Sarah Whyte Dissertation Submitted 2018-09-04 Post-Defence Revisions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Is Sci-Hub Increasing Visibility of Indian Research Papers? an Analytical Evaluation Vivek Kumar Singh1,*, Satya Swarup Srichandan1, Sujit Bhattacharya2
Journal of Scientometric Res. 2021; 10(1):130-134 http://www.jscires.org Perspective Paper Is Sci-Hub Increasing Visibility of Indian Research Papers? An Analytical Evaluation Vivek Kumar Singh1,*, Satya Swarup Srichandan1, Sujit Bhattacharya2 1Department of Computer Science, Banaras Hindu University, Varanasi, Uttar Pradesh, INDIA. 2CSIR-National Institute of Science Technology and Development Studies, New Delhi, INDIA. ABSTRACT Sci-Hub, founded by Alexandra Elbakyan in 2011 in Kazakhstan has, over the years, Correspondence emerged as a very popular source for researchers to download scientific papers. It is Vivek Kumar Singh believed that Sci-Hub contains more than 76 million academic articles. However, recently Department of Computer Science, three foreign academic publishers (Elsevier, Wiley and American Chemical Society) have Banaras Hindu University, filed a lawsuit against Sci-Hub and LibGen before the Delhi High Court and prayed for Varanasi-221005, INDIA. complete blocking these websites in India. It is in this context, that this paper attempts to Email id: [email protected] find out how many Indian research papers are available in Sci-Hub and who downloads them. The citation advantage of Indian research papers available on Sci-Hub is analysed, Received: 16-03-2021 with results confirming that such an advantage do exist. Revised: 29-03-2021 Accepted: 25-04-2021 Keywords: Indian Research, Indian Science, Black Open Access, Open Access, Sci-Hub. DOI: 10.5530/jscires.10.1.16 INTRODUCTION access publishing of their research output, and at the same time encouraging their researchers to publish in openly Responsible Research and Innovation (RRI) has become one accessible forms. -
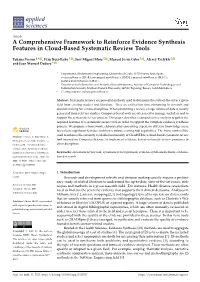
A Comprehensive Framework to Reinforce Evidence Synthesis Features in Cloud-Based Systematic Review Tools
applied sciences Article A Comprehensive Framework to Reinforce Evidence Synthesis Features in Cloud-Based Systematic Review Tools Tatiana Person 1,* , Iván Ruiz-Rube 1 , José Miguel Mota 1 , Manuel Jesús Cobo 1 , Alexey Tselykh 2 and Juan Manuel Dodero 1 1 Department of Informatics Engineering, University of Cadiz, 11519 Puerto Real, Spain; [email protected] (I.R.-R.); [email protected] (J.M.M.); [email protected] (M.J.C.); [email protected] (J.M.D.) 2 Department of Information and Analytical Security Systems, Institute of Computer Technologies and Information Security, Southern Federal University, 347922 Taganrog, Russia; [email protected] * Correspondence: [email protected] Abstract: Systematic reviews are powerful methods used to determine the state-of-the-art in a given field from existing studies and literature. They are critical but time-consuming in research and decision making for various disciplines. When conducting a review, a large volume of data is usually generated from relevant studies. Computer-based tools are often used to manage such data and to support the systematic review process. This paper describes a comprehensive analysis to gather the required features of a systematic review tool, in order to support the complete evidence synthesis process. We propose a framework, elaborated by consulting experts in different knowledge areas, to evaluate significant features and thus reinforce existing tool capabilities. The framework will be used to enhance the currently available functionality of CloudSERA, a cloud-based systematic review Citation: Person, T.; Ruiz-Rube, I.; Mota, J.M.; Cobo, M.J.; Tselykh, A.; tool focused on Computer Science, to implement evidence-based systematic review processes in Dodero, J.M. -

Open Access Availability of Scientific Publications
Analytical Support for Bibliometrics Indicators Open access availability of scientific publications Analytical Support for Bibliometrics Indicators Open access availability of scientific publications* Final Report January 2018 By: Science-Metrix Inc. 1335 Mont-Royal E. ▪ Montréal ▪ Québec ▪ Canada ▪ H2J 1Y6 1.514.495.6505 ▪ 1.800.994.4761 [email protected] ▪ www.science-metrix.com *This work was funded by the National Science Foundation’s (NSF) National Center for Science and Engineering Statistics (NCSES). Any opinions, findings, conclusions or recommendations expressed in this report do not necessarily reflect the views of NCSES or the NSF. The analysis for this research was conducted by SRI International on behalf of NSF’s NCSES under contract number NSFDACS1063289. Analytical Support for Bibliometrics Indicators Open access availability of scientific publications Contents Contents .............................................................................................................................................................. i Tables ................................................................................................................................................................. ii Figures ................................................................................................................................................................ ii Abstract ............................................................................................................................................................ -

Sci-Hub Downloads Lead to More Article Citations
THE SCI-HUB EFFECT:SCI-HUB DOWNLOADS LEAD TO MORE ARTICLE CITATIONS Juan C. Correa⇤ Henry Laverde-Rojas Faculty of Business Administration Faculty of Economics University of Economics, Prague, Czechia Universidad Santo Tomás, Bogotá, Colombia [email protected] [email protected] Fernando Marmolejo-Ramos Julian Tejada Centre for Change and Complexity in Learning Departamento de Psicologia University of South Australia Universidade Federal de Sergipe [email protected] [email protected] Štepánˇ Bahník Faculty of Business Administration University of Economics, Prague, Czechia [email protected] ABSTRACT Citations are often used as a metric of the impact of scientific publications. Here, we examine how the number of downloads from Sci-hub as well as various characteristics of publications and their authors predicts future citations. Using data from 12 leading journals in economics, consumer research, neuroscience, and multidisciplinary research, we found that articles downloaded from Sci-hub were cited 1.72 times more than papers not downloaded from Sci-hub and that the number of downloads from Sci-hub was a robust predictor of future citations. Among other characteristics of publications, the number of figures in a manuscript consistently predicts its future citations. The results suggest that limited access to publications may limit some scientific research from achieving its full impact. Keywords Sci-hub Citations Scientific Impact Scholar Consumption Knowledge dissemination · · · · Introduction Science and its outputs are essential in daily life, as they help to understand our world and provide a basis for better decisions. Although scientific findings are often cited in social media and shared outside the scientific community [1], their primary use is what we could call “scholar consumption.” This phenomenon includes using websites that provide subscription-based access to massive databases of scientific research [2]. -

Google Scholar, Web of Science, and Scopus
Journal of Informetrics, vol. 12, no. 4, pp. 1160-1177, 2018. https://doi.org/10.1016/J.JOI.2018.09.002 Google Scholar, Web of Science, and Scopus: a systematic comparison of citations in 252 subject categories Alberto Martín-Martín1 , Enrique Orduna-Malea2 , Mike 3 1 Thelwall , Emilio Delgado López-Cózar Version 1.6 March 12, 2019 Abstract Despite citation counts from Google Scholar (GS), Web of Science (WoS), and Scopus being widely consulted by researchers and sometimes used in research evaluations, there is no recent or systematic evidence about the differences between them. In response, this paper investigates 2,448,055 citations to 2,299 English-language highly-cited documents from 252 GS subject categories published in 2006, comparing GS, the WoS Core Collection, and Scopus. GS consistently found the largest percentage of citations across all areas (93%-96%), far ahead of Scopus (35%-77%) and WoS (27%-73%). GS found nearly all the WoS (95%) and Scopus (92%) citations. Most citations found only by GS were from non-journal sources (48%-65%), including theses, books, conference papers, and unpublished materials. Many were non-English (19%- 38%), and they tended to be much less cited than citing sources that were also in Scopus or WoS. Despite the many unique GS citing sources, Spearman correlations between citation counts in GS and WoS or Scopus are high (0.78-0.99). They are lower in the Humanities, and lower between GS and WoS than between GS and Scopus. The results suggest that in all areas GS citation data is essentially a superset of WoS and Scopus, with substantial extra coverage. -

I Introducing Primary Scientific Literature to First-Year
SUMMER 2013 • Volume 34, Number 4 ON THE WEB COUNCIL ON UNDERGRADUATE RESEARCH z Introducing Primary Scientific Literature To First-year Undergraduate Researchers Swan, Chris, Jesse Cooper, and Amanda Stockwell. 2007. “Introducing Engineering Students to Research Through a First Year Advising Program.” Susan Carson, Eric S. Miller American Society for Engineering Education. Honolulu, Hawaii, June 24-27. North Carolina State University of the phages in the second semester. The student experience at our institution incorporated critical aspects of under- Wonziak, Carl. 2011. “Freshman Fellows: Recruiting and Retaining Great In the past decade, recommendations for reforming the graduate research, including: project ownership; keeping a Students Through Research Opportunities.” Council on Undergraduate Research way we teach science to undergraduate students have detailed laboratory notebook; disseminating research find- Quarterly 32: 8-15. surged. In particular, emerging research suggests that stu- ings in both oral and written forms; and— the focus of this Zydney, Andrew L., Joan S. Bennett, Abdus Shahid, and Karen W. Bauer. dents benefit from self-guided learning practices that are article—reading and discussing relevant primary scientific 2002. “Faculty Perspectives Regarding Undergraduate Research Experience in focused on core concepts and competencies rather than on literature. Science and Engineering.” Journal of Engineering Education 91: 291-297 content coverage. (National Research Council 2003, 2007, 2009; American Advancement for -

Amplifying the Impact of Open Access: Wikipedia and the Diffusion of Science
(forthcoming in the Journal of the Association for Information Science and Technology) Amplifying the Impact of Open Access: Wikipedia and the Diffusion of Science Misha Teplitskiy Grace Lu Eamon Duede Dept. of Sociology and KnowledgeLab Computation Institute and KnowledgeLab University of Chicago KnowledgeLab University of Chicago [email protected] University of Chicago [email protected] (773) 834-4787 [email protected] (773) 834-4787 5735 South Ellis Avenue (773) 834-4787 5735 South Ellis Avenue Chicago, Illinois 60637 5735 South Ellis Avenue Chicago, Illinois 60637 Chicago, Illinois 60637 Abstract With the rise of Wikipedia as a first-stop source for scientific knowledge, it is important to compare its representation of that knowledge to that of the academic literature. Here we identify the 250 most heavi- ly used journals in each of 26 research fields (4,721 journals, 19.4M articles in total) indexed by the Scopus database, and test whether topic, academic status, and accessibility make articles from these journals more or less likely to be referenced on Wikipedia. We find that a journal’s academic status (im- pact factor) and accessibility (open access policy) both strongly increase the probability of its being ref- erenced on Wikipedia. Controlling for field and impact factor, the odds that an open access journal is referenced on the English Wikipedia are 47% higher compared to paywall journals. One of the implica- tions of this study is that a major consequence of open access policies is to significantly amplify the dif- fusion of science, through an intermediary like Wikipedia, to a broad audience. Word count: 7894 Introduction Wikipedia, one of the most visited websites in the world1, has become a destination for information of all kinds, including information about science (Heilman & West, 2015; Laurent & Vickers, 2009; Okoli, Mehdi, Mesgari, Nielsen, & Lanamäki, 2014; Spoerri, 2007). -

Public Health Chronicles
Public Health Chronicles TOBACCO INDUSTRY bacco industry to manipulate information on the risks of MANIPULATION OF RESEARCH tobacco (Figure). These strategies have remained remark- ably constant since the early 1950s. During the 1950s and Lisa A. Bero, PhD 1960s, the tobacco industry focused on refuting data on the adverse effects of active smoking. The industry applied the Research findings provide the basis for estimates of risk. tools it had developed during this time to refute data on However, research findings or “facts” are subject to interpre- the adverse effects of secondhand smoke exposure from the tation and to the social construction of the evidence.1 Re- 1970s through the 1990s. search evidence has a context. The roles of framing, problem The release of previously secret internal tobacco industry definition, and choice of language influence risk communi- documents as a result of the Master Settlement Agreement cation.2 Since data do not “speak for themselves,” interest in 1998 has given the public health community insight into groups can play a critical role in creating and communicat- the tobacco industry’s motives, strategies, tactics, and data.16 ing the research evidence on risk. These documents show that for decades the industry has An interest group is an organized group with a narrowly tried to generate controversy about the health risks of its defined viewpoint, which protects its position or profits.3 products. The internal documents also reveal how the in- These groups are not exclusively business groups, but can dustry has been concerned about maintaining its credibility include all kinds of organizations that may attempt to influ- as it has manipulated research on tobacco.16 ence government.4,5 Interest groups can be expected to con- The tobacco industry has explicitly stated its goal of gen- struct the evidence about a health risk to support their erating controversy about the health risks of tobacco. -

Scientific Literature Resources: a Guide for CNRA Employees
Scientific Literature Resources: A Guide for CNRA Employees GAVIN NEWSOM, GOVERNOR FEBRUARY 2020 PREPARED BY Nicole Waugh, California Energy Commission Library Amy Loseth, California Geological Survey Library Jenny Woo, California Energy Commission Library CDFW Literature Access SIFT (Science Institute Focus Group) 2 TABLE OF CONTENTS INTRODUCTION ............................................................................................................................... 7 SECTION 1: ONLINE RESOURCES ..................................................................................................... 8 1.1 Citation Databases ................................................................................................................ 8 Scopus ...................................................................................................................................... 8 Google Scholar ......................................................................................................................... 8 Pubmed .................................................................................................................................... 8 1.2 Databases .............................................................................................................................. 9 Biodiversity Heritage Library ................................................................................................... 9 Birds of North America ........................................................................................................... -
An Introduction to Bibliometrics
AN INTRODUCTION TO BIBLIOMETRICS PROF JONATHAN GRANT THE POLICY INSTITUTE, KING’S COLLEGE LONDON NOVEMBER 10- 2015 LEARNING OBJECTIVES AND KEY MESSAGES Introduce you to bibliometrics in a general manner Show you the basic requirements for conducting bibliometric analyses You will learn about invalid bibliometric measures around Build up expertise in bibliometrics before using it ! Use bibliometrics wisely, and in context ! CONTENT OF TALK Introduction of bibliometrics and data systems Basic requirements for bibliometric analysis Validity of research assessment Bibliometric indicators Some example uses THE METRICS TIDE PROVIDES GOOD OVERVIEW ON (BIBLIO)METRICS http:// www.hefce.ac.uk /media/ HEFCE,2014/ Content/Pubs/ Independentrese arch/2015/ The,Metric,Tide / 2015_metric_tid e.pdf WHAT IS BIBLIOMETRICS? • The use of published scientific literature (articles, books, conference proceedings, etc.) for measuring research activity eg output volume, science 'quality', interdisciplinarity, networking • New knowledge created by scientists is embedded in the scientific literature • By measuring scientific literature, we measure knowledge and the ways it is produced BIBLIOMETRICS RELIES ON INFORMATION IN A PAPER Journal Title Authors Addresses Abstract References BIBLIOGRAPHIC DATA SYSTEMS In the field we work with three bibliographic databases: Web of Science by Thomson Reuters; Scopus by Elsevier Science; Google Scholar by Google. Understanding strengths and weakness of different databases is key (i.e. “Coverage”) LEVELS OF BIBLIOMETRIC ANALYSIS Macro level eg country and region comparisons Meso level eg research organisation, universities, institutes Mirco level eg analysis of programmes, groups or individual researchers THREE METHODS OF DATA COLLECTION 1. Based on list of names of researchers 2. Based on a list of publications of a unit 3. -

Using Scientific Literature in Biology Courses I. Types of Literature II
Literature Research B-1 Using Scientific Literature in Biology Courses I. Types of Literature Introduction Page 2 Scientific Literature Primary literature Page 2 Secondary literature Page 3 Comparison of primary and secondary Page 4 Guidelines for deciding which sources to use Page 5 Citing Sources of Information Guidelines for deciding when to cite Page 6 Avoiding plagiarism in scientific writing Page 6 II. How to Cite Sources The Name-Year System of Citing Page 7 Creating a Literature Cited List Page 8 Formatting References Page 9 Print Resources Page 10 Electronic Resources Page 11 Sources not in Electronic Form or Print Page 12 Literature Research B-2 Introduction In science, knowledge accumulates as individuals study phenomena in the natural world. These researchers base their studies on the information contributed in the past by others, and the results of the new studies provide new information or different interpretations of the subjects under investigation. Scientists share their work through the publication of the results of their original research projects. In this way, the new knowledge is available to all who have an interest in those subjects. At Earlham, we believe it is important that you learn how to access and use this scientific literature. Our reasons for this include: • Reading scientific literature is one of the necessary components of scientific research. • Using scientific literature shows something about the social structure of the activity of scientists -- it illustrates the formal means by which scientists communicate with each other and with wider communities. • By reading scientific literature, you will see examples of the writing style by which scientists communicate. -

Scientific Literature Review Overview
Scientific Literature Review Overview: 1. What is a Scientific Literature Review? 2. How to write a Scientific Literature Review 3. Key elements of a Coherent Literature Review 4. Literature Review Structure What is a Scientific Literature Review? Scientific Literature Review: A scientific literature review is a critical account of what has been published on a topic by accredited researchers. It may be: • A stand-alone assignment • An introduction to an essay, report, thesis, etc. • Part of research/grant proposals Scientific Literature Review: Writing a literature review will: • Improve your topic knowledge • Provide new insight on your topic to others • Demonstrate your literature searching abilities • Demonstrate your critical analysis skills • Demonstrate your communication/writing skills …your lecturer will be marking you on these skills! Scientific Literature Review: A scientific literature review is not: • An English essay… use scientific writing! • A summary of each research article that you read • Based on personal opinion or biased towards your opinion • A chronological history of events in your research area Scientific Literature Review: What is the purpose of a literature review? Scientific Literature Review: What is the purpose of a literature review? Communication and advancement of scientific knowledge! • Scientific knowledge is not static: reviews help scientists to understand how knowledge in a particular field is changing and developing over time • There is a significant output of scientific publications – literature