Carcinogenesis: the Cancer Cell–Mast Cell Connection
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tasmanian Devils' Transmissible Cancer
Tasmanian devils’ transmissible cancer: Izarbe Aísa Marín Genetics Bachelor’s Degree What is the future? Final Project | June 2017 Introduction Devil Facial Tumor Disease 1Why is Tasmanian devils’ cancer incidence so high? 2Introduction to transmissible cancers Carcinogenesis is thought to occur via Peto’s Paradox represents the lack of accumulation of mutations and mutation correlation between cancer prevalence rates depend on cell number, which and body size or lifespan and it can be Primary Mode of Lack of Capacity for correlates with body size and lifespan. useful to explore cases that are far tumor’s origin transmission allorecognition infinite growth Then, large and long-lived animals from what is expected. Tasmanian should have more cancers than smaller devils suffer from Devil Facial Tumor and shorter-lived ones, due to increased Disease (DFTD), a lethal transmissible The ancestral type of DTDF is thought to be derived from a Schwann cell (clonal number of cell divisions. cancer that is threatening the species origin) and it is transmitted by biting during mating or feeding interactions. to extinction. (2) (1) y = 0,0815 - 0,0061x [y=%Tumors; x=Log(Mass[x]*LifeSpan[y])] 10x DFTD was first reported in Mount William National Park, northeastern Tasmania, in 1996. In 20 years, the disease has spread to more than 85% Forestier of wild Tasmanian devil Peninsula populations, causing severe declines. Immunology of DFTD 3Why devils immune system do not recognize DFTD? (3) Deficiency of devil Marsupials’ immune system is different immune system from, rather than inferior to mammals’ immune system. Immunological Low genetic Slower immune responses tolerance diversity facilitate early transmission events. -
Principles of Cancer Prevention and Will Emphasize the Scientific Underpinnings of This Emerging Discipline
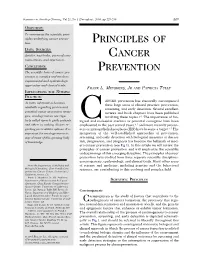
Seminars in Oncology Nursing, Vol 21, No 4 (November), 2005: pp 229-235 229 OBJECTIVE: To summarize the scientific prin- ciples underlying cancer preven- tion. PRINCIPLES OF DATA SOURCES: Articles, text books, personal com- CANCER munications, and experience. CONCLUSION: PREVENTION The scientific basis of cancer pre- vention is complex and involves experimental and epidemiologic approaches and clinical trials. FRANK L. MEYSKENS,JR AND PATRICIA TULLY IMPLICATIONS FOR NURSING PRACTICE: ANCER prevention has classically encompassed As more information becomes three large areas of clinical practice: prevention, available regarding proven and screening, and early detection. Several excellent potential cancer-prevention strate- reviews and book chapters have been published gies, oncology nurses are regu- involving these topics.1-3 The importance of bio- larly called upon to guide patients Clogical and molecular markers as potential surrogates have been and others in making choices re- emphasized in the past several years,4,5 and more recently precan- garding preventative options. It is cers or intraepithelial neoplasia (IEN) have become a target.6,7 The important for oncology nurses to integration of the well-established approaches of prevention, stay abreast of this growing body screening, and early detection with biological measures of disease of knowledge. risk, progression, and prognosis has become the hallmark of mod- ern cancer prevention (see Fig 1). In this article we will review the principles of cancer prevention and will emphasize the scientific underpinnings of this emerging discipline. The principles of cancer prevention have evolved from three separate scientific disciplines: carcinogenesis, epidemiology, and clinical trials. Many other areas From the Department of Medicine and of science and medicine, including genetics and the behavioral Biological Chemistry, Chao Family Com- sciences, are contributing to this evolving and complex field. -

Carcinogenesis
Chapter 3 Chapter 3 Carcinogenesis CONTENTS Oral Carcinoma and Smokeless Tobacco Use: A Clinical Profile W. Frederick McGuirt and Anna Wray .................................................. 91 Introduction .................................................................................... 91 Patients ............................................................................................ 91 Field Cancerization ......................................................................... 92 Discussion........................................................................................ 93 References ........................................................................................ 95 Chemical Composition of Smokeless Tobacco Products Klaus D. Brunnemann and Dietrich Hoffmann ..................................... 96 Introduction .................................................................................... 96 Chemical Composition ................................................................... 97 Carcinogenic Agents in ST .............................................................. 97 Carcinogenic N-Nitrosamines ....................................................... 100 TSNA .............................................................................................. 101 Control of Carcinogens in ST ....................................................... 104 References ...................................................................................... 106 Carcinogenesis of Smokeless Tobacco Dietrich Hoffmann, Abraham -

Mitochondrial Metabolism in Carcinogenesis and Cancer Therapy
cancers Review Mitochondrial Metabolism in Carcinogenesis and Cancer Therapy Hadia Moindjie 1,2, Sylvie Rodrigues-Ferreira 1,2,3 and Clara Nahmias 1,2,* 1 Inserm, Institut Gustave Roussy, UMR981 Biomarqueurs Prédictifs et Nouvelles Stratégies Thérapeutiques en Oncologie, 94800 Villejuif, France; [email protected] (H.M.); [email protected] (S.R.-F.) 2 LabEx LERMIT, Université Paris-Saclay, 92296 Châtenay-Malabry, France 3 Inovarion SAS, 75005 Paris, France * Correspondence: [email protected]; Tel.: +33-142-113-885 Simple Summary: Reprogramming metabolism is a hallmark of cancer. Warburg’s effect, defined as increased aerobic glycolysis at the expense of mitochondrial respiration in cancer cells, opened new avenues of research in the field of cancer. Later findings, however, have revealed that mitochondria remain functional and that they actively contribute to metabolic plasticity of cancer cells. Understand- ing the mechanisms by which mitochondrial metabolism controls tumor initiation and progression is necessary to better characterize the onset of carcinogenesis. These studies may ultimately lead to the design of novel anti-cancer strategies targeting mitochondrial functions. Abstract: Carcinogenesis is a multi-step process that refers to transformation of a normal cell into a tumoral neoplastic cell. The mechanisms that promote tumor initiation, promotion and progression are varied, complex and remain to be understood. Studies have highlighted the involvement of onco- genic mutations, genomic instability and epigenetic alterations as well as metabolic reprogramming, Citation: Moindjie, H.; in different processes of oncogenesis. However, the underlying mechanisms still have to be clarified. Rodrigues-Ferreira, S.; Nahmias, C. Mitochondria are central organelles at the crossroad of various energetic metabolisms. -

Cancer Biology Introduction Proto-Oncogenes Tumor
Introduction • Tissue homeostasis depends on the regulated cell division and self-elimination (programmed cell Cancer Biology death) of each of its constituent members except its stem cells • A tumor arises as a result of uncontrolled cell division and failure for self-elimination Chapter 18 • Alterations in three groups of genes are responsible Eric J. Hall., Amato Giaccia, for the deregulated control mechanisms that are the hallmarks of cancer cells: proto-oncogenes, tumor- Radiobiology for the Radiologist supressor genes, and DNA stability genes Proto-oncogenes Tumor-suppressor genes • Proto-oncogenes are components of signaling • Tumor-suppressor genes are also components of networks that act as positive growth the same signaling networks as proto-oncogenes, except that they act as negative growth regulators regulators in response to mitogens, cytokines, • They modulate proliferation and survival by and cell-to-cell contact antagonizing the biochemical functions of proto- • A gain-of-function mutation in only one copy oncogenes or responding to unchecked growth signals of a protooncogene results in a dominantly • In contrast to oncogenes, inactivation of both acting oncogene that often fails to respond to copies of tumor-suppressor genes is required for extracellular signals loss of function in most cases DNA stability genes Mechanisms of carcinogenesis • DNA stability genes form a class of genes • A single genetic alteration that leads to the involved in both monitoring and activation of an oncogene or loss of a tumor maintaining -

A Guide to Cancer Immunotherapy: from T Cell Basic Science to Clinical Practice
REVIEWS A guide to cancer immunotherapy: from T cell basic science to clinical practice Alex D. Waldman 1,2, Jill M. Fritz1,2 and Michael J. Lenardo 1,2 ✉ Abstract | The T lymphocyte, especially its capacity for antigen-directed cytotoxicity, has become a central focus for engaging the immune system in the fight against cancer. Basic science discoveries elucidating the molecular and cellular biology of the T cell have led to new strategies in this fight, including checkpoint blockade, adoptive cellular therapy and cancer vaccinology. This area of immunological research has been highly active for the past 50 years and is now enjoying unprecedented bench-to-bedside clinical success. Here, we provide a comprehensive historical and biological perspective regarding the advent and clinical implementation of cancer immunotherapeutics, with an emphasis on the fundamental importance of T lymphocyte regulation. We highlight clinical trials that demonstrate therapeutic efficacy and toxicities associated with each class of drug. Finally, we summarize emerging therapies and emphasize the yet to be elucidated questions and future promise within the field of cancer immunotherapy. Neoantigens The idea to deploy the immune system as a tool to treat system to prevent carcinogenesis in a manner similar to 1 1 Antigens not expressed by neoplastic disease originated in the nineteenth century . graft rejection . Productive immune responses following self-tissues under normal Wilhelm Busch and Friedrich Fehleisen were the first tumoural adoptive transfer in mice4 and clinical reports conditions that manifest in to describe an epidemiological association between of spontaneous regression of melanoma in patients with the context of pathology; in 5 cancer, these could be altered immune status and cancer. -

Guidelines for Carcinogen Risk Assessment
EPA/630/P-03/001B March 2005 Guidelines for Carcinogen Risk Assessment Risk Assessment Forum U.S. Environmental Protection Agency Washington, DC DISCLAIMER Mention of trade names or commercial products does not constitute endorsement or recommendation for use. CONTENTS 1. INTRODUCTION ........................................................ 1-1 1.1. PURPOSE AND SCOPE OF THE GUIDELINES ........................ 1-1 1.2. ORGANIZATION AND APPLICATION OF THE GUIDELINES ........... 1-3 1.2.1. Organization .............................................. 1-3 1.2.2. Application ............................................... 1-5 1.3. KEY FEATURES OF THE CANCER GUIDELINES ..................... 1-7 1.3.1. Critical Analysis of Available Information as the Starting Point for Evaluation ............................................... 1-7 1.3.2. Mode of Action ........................................... 1-10 1.3.3. Weight of Evidence Narrative ............................... 1-11 1.3.4. Dose-response Assessment .................................. 1-12 1.3.5. Susceptible Populations and Lifestages ........................ 1-13 1.3.6. Evaluating Risks from Childhood Exposures .................... 1-15 1.3.7. Emphasis on Characterization ............................... 1-21 2. HAZARD ASSESSMENT .................................................. 2-1 2.1. OVERVIEW OF HAZARD ASSESSMENT AND CHARACTERIZATION . 2-1 2.1.1. Analyses of Data ........................................... 2-1 2.1.2. Presentation of Results ...................................... 2-1 2.2. -

Carcinogenesis and Chemotherapy—Cancer's Continuing Core Challenges: Third Charles Heidelberger Symposium1
(CANCER RESEARCH 50. 7405-7409. November 15. 1990) Meeting Report Carcinogenesis and Chemotherapy—Cancer's Continuing Core Challenges: Third Charles Heidelberger Symposium1 Dr. Charles Heidelberger (1920-1983) devoted his entire delberger was able to attend the symposium and to share working life to cancer research and made outstanding contri memories of Charlie with us. butions in the areas of cancer chemotherapy and chemical carcinogenesis. According to his words (1), these parallel threads of research are "cancer's continuing core challenges." Keynote Lecture Dr. Heidelberger was a pioneer in the development of antime- The program of 38 scientific presentations was commenced tabolic drugs for the treatment of cancer. He introduced a with a keynote lecture given by Dr. T. Sugimura (National fluorine atom into uracil to produce 5-FU,2 a standard com Cancer Center, Tokyo, Japan) on "multiple genetic alterations during carcinogenesis." Dr. Sugimura summarized the multiple ponent of long standing, used in several protocols for the treatment of human solid cancers. His contributions to chemi genetic alterations observed in human cancers, which include cal carcinogenesis include the synthesis of radioactive polycyclic point mutations, rearrangements, sequence deletions, gene am aromatic hydrocarbons in the 1940s, the binding of polycyclic plification, and integration of viral genomes. Through these alterations, activation of oncogenes and inactivation of antion- aromatic hydrocarbons to cellular macromolecules in the 1950s cogenes occur, resulting in the acquisition of malignant phe- and 1960s, and the development of mammalian cell transfor mation in vitro in the C3H/10T'/2 cell line in the 1960s and notypes. Multiple genetic alterations are commonly found in many cancers, but the patterns of alterations vary depending 1970s. -
Radiation Carcinogenesis
Radiation Carcinogenesis November 22, 2016 Dhyan Chandra, Ph.D. Pharmacology and Therapeutics Roswell Park Cancer Institute Email: [email protected] Overview - History of radiation and radiation-induced damage - Bystander effect of radiation - Methods for DNA damage analysis - Stages of carcinogenesis and models - Mechanism of radiation-induced carcinogenesis - Role of oncogenes and tumor suppressors - Risk projections and risk estimates - Importance of dose and age on tumor incidence - Second malignancy after radiotherapy Radiation and cancer • 1895- Roentgen discovered X-rays • 1896- Henri Becquerel discovered radioactivity • 1897- Rutherford discovered α and β rays • 1898- Curies discovered polonium and radium • 1902- First report on radiation-induced skin cancer • 1911- First report of leukemia in 5 radiation workers Types of radiation Ionizing radiation: - α particles (2 protons and 2 neutrons) - β particles (electron equivalent) - Neutrons - Gamma rays - X-rays Non-ionizing radiation: - Microwaves - Visible light - Radio waves and TV waves - UV radiation (except shortest wavelengths) Units and doses Activity: Quantity of a radionuclide which describes the rate at which decays occur in an amount of a radionuclide. The SI unit of radioactivity is the becquerel (Bq), which replaced the old unit, the curie (Ci). Becquerel (Bq): One becquerel corresponds to 1 disintegration of a radionuclide per second. Curie (Ci): Old unit of radioactivity, corresponding to 3.7 x 1010 radioactive disintegrations per second Units and doses Absorbed dose (D): The energy imparted per unit mass by ionizing radiation to matter at a specific point. Gy: The SI unit of absorbed dose is joule per kilogram (J kg-1). The special name for this unit is gray (Gy). -

Role of Micrornas in Lung Carcinogenesis Induced by Asbestos
Journal of Personalized Medicine Review Role of microRNAs in Lung Carcinogenesis Induced by Asbestos Rakhmetkazhy Bersimbaev *, Olga Bulgakova * , Akmaral Aripova, Assiya Kussainova and Oralbek Ilderbayev Department of General Biology and Genomics, Institute of Cell Biology and Biotechnology, L.N. Gumilyov Eurasian National University, Nur-Sultan 010008, Kazakhstan; [email protected] (A.A.); [email protected] (A.K.); [email protected] (O.I.) * Correspondence: [email protected] (R.B.); [email protected] (O.B.); Tel.: +7-7172-33-53-77 (R.B.); +7-707-432-97-27 (O.B.) Abstract: MicroRNAs are a class of small noncoding endogenous RNAs 19–25 nucleotides long, which play an important role in the post-transcriptional regulation of gene expression by targeting mRNA targets with subsequent repression of translation. MicroRNAs are involved in the patho- genesis of numerous diseases, including cancer. Lung cancer is the leading cause of cancer death in the world. Lung cancer is usually associated with tobacco smoking. However, about 25% of lung cancer cases occur in people who have never smoked. According to the International Agency for Research on Cancer, asbestos has been classified as one of the cancerogenic factors for lung cancer. The mechanism of malignant transformation under the influence of asbestos is associated with the genotoxic effect of reactive oxygen species, which initiate the processes of DNA damage in the cell. However, epigenetic mechanisms such as changes in the microRNA expression profile may also be implicated in the pathogenesis of asbestos-induced lung cancer. Numerous studies have shown that microRNAs can serve as a biomarker of the effects of various adverse environmental factors on the human body. -

Chemical and Physical Carcinogenesis: Advances and Perspectives for the 1990S1
[CANCER RESEARCH (SUPPL.) 51, 5023s-5044s, September 15. 1991] Chemical and Physical Carcinogenesis: Advances and Perspectives for the 1990s1 Curtis C. Harris2 Laboratory of Human Carcinogenesis, National Cancer Institute, N1H, Bethesda, Maryland 20892 Abstract the initiated cells with both an altered responsiveness to their microenvironment and moreover exerts a selective clonal ex Carcinogenesis is a multistage process driven by carcinogen-induced pansion advantage when compared to the surrounding normal genetic and epigenetic damage in susceptible cells that gain a selective cells (26-28). The initiated cells may have decreased respon growth advantage and undergo clonal expansion as the result of activation siveness to the inter- and intracellular signals that maintain of protooncogenes and/or inactivation of tumor suppressor genes. There fore, the mutational spectra of chemical and physical carcinogens in these normal tissue architecture and regulate the homeostatic growth critical genes are of interest to define endogenous and exogenous muta and maturation of cells. For example, initiated cells may be less tional mechanisms. The p53 tumor suppressor gene is ideally suited for responsive to negative growth factors, inducers of terminal cell analysis of the mutational spectrum. Such an analysis has revealed differentiation and/or programmed cell death (4, 26, 29-35). evidence for both exogenous and endogenous molecular mechanisms of Perturbation of the normal microenvironment by (a) physical Carcinogenesis. For example, an informative p53 mutational spectrum of means, e.g., wounding of the mouse skin or partial hepatectomy frequent G—»Ttransversions in codon 249 is found in hepatocellular carcinomas from either Qidong, People's Republic of China, or southern in rodents, (b) chemical agents, e.g., exposure of the mouse skin to certain phorbol esters or exposure of the rat liver to Africa. -
The Ecology and Evolution of Wildlife Cancers: Applications for Management and Conservation
Received: 2 December 2019 | Revised: 23 February 2020 | Accepted: 28 February 2020 DOI: 10.1111/eva.12948 SPECIAL ISSUE REVIEW AND SYNTHESES The ecology and evolution of wildlife cancers: Applications for management and conservation Rodrigo Hamede1,2 | Rachel Owen3 | Hannah Siddle3 | Sarah Peck4 | Menna Jones1 | Antoine M. Dujon2 | Mathieu Giraudeau5 | Benjamin Roche5 | Beata Ujvari1,2 | Frédéric Thomas5 1School of Natural Sciences, University of Tasmania, Hobart, Tas., Australia Abstract 2Centre for Integrative Ecology, School of Ecological and evolutionary concepts have been widely adopted to understand host– Life and Environmental Sciences, Deakin pathogen dynamics, and more recently, integrated into wildlife disease management. University, Vic., Australia 3Centre for Biological Sciences, University Cancer is a ubiquitous disease that affects most metazoan species; however, the of Southampton, Southampton, UK role of oncogenic phenomena in eco-evolutionary processes and its implications for 4 Wildlife Veterinarian, Veterinary Register of wildlife management and conservation remains undeveloped. Despite the pervasive Tasmania, South Hobart, Tas., Australia nature of cancer across taxa, our ability to detect its occurrence, progression and 5Centre de Recherches Ecologiques et Evolutives sur le Cancer/Centre de prevalence in wildlife populations is constrained due to logistic and diagnostic limita- Recherches en Ecologie et Evolution de la tions, which suggests that most cancers in the wild are unreported and understudied. Santé, Unité Mixte de Recherches, Institut de Recherches pour le Développement Nevertheless, an increasing number of virus-associated and directly transmissible 224-Centre National de la Recherche cancers in terrestrial and aquatic environments have been detected. Furthermore, Scientifique 5290-Université de Montpellier, Montpellier, France anthropogenic activities and sudden environmental changes are increasingly associ- ated with cancer incidence in wildlife.