical and Trade Information 227 Notice about CIGWELD’s Welding Consumables Pocket Guide (manual). The information in this Pocket Guide has been prepared as a reference only for use exclusively with the products identified in it. Each user should properly assess the information in the specific context of the intended application. Throughout this manual there are specific safety warnings. Disobeying or failing to heed these warnings can result, in some circumstances, in the unchecked emission of poisonous gases, or burns from explosion or electric shock. Although care has been taken in compiling this information, CIGWELD will not be liable for any direct, indirect, special or consequential damage (including damage resulting from its negligence), arising out of, or connected with the use of, or reliance on, this information except for liability imposed by legislation (including the Trade Practices Act), that cannot be excluded. CIGWELD does not make or give any express or implied warranties or representations except for those that are implied by legislation (including the Trade Practices Act), that cannot be excluded. Where the preceding paragraphs cannot legally operate, and to the extent permitted by law, CIGWELD’s liability for breach of any term or warranty implied by law is limited to and completely discharged at CIGWELD’s option, by either: a) replacement of the manual in hard copy form; b) payment of the cost of replacing the manual or acquiring an equivalent one. -

World Para Nordic Skiing Homologation Guide Version 2017
World Para Nordic Skiing Homologation Guide Version 2017 Homologation of courses for World Para Nordic Skiing (WPNS) (Para Cross Country Skiing and Para Biathlon for skiers with impairments) 1 General In general, the philosophy for FIS homologation, and the requirements and recommendations for stadium and course design applies to World Para Nordic Skiing as well. IBU requirements for stadium, range and course design are also applicable, particularly on IBU venues. See FIS Homologation manual for: - Philosophy of Homologation - Course Design Criteria - Design of courses - Stadium - Waxing cabins, Ski test area, warm up course - Practicing homologation skills However, since certain classes and categories have clear physical limitations, the courses must in general be made easier, with special attention to fast downhill sections, sharp curves, and steep or long up hills. The following sections will describe areas within homologation work that specifically should be considered when designing courses for Paralympic Nordic Skiing athletes. 2 Definitions 2.1 HD (height difference) is the difference in height between the lowest and highest points of a competition course. 2.2 MC (Maximum climb) is the climb with the highest partial height difference, in other terms, the biggest uphill. The uphill can be interrupted by a section of undulating terrain that does not exceed 200 m in length or a downhill that does not exceed 10 m PHD. 2.3 TC (Total climb) represents a total of all climbs on the course. World Para Nordic Skiing Homologation Guide ver 2017 1 3 Classification Paralympic Nordic Skiing athletes are classified according to the following table: Category Class Region Impairment Main sport equipment and degree of impairment Standing LW2 Impairments in one lower limb (ex. -

Framework for In-Field Analyses of Performance and Sub-Technique Selection in Standing Para Cross-Country Skiers
sensors Article Framework for In-Field Analyses of Performance and Sub-Technique Selection in Standing Para Cross-Country Skiers Camilla H. Carlsen 1,*, Julia Kathrin Baumgart 1, Jan Kocbach 1,2, Pål Haugnes 1 , Evy M. B. Paulussen 1,3 and Øyvind Sandbakk 1 1 Centre for Elite Sports Research, Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, 7491 Trondheim, Norway; [email protected] (J.K.B.); [email protected] (J.K.); [email protected] (P.H.); [email protected] (E.M.B.P.); [email protected] (Ø.S.) 2 NORCE Norwegian Research Centre AS, 5008 Bergen, Norway 3 Faculty of Health, Medicine & Life Sciences, Maastricht University, 6200 MD Maastricht, The Netherlands * Correspondence: [email protected]; Tel.: +47-452-40-788 Abstract: Our aims were to evaluate the feasibility of a framework based on micro-sensor technology for in-field analyses of performance and sub-technique selection in Para cross-country (XC) skiing by using it to compare these parameters between elite standing Para (two men; one woman) and able- bodied (AB) (three men; four women) XC skiers during a classical skiing race. The data from a global navigation satellite system and inertial measurement unit were integrated to compare time loss and selected sub-techniques as a function of speed. Compared to male/female AB skiers, male/female Para skiers displayed 19/14% slower average speed with the largest time loss (65 ± 36/35 ± 6 s/lap) Citation: Carlsen, C.H.; Kathrin found in uphill terrain. -
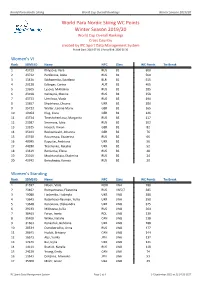
World Para Nordic Skiing WC Points Winter Season 2019/20
World Para Nordic Skiing World Cup Overall Rankings Winter Season 2019/20 World Para Nordic Skiing WC Points Winter Season 2019/20 World Cup Overall Rankings Cross Country created by IPC Sport Data Management System Period Start: 2019-07-01 | Period End: 2020-06-30 Women's VI Rank SDMS ID Name NPC Class WC Points Tie Break 1 43739 Khlyzova, Vera RUS B2 600 2 43732 Panferova, Anna RUS B2 560 3 13436 Sakhanenka, Sviatlana BLR B2 515 4 29128 Edlinger, Carina AUT B1 405 5 13605 Lysova, Mikhalina RUS B2 285 6 23918 Galitsyna, Marina RUS B1 258 7 43733 Umrilova, Vlada RUS B3 190 8 13657 Shyshkova, Oksana UKR B2 180 9 35723 Walter, Leonie Maria GER B2 165 10 19064 Klug, Clara GER B1 126 11 43734 Tereshchenkova, Margarita RUS B3 117 12 23987 Smirnova, Iuliia RUS B2 102 13 13525 Hoesch, Vivian GER B1 82 14 35103 Recktenwald, Johanna GER B2 76 15 43740 Razumnaia, Ekaterina RUS B2 66 16 40995 Kapustei, Andriana UKR B2 56 17 44280 Tkachenko, Nataliia UKR B2 52 18 13619 Remizova, Elena RUS B3 48 19 23919 Moshkovskaia, Ekaterina RUS B2 24 20 43742 Berezhnaia, Kseniia RUS B2 20 Women's Standing Rank SDMS ID Name NPC Class WC Points Tie Break 1 31597 Nilsen, Vilde NOR LW4 780 2 23402 Rumyantseva, Ekaterina RUS LW5/7 385 3 19080 Liashenko, Liudmyla UKR LW8 380 4 13643 Batenkova-Bauman, Yuliia UKR LW6 350 5 13648 Kononova, Oleksandra UKR LW8 325 6 29233 Mikheeva, Iuliia RUS LW8 264 7 30463 Faron, Iweta POL LW8 239 8 35400 Wilkie, Natalie CAN LW8 238 9 31663 Konashuk, Bohdana UKR LW8 188 10 20534 Ostroborodko, Anna RUS LW8 177 11 20641 Hudak, Brittany CAN -

THIRU. V. LOGANATHAN, BA, LLB, D.No . 659 / 2020 Dated 16.10
JUDICIAL MAGISTRATE COURT, TIRUTTANI PRESENT : THIRU. V. LOGANATHAN, B.A., L.L.B., D.No . 659 / 2020 Dated 16.10.2020 COVID19 ADVANCE SPECIAL CAUSE LIST, FOR 19.10.2020 (As per the OM. In D.No 5050/A/2020 dated 24.09.2020 of the Hon'ble Principal District Sessions Judge, Tiruvallur) S. Case No. Name of Parties Name of the counsel Date of Stage of the No Hearing case . 1. C.C.No.36/2017 SI of Police App for Prosecution 19.10.2020 Served Tiruttani P.S and summons of Vs Mr.V.Venkatesan Lw1, Lw4 to Babu Lw6 2. C.C.No.332/2013 Inspector of Police App for Prosecution 19.10.2020 Served Thiruvalangadu P.S and summons of Vs Mr.D.Nagaraj Lw12 & Sampathkumar Lw13 3. C.C.No.60/2015 Inspector of Police, App for Prosecution 19.10.2020 Served Thiruvalangadu P.S and summons of Vs Mr.V.Kishore Reddy Lw9 to Lw12 Narasimman (I.O) 4. C.C.2/2015 CCIW-CID App for Prosecution 19.10.2020 Served Tiruvallur and summons of Vs Mr.P.M.Narasimman Lw5 to Lw7 Rajendran 5. C.C.1/2015 CCIW-CID App for Prosecution 19.10.2020 Served Tiruvallur and summons of Vs Mr.P.M.Narasimman Lw5 to Lw7 Rajendran 6. C.C.No.40/2017 SI of Police, App for Prosecution 19.10.2020 Served DCB-Tiruvallur and summons of Vs Mr.V.Kishore Reddy Pw1 to Pw5 Venkatesan for chief continuation 7. C.C.No.224/2015 SI of police App for Prosecution 19.10.2020 Served Tiruttani P.S and summons to Vs Mr.R.Sivaraj Lw6 to Lw9 Parthiban 8. -

START LIST As of 11 DEC 2017
CROSS COUNTRY LONG DISTANCE START LIST As of 11 DEC 2017 NPC Sport Start IPCNS WC Bib Name Code Class % Time Points Points Remarks Women Long C,Sitting 1 IOVLEVA Mariia NPA LW12 100 10:00:30 82 2 GULIAEVA Irina NPA LW12 100 10:01:00 81 3 ZHANG Lei CHN LW12 100 10:01:30 38 4 ABDIKARIMOVA Akzhana NPA LW10.5 90 10:02:00 48 5 FEDOROVA Nadezhda NPA LW12 100 10:02:30 45 6 ZAINULLINA Marta NPA LW12 100 10:03:00 140 7 KOCHEROVA Natalia NPA LW12 100 10:03:30 55 8 dos SANTOS ROCHA Aline BRA LW11 94 10:04:00 339.52 31 9 BALTABAYEVA Zhanyl KAZ LW12 100 10:04:30 228.48 10 LEE Do Yeon KOR LW12 100 10:05:00 226.20 15 11 GRETSCH Kendall USA LW11.5 96 10:05:30 160.33 64 12 SEO Vo-Ra-Mi KOR LW10.5 90 10:06:00 131.27 38 13 NAN Yuyu CHN LW11 94 10:06:30 113.22 20 14 JIN Yawei CHN LW10 86 10:07:00 73.85 56 15 CHU Beibei CHN LW12 100 10:07:30 58.47 65 16 SKARSTEIN Birgit NOR LW11 94 10:08:00 26.12 110 17 MASTERS Oksana USA LW12 100 10:08:30 0.00 120 18 ESKAU Andrea (WL) GER LW11 94 10:09:00 1.71 200 Men Long C,Sitting 21 RIBERA Cristian BRA LW11 94 10:40:30 24 22 HUANG Feixiang CHN LW12 100 10:41:00 30 23 GANZEI Aleksandr NPA LW12 100 10:41:30 68 24 KADENOV Suyundyk KAZ LW12 100 10:42:00 25 ZHENG Peng CHN LW10 86 10:42:30 82 26 LIM Woo Geun KOR LW11 94 10:43:00 27 FURUBERG Arnt Christian SWE LW11.5 96 10:43:30 15 28 WAGNER Jeremy USA LW11.5 96 10:44:00 21 29 AMINOV Rustam NPA LW10 86 10:44:30 9 30 PETUSHKOV Roman NPA LW12 100 10:45:00 53 31 FRAZIER Eric USA LW11 94 10:45:30 32 DAVIDOVICH Aleksandr NPA LW12 100 10:46:00 125 33 ROCHA Fernando BRA LW11.5 96 10:46:30 -
Classification Information Sheet Para-Cross Country Skiing
Classification Information Sheet Para-Cross Country Skiing This information is intended to be a generic guide to classification for Para-Cross Country Skiing. The classification of athletes in this sport is performed by authorised classifiers according to the World Para Nordic Skiing classification rules. What is the classification process? Trained classifiers assess an athlete using the World Para Nordic Skiing classification rules to determine the following: 1. Does the athlete have an eligible impairment type? An athlete must have a permanent eligible impairment type and provide medical documentation detailing their diagnosis and health condition. 2. Does the athlete meet the minimum impairment criteria for the sport? Specific criteria applied to each sport to determine if a person’s impairment results in sufficient limitation in their sport. This is called the minimum impairment criteria. 3. What is the appropriate class to allocate the athlete for competition? Classes are detailed in the classification rules for the sport and a classifier determines the class an athlete will compete in. Which Paralympic impairment groups compete in Para-Cross Country Skiing? Athletes are required to have a permanent, eligible impairment and will be required to provide medical diagnostic information about their diagnosis and impairment. Eligible Impairment Type Examples of health conditions Vision Reduced or no vision in both eyes caused by damage to the eye structure, optical Impairment nerves/optic pathways, or visual cortex of the brain. Includes -

World Para Alpine Skiing EC Points Winter Season
World Para Alpine Skiing Europa Cup Overall Rankings Winter Season 2016/17 World Para Alpine Skiing EC Points Winter Season 2016/17 Europa Cup Overall Rankings created by IPC Sport Data Management System Period Start: 2016-07-01 | Period End: 2017-06-30 Women's VI Rank SDMS ID Name NPC Class EC Points Tie Break 1 24063 Goluza, Eva CRO B2 625 2 24071 Sana, Eleonor BEL B3 560 3 23842 Ristau, Noemi Ewa GER B2 430 4 12946 Perrine, Melissa AUS B2 400 5 20310 Dessart, Marie-Morgane BEL B3 270 6 13418 Umstead, Danelle USA B2 215 7 13140 Gallagher, Kelly GBR B3 100 8= 14237 Mannella, Staci USA B3 80 8= 16125 Yang, Jae Rim KOR B2 80 Women's Standing Rank SDMS ID Name NPC Class EC Points Tie Break 1 13086 Pueyo Marimon, Ursula ESP LW2 829 2 17261 Schmidt, Bigna SUI LW5/7-3 660 3 29162 Rieder, Anna-Maria GER LW9-1 600 4 13206 Corradini, Melania ITA LW6/8-1 440 5 13261 Jochemsen, Anna NED LW2 360 6 13162 Rothfuss, Andrea GER LW6/8-2 300 7 31624 Hondo, Ammi JPN LW6/8-2 260 8 17095 Chatel-Laley, Marie FRA LW9-2 215 9 22219 Perez de Juan, Barbara ESP LW4 210 10 20240 Turgeon, Frederique CAN LW2 141 11 26952 Pemble, Mel CAN LW9-2 125 12 22832 Jepsen, Mollie CAN LW6/8-2 80 13 13034 Schwartz, Melanie USA LW2 77 14 31418 Joechl, Eva-Maria AUT LW6/8-1 60 15 13351 Smarzova, Petra SVK LW6/8-2 40 Women's Sitting Rank SDMS ID Name NPC Class EC Points Tie Break 1 18077 Hagspiel, Ruth GER LW10-1 595 2 28882 Tuertscher, Heike AUT LW12-1 490 3 21797 van Bergen, Barbara NED LW11 460 4 12977 Loesch, Claudia AUT LW11 380 5 13163 Schaffelhuber, Anna GER LW10-2 260 6 -

IPC Alpine Skiing Classification Rules and Regulations
IPC Alpine Skiing Classification Rules and Regulations 05 December 2012 International Paralympic Committee Adenauerallee 212-214 Tel.+49 228 2097-200 www.paralympic.org 53113 Bonn, Germany Fax+49 228 2097-209 [email protected] Content 1 INTRODUCTION TO CLASSIFICATION ..................................................................................................... 4 1.1 GOVERNANCE ........................................................................................................................................................... 4 1.2 STRUCTURE OF CLASSIFICATION REGULATIONS .................................................................................................................. 4 1.3 PURPOSE OF CLASSIFICATION REGULATIONS ..................................................................................................................... 4 1.4 IPC CLASSIFICATION CODE ........................................................................................................................................... 5 1.5 DEFINITIONS ............................................................................................................................................................. 5 2 CLASSIFIERS .......................................................................................................................................... 5 2.1 CLASSIFICATION PERSONNEL ......................................................................................................................................... 5 2.2 CLASSIFIERS – LEVELS -

World Para Alpine Skiing Rankings Rankings June 2017
World Para Alpine Skiing Rankings Rankings June 2017 World Para Alpine Skiing Rankings Rankings June 2017 created by IPC Sport Data Management System Gender: Men | Period Start: 2016-03-01 | Period End: 2017-06-01 Slalom Races Code Race Code Race Code Race 1 WPAS-20170402-GBR-SL 17 WPAS-20170208-KOR-SL 33 EC-20161117-NED-SL 2 WPAS-20170402-SUI-SL 18 WPAS-20170205-USA-SL 34 WPAS-20161116-NED-SL 3 WPAS-20170331-USA-SL 19 WCH-20170131-ITA-SL 35 WPAS-20161115-NED-SL 4 EC-20170331-SUI-SL 20 WC-20170120-SLO-SL 36 WPAS-20160403-ITA-SL 5 WPAS-20170331-CAN-SL 21 WC-20170119-SLO-SL 37 WPAS-20160327-CAN-SL 6 WPAS-20170326-AUT-SL 22 EC-20170109-SUI-SL 38 WPAS-20160327-CAN-SL 7 WPAS-20170326-FRA-SL 23 WPAS-20170107-AUT-SL 39 WPAS-20160326-FRA-SL 8 WPAS-20170325-ITA-SL 24 WPAS-20170106-AUT-SL 40 WPAS-20160324-USA-SL 9 WC-20170318-KOR-SL 25 WPAS-20170104-USA-SL 41 WPAS-20160324-FRA-SL 10 WPAS-20170305-CZE-SL 26 WC-20161222-SUI-SL 42 WPAS-20160323-USA-SL 11 WPAS-20170218-AUT-SL 27 WC-20161221-SUI-SL 43 AS-20160321-JPN-SL 12 EC-20170216-CRO-SL 28 WC-20161215-AUT-SL 44 AS-20160320-JPN-SL 13 EC-20170215-CRO-SL 29 WPAS-20161211-GER-SL 45 WPAS-20160320-SUI-SL 14 WPAS-20170210-USA-SL 30 WPAS-20161202-USA-SL 46 WPAS-20160312-AUT-SL 15 WPAS-20170209-KOR-SL 31 WPAS-20161201-USA-SL 47 AS-20160310-KOR-SL 16 WPAS-20170209-USA-SL 32 EC-20161118-NED-SL Men's Slalom VI Rank SDMS ID Name NPC Class WPAS Points Races 1 20881 Bertagnolli, Giacomo ITA B3 1.25 21 / 26 2 13335 Haraus, Miroslav SVK B2 5.72 20 / 26 3 13078 Santacana Maiztegui, Yon ESP B2 13.70 19 / 27 4 14863 -

World Para Alpine Skiing Rules and Regulations
World Para Alpine Skiing Rules and Regulations 2018/2019 August 2018 World Para Alpine Skiing Rules and Regulations For Alpine Skiing: Downhill, Super-G, Super Combined, Giant Slalom, Slalom, & Team Events 2018-2019 Season – valid until 1 October 2019 World Para Alpine Skiing Rules and Regulations: Competition Season 2018-2019 1 Contents Section 1: Regulations 300 Joint Regulations for World Para Alpine Skiing (WPAS) 301 WPAS Competitions 302 World Cup (Level 0) and Europa Cup, NORAM (Level 1) Point System, Rankings and Trophies 303 World Para Alpine Skiing Calendar 304 World Para Alpine Skiing Race Licence (WPAS Licence) 305 Race Licence Pre-requisites 306 Competitor’s Obligations and Rights 307 Sponsorships and Advertising 308 Display of Competition Equipment 309 Organisation of Competition 310 Invitation/Programme 311 Competition Administration and Fee Regulations (Athletes and Organising Committees) 312 Competition Entries 313 Team Captains’ Meetings 314 Draw 315 Start List / Publication of Results 316 Competitor Medical Examinations and Compliance with the IPC Anti-Doping Code 317 Medical Services Required from Event Organisers 318 Competition Equipment 319 Equipment Controls 320 Gambling and Competitions 321 Sanctions 322 Procedural Guidelines 323 Protests 324 Place of Submission World Para Alpine Skiing Rules and Regulations: Competition Season 2018-2019 2 325 Deadlines for Submission 326 Form of Protests 327 Protest Fees 328 Authorisation 329 Settlement of Protests by the Jury 330 Appeals Section 2: Rules Common to All Alpine Skiing -
National Officials Program LEVEL 1 Alpine, Para Alpine, Ski Cross
National Officials Program LEVEL 1 Alpine, Para Alpine, Ski Cross Updated: November 2015 FACILITATOR: ( Insert Name ) INTRODUCTION • Name: • Club: • Child’s Race Category: • Your involvement with Racing: – Racer – Official • Why are you taking this course? • Expectations of this course? OBJECTIVES OBJECTIVES • Hierarchy of Alpine Sanctioning Bodies • Canadian Officials Program • The Race Course • Race Organization • Race Officials & Their Functions • Timing • Gate Judging & Correct Passage • Course Crew & Safety set-up OVERVIEW • Sanctioning Bodies • Competitive Racing Levels • Officials’ Program OVERVIEW ALPINE INTERNATIONAL SKI FEDERATION • World governing body • Rules and Standards, sanctions, penalties • World Cup • World Championships • Continental Cups • Olympic Winter Games with/for IOC • www.fis-ski.com NSO – Alpine Canada Alpin • National Sports Organization - ACA • National governing body - Alpine, Para-alpine, Ski Cross • National Ski Teams • National Championships • Rules and Standards, sanctions, penalties (FIS compliant and ACA) • Leadership for sport development at national level (racing, coaching, officiating) • www.alpinecanada.org PTSO Provincial Territorial Sports Organizations: • Provincial governing body • Provincial Ski Teams • Provincial Championships • Rules and Standards, sanctions, penalties (FIS & ACA compliant and ‘local’) • Leadership for sport development at provincial level (racing, coaching, officiating) DIVISIONS / ZONES • Local governing body • Local Teams • Rules and Standards, sanctions, penalties (FIS, ACA and PSO compliant) • Leadership for sport development at local level (racing, coaching, officiating) RACING LEVELS • Non-Points Races . All age groups, calendared by divisions with PSO • Club specific ‘house-league’ and ‘fun-n-glory’ programs usually are not under PSO sanction • National Points Races . U14 and older, calendared at ACA by PSO . Competitive stream to qualify for provincial and national championships • FIS Races . U18 and older, calendared at FIS by ACA .