Rubidium Chloride Modulated the Intestinal Microbiota Community in Mice
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Phylogenetics of Archaeal Lipids Amy Kelly 9/27/2006 Outline
Phylogenetics of Archaeal Lipids Amy Kelly 9/27/2006 Outline • Phlogenetics of Archaea • Phlogenetics of archaeal lipids • Papers Phyla • Two? main phyla – Euryarchaeota • Methanogens • Extreme halophiles • Extreme thermophiles • Sulfate-reducing – Crenarchaeota • Extreme thermophiles – Korarchaeota? • Hyperthermophiles • indicated only by environmental DNA sequences – Nanoarchaeum? • N. equitans a fast evolving euryarchaeal lineage, not novel, early diverging archaeal phylum – Ancient archael group? • In deepest brances of Crenarchaea? Euryarchaea? Archaeal Lipids • Methanogens – Di- and tetra-ethers of glycerol and isoprenoid alcohols – Core mostly archaeol or caldarchaeol – Core sometimes sn-2- or Images removed due to sn-3-hydroxyarchaeol or copyright considerations. macrocyclic archaeol –PMI • Halophiles – Similar to methanogens – Exclusively synthesize bacterioruberin • Marine Crenarchaea Depositional Archaeal Lipids Biological Origin Environment Crocetane methanotrophs? methane seeps? methanogens, PMI (2,6,10,15,19-pentamethylicosane) methanotrophs hypersaline, anoxic Squalane hypersaline? C31-C40 head-to-head isoprenoids Smit & Mushegian • “Lost” enzymes of MVA pathway must exist – Phosphomevalonate kinase (PMK) – Diphosphomevalonate decarboxylase – Isopentenyl diphosphate isomerase (IPPI) Kaneda et al. 2001 Rohdich et al. 2001 Boucher et al. • Isoprenoid biosynthesis of archaea evolved through a combination of processes – Co-option of ancestral enzymes – Modification of enzymatic specificity – Orthologous and non-orthologous gene -

WO 2018/064165 A2 (.Pdf)
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2018/064165 A2 05 April 2018 (05.04.2018) W !P O PCT (51) International Patent Classification: Published: A61K 35/74 (20 15.0 1) C12N 1/21 (2006 .01) — without international search report and to be republished (21) International Application Number: upon receipt of that report (Rule 48.2(g)) PCT/US2017/053717 — with sequence listing part of description (Rule 5.2(a)) (22) International Filing Date: 27 September 2017 (27.09.2017) (25) Filing Language: English (26) Publication Langi English (30) Priority Data: 62/400,372 27 September 2016 (27.09.2016) US 62/508,885 19 May 2017 (19.05.2017) US 62/557,566 12 September 2017 (12.09.2017) US (71) Applicant: BOARD OF REGENTS, THE UNIVERSI¬ TY OF TEXAS SYSTEM [US/US]; 210 West 7th St., Austin, TX 78701 (US). (72) Inventors: WARGO, Jennifer; 1814 Bissonnet St., Hous ton, TX 77005 (US). GOPALAKRISHNAN, Vanch- eswaran; 7900 Cambridge, Apt. 10-lb, Houston, TX 77054 (US). (74) Agent: BYRD, Marshall, P.; Parker Highlander PLLC, 1120 S. Capital Of Texas Highway, Bldg. One, Suite 200, Austin, TX 78746 (US). (81) Designated States (unless otherwise indicated, for every kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DJ, DK, DM, DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, HR, HU, ID, IL, IN, IR, IS, JO, JP, KE, KG, KH, KN, KP, KR, KW, KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. -

Proteome Cold-Shock Response in the Extremely Acidophilic Archaeon, Cuniculiplasma Divulgatum
microorganisms Article Proteome Cold-Shock Response in the Extremely Acidophilic Archaeon, Cuniculiplasma divulgatum Rafael Bargiela 1 , Karin Lanthaler 1,2, Colin M. Potter 1,2 , Manuel Ferrer 3 , Alexander F. Yakunin 1,2, Bela Paizs 1,2, Peter N. Golyshin 1,2 and Olga V. Golyshina 1,2,* 1 School of Natural Sciences, Bangor University, Deiniol Rd, Bangor LL57 2UW, UK; [email protected] (R.B.); [email protected] (K.L.); [email protected] (C.M.P.); [email protected] (A.F.Y.); [email protected] (B.P.); [email protected] (P.N.G.) 2 Centre for Environmental Biotechnology, Bangor University, Deiniol Rd, Bangor LL57 2UW, UK 3 Systems Biotechnology Group, Department of Applied Biocatalysis, CSIC—Institute of Catalysis, Marie Curie 2, 28049 Madrid, Spain; [email protected] * Correspondence: [email protected]; Tel.: +44-1248-388607; Fax: +44-1248-382569 Received: 27 April 2020; Accepted: 15 May 2020; Published: 19 May 2020 Abstract: The archaeon Cuniculiplasma divulgatum is ubiquitous in acidic environments with low-to-moderate temperatures. However, molecular mechanisms underlying its ability to thrive at lower temperatures remain unexplored. Using mass spectrometry (MS)-based proteomics, we analysed the effect of short-term (3 h) exposure to cold. The C. divulgatum genome encodes 2016 protein-coding genes, from which 819 proteins were identified in the cells grown under optimal conditions. In line with the peptidolytic lifestyle of C. divulgatum, its intracellular proteome revealed the abundance of proteases, ABC transporters and cytochrome C oxidase. From 747 quantifiable polypeptides, the levels of 582 proteins showed no change after the cold shock, whereas 104 proteins were upregulated suggesting that they might be contributing to cold adaptation. -
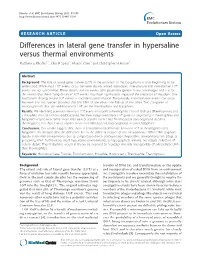
Differences in Lateral Gene Transfer in Hypersaline Versus Thermal Environments Matthew E Rhodes1*, John R Spear2, Aharon Oren3 and Christopher H House1
Rhodes et al. BMC Evolutionary Biology 2011, 11:199 http://www.biomedcentral.com/1471-2148/11/199 RESEARCH ARTICLE Open Access Differences in lateral gene transfer in hypersaline versus thermal environments Matthew E Rhodes1*, John R Spear2, Aharon Oren3 and Christopher H House1 Abstract Background: The role of lateral gene transfer (LGT) in the evolution of microorganisms is only beginning to be understood. While most LGT events occur between closely related individuals, inter-phylum and inter-domain LGT events are not uncommon. These distant transfer events offer potentially greater fitness advantages and it is for this reason that these “long distance” LGT events may have significantly impacted the evolution of microbes. One mechanism driving distant LGT events is microbial transformation. Theoretically, transformative events can occur between any two species provided that the DNA of one enters the habitat of the other. Two categories of microorganisms that are well-known for LGT are the thermophiles and halophiles. Results: We identified potential inter-class LGT events into both a thermophilic class of Archaea (Thermoprotei) and a halophilic class of Archaea (Halobacteria). We then categorized these LGT genes as originating in thermophiles and halophiles respectively. While more than 68% of transfer events into Thermoprotei taxa originated in other thermophiles, less than 11% of transfer events into Halobacteria taxa originated in other halophiles. Conclusions: Our results suggest that there is a fundamental difference between LGT in thermophiles and halophiles. We theorize that the difference lies in the different natures of the environments. While DNA degrades rapidly in thermal environments due to temperature-driven denaturization, hypersaline environments are adept at preserving DNA. -

UC Berkeley UC Berkeley Electronic Theses and Dissertations
UC Berkeley UC Berkeley Electronic Theses and Dissertations Title Analyzing Microbial Physiology and Nutrient Transformation in a Model, Acidophilic Microbial Community using Integrated `Omics' Technologies Permalink https://escholarship.org/uc/item/259113st Author Justice, Nicholas Bruce Publication Date 2013 Supplemental Material https://escholarship.org/uc/item/259113st#supplemental Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California Analyzing Microbial Physiology and Nutrient Transformation in a Model, Acidophilic Microbial Community using Integrated ‘Omics’ Technologies By Nicholas Bruce Justice A dissertation submitted in partial satisfaction of the requirements for the degree of Doctor of Philosophy in Microbiology in the Graduate Division of the University of California, Berkeley Committee in charge: Professor Jillian Banfield, Chair Professor Mary Firestone Professor Mary Power Professor John Coates Fall 2013 Abstract Analyzing Microbial Physiology and Nutrient Transformation in a Model, Acidophilic Microbial Community using Integrated ‘Omics’ Technologies by Nicholas Bruce Justice Doctor of Philosophy in Microbiology University of California, Berkeley Professor Jillian F. Banfield, Chair Understanding how microorganisms contribute to nutrient transformations within their community is critical to prediction of overall ecosystem function, and thus is a major goal of microbial ecology. Communities of relatively tractable complexity provide a unique opportunity to study the distribution of metabolic characteristics amongst microorganisms and how those characteristics subscribe diverse ecological functions to co-occurring, and often closely related, species. The microbial communities present in the low-pH, metal-rich environment of the acid mine drainage (AMD) system in Richmond Mine at Iron Mountain, CA constitute a model microbial community due to their relatively low diversity and extensive characterization over the preceding fifteen years. -
Influence of External and Internal Environmental Factors on Intestinal Microbiota of Wild and Domestic Animals A
Influence of external and internal environmental factors on intestinal microbiota of wild and domestic of animals factors on intestinal microbiota Influence of external and internal environmental Influence of external and internal environmental factors on intestinal microbiota of wild and domestic animals A. Umanets Alexander Umanets Propositions 1. Intestinal microbiota and resistome composition of wild animals are mostly shaped by the animals’ diet and lifestyle. (this thesis) 2. When other environmental factors are controlled, genetics of the host lead to species- or breed specific microbiota patterns. (this thesis) 3. Identifying the response of microbial communities to factors that only have a minor contribution to overall microbiota variation faces the same problems as the discovery of exoplanets. 4. Observational studies in microbial ecology using cultivation- independent methods should be considered only as a guide for further investigations that employ controlled experimental conditions and mechanistic studies of cause-effect relationships. 5. Public fear of genetic engineering and artificial intelligence is not helped by insufficient public education and misleading images created through mass- and social media. 6. Principles of positive (Darwinian) and negative selection govern the repertoire of techniques used within martial arts. Propositions belonging to the thesis, entitled Influence of external and internal environmental factors on intestinal microbiota of wild and domestic animals Alexander Umanets Wageningen, 17 October -

Advances in Applied Microbiology, Voume 49 (Advances in Applied
ADVANCES IN Applied Microbiology VOLUME 49 ThisPageIntentionallyLeftBlank ADVANCES IN Applied Microbiology Edited by ALLEN I. LASKIN JOAN W. BENNETT Somerset, New Jersey New Orleans, Louisiana GEOFFREY M. GADD Dundee, United Kingdom VOLUME 49 San Diego New York Boston London Sydney Tokyo Toronto This book is printed on acid-free paper. ∞ Copyright C 2001 by ACADEMIC PRESS All Rights Reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the Publisher. The appearance of the code at the bottom of the first page of a chapter in this book indicates the Publisher’s consent that copies of the chapter may be made for personal or internal use of specific clients. This consent is given on the condition, however, that the copier pay the stated per copy fee through the Copyright Clearance Center, Inc. (222 Rosewood Drive, Danvers, Massachusetts 01923), for copying beyond that permitted by Sections 107 or 108 of the U.S. Copyright Law. This consent does not extend to other kinds of copying, such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale. Copy fees for pre-2000 chapters are as shown on the title pages. If no fee code appears on the title page, the copy fee is the same as for current chapters. 0065-2164/01 $35.00 Academic Press A division of Harcourt, Inc. 525 B Street, Suite 1900, San Diego, California 92101-4495, USA http://www.academicpress.com Academic Press Harcourt Place, 32 Jamestown Road, London NW1 7BY, UK http://www.academicpress.com International Standard Serial Number: 0065-2164 International Standard Book Number: 0-12-002649-X PRINTED IN THE UNITED STATES OF AMERICA 010203040506MM987654321 CONTENTS Microbial Transformations of Explosives SUSAN J. -

Occurrence and Expression of Novel Methyl-Coenzyme M Reductase Gene
www.nature.com/scientificreports OPEN Occurrence and expression of novel methyl-coenzyme M reductase gene (mcrA) variants in hot spring Received: 6 April 2017 Accepted: 27 June 2017 sediments Published: xx xx xxxx Luke J. McKay1,2, Roland Hatzenpichler1,3, William P. Inskeep2 & Matthew W. Fields1,4 Recent discoveries have shown that the marker gene for anaerobic methane cycling (mcrA) is more widespread in the Archaea than previously thought. However, it remains unclear whether novel mcrA genes associated with the Bathyarchaeota and Verstraetearchaeota are distributed across diverse environments. We examined two geochemically divergent but putatively methanogenic regions of Yellowstone National Park to investigate whether deeply-rooted archaea possess and express novel mcrA genes in situ. Small-subunit (SSU) rRNA gene analyses indicated that Bathyarchaeota were predominant in seven of ten sediment layers, while the Verstraetearchaeota and Euryarchaeota occurred in lower relative abundance. Targeted amplifcation of novel mcrA genes suggested that diverse taxa contribute to alkane cycling in geothermal environments. Two deeply-branching mcrA clades related to Bathyarchaeota were identifed, while highly abundant verstraetearchaeotal mcrA sequences were also recovered. In addition, detection of SSU rRNA and mcrA transcripts from one hot spring suggested that predominant Bathyarchaeota were also active, and that methane cycling genes are expressed by the Euryarchaeota, Verstraetearchaeota, and an unknown lineage basal to the Bathyarchaeota. These fndings greatly expand the diversity of the key marker gene for anaerobic alkane cycling and outline the need for greater understanding of the functional capacity and phylogenetic afliation of novel mcrA variants. Archaea are the primary drivers of CH4 cycling on our planet. -

Confident Phylogenetic Identification of Uncultured Prokaryotes Through
Environmental Microbiology (2019) 21(7), 2485–2498 doi:10.1111/1462-2920.14636 Confident phylogenetic identification of uncultured prokaryotes through long read amplicon sequencing of the 16S-ITS-23S rRNA operon Joran Martijn ,1 Anders E. Lind,1 Max E. Schön,1 method to those who wish to cost-effectively and confi- Ian Spiertz,1 Lina Juzokaite,1 Ignas Bunikis,2 dently estimate the phylogenetic diversity of prokary- Olga V. Pettersson2 and Thijs J. G. Ettema 1,3* otes in environmental samples at high throughput. 1Department of Cell and Molecular Biology, Science for Life Laboratory, Uppsala University, SE-75123, Uppsala, Sweden. Introduction 2Science for Life Laboratory, Uppsala University, The 16S rRNA gene has been used for decades to phylo- SE-75185, Uppsala, Sweden. genetically classify bacteria and archaea (Woese and Fox, 3 Laboratory of Microbiology, Department of 1977). The gene excels in this respect because of its uni- Agrotechnology and Food Sciences, Wageningen versal occurrence, resistance to horizontal gene transfer University, Stippeneng 4, 6708WE, Wageningen, and high degree of conservation (Woese, 1987; Green The Netherlands. and Noller, 1997). Highly conserved regions are inter- spersed with highly variable regions, allowing for phyloge- Summary netic classification at species and higher taxonomic levels. In addition, the gene has proven to be an excellent target Amplicon sequencing of the 16S rRNA gene is the pre- for studies aiming to quantify the taxonomic composition dominant method to quantify microbial compositions of microbial communities via high-throughput PCR and to discover novel lineages. However, traditional amplicon sequencing (Doolittle, 1999). Primers are usually short amplicons often do not contain enough informa- designed such that they anneal to stretches of conserved tion to confidently resolve their phylogeny. -

Downloaded from Genome Website
bioRxiv preprint doi: https://doi.org/10.1101/2020.11.18.388454; this version posted November 19, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 1 Characterization of the first cultured free-living representative of 2 Candidatus Izimaplasma uncovers its unique biology 3 Rikuan Zheng1,2,3,4, Rui Liu1,2,4, Yeqi Shan1,2,3,4, Ruining Cai1,2,3,4, Ge Liu1,2,4, Chaomin Sun1,2,4* 1 4 CAS Key Laboratory of Experimental Marine Biology & Center of Deep Sea 5 Research, Institute of Oceanology, Chinese Academy of Sciences, Qingdao, China 2 6 Laboratory for Marine Biology and Biotechnology, Qingdao National Laboratory 7 for Marine Science and Technology, Qingdao, China 3 8 College of Earth Science, University of Chinese Academy of Sciences, Beijing, 9 China 10 4Center of Ocean Mega-Science, Chinese Academy of Sciences, Qingdao, China 11 12 * Corresponding author 13 Chaomin Sun Tel.: +86 532 82898857; fax: +86 532 82898857. 14 E-mail address: [email protected] 15 16 17 Key words: Candidatus Izimaplasma, uncultivation, biogeochemical cycling, 18 extracellular DNA, in situ, deep sea 19 Running title: Characterization of the first cultured Izimaplasma 20 21 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.11.18.388454; this version posted November 19, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 22 Abstract 23 Candidatus Izimaplasma, an intermediate in the reductive evolution from Firmicutes 24 to Mollicutes, was proposed to represent a novel class of free-living wall-less bacteria 25 within the phylum Tenericutes found in deep-sea methane seeps. -

(Gid ) Genes Coding for Putative Trna:M5u-54 Methyltransferases in 355 Bacterial and Archaeal Complete Genomes
Table S1. Taxonomic distribution of the trmA and trmFO (gid ) genes coding for putative tRNA:m5U-54 methyltransferases in 355 bacterial and archaeal complete genomes. Asterisks indicate the presence and the number of putative genes found. Genomes Taxonomic position TrmA Gid Archaea Crenarchaea Aeropyrum pernix_K1 Crenarchaeota; Thermoprotei; Desulfurococcales; Desulfurococcaceae Cenarchaeum symbiosum Crenarchaeota; Thermoprotei; Cenarchaeales; Cenarchaeaceae Pyrobaculum aerophilum_str_IM2 Crenarchaeota; Thermoprotei; Thermoproteales; Thermoproteaceae Sulfolobus acidocaldarius_DSM_639 Crenarchaeota; Thermoprotei; Sulfolobales; Sulfolobaceae Sulfolobus solfataricus Crenarchaeota; Thermoprotei; Sulfolobales; Sulfolobaceae Sulfolobus tokodaii Crenarchaeota; Thermoprotei; Sulfolobales; Sulfolobaceae Euryarchaea Archaeoglobus fulgidus Euryarchaeota; Archaeoglobi; Archaeoglobales; Archaeoglobaceae Haloarcula marismortui_ATCC_43049 Euryarchaeota; Halobacteria; Halobacteriales; Halobacteriaceae; Haloarcula Halobacterium sp Euryarchaeota; Halobacteria; Halobacteriales; Halobacteriaceae; Haloarcula Haloquadratum walsbyi Euryarchaeota; Halobacteria; Halobacteriales; Halobacteriaceae; Haloquadra Methanobacterium thermoautotrophicum Euryarchaeota; Methanobacteria; Methanobacteriales; Methanobacteriaceae Methanococcoides burtonii_DSM_6242 Euryarchaeota; Methanomicrobia; Methanosarcinales; Methanosarcinaceae Methanococcus jannaschii Euryarchaeota; Methanococci; Methanococcales; Methanococcaceae Methanococcus maripaludis_S2 Euryarchaeota; Methanococci; -

The Novel Extremely Acidophilic, Cell-Wall-Deficient Archaeon Cuniculiplasma Divulgatum Gen
International Journal of Systematic and Evolutionary Microbiology (2016), 66, 332–340 DOI 10.1099/ijsem.0.000725 The novel extremely acidophilic, cell-wall-deficient archaeon Cuniculiplasma divulgatum gen. nov., sp. nov. represents a new family, Cuniculiplasmataceae fam. nov., of the order Thermoplasmatales Olga V. Golyshina,1 Heinrich Lu¨nsdorf,2 Ilya V. Kublanov,3 Nadine I. Goldenstein,4 Kai-Uwe Hinrichs4 and Peter N. Golyshin1 Correspondence 1School of Biological Sciences, Bangor University, Deiniol Rd, Bangor LL57 2UW, UK Olga V. Golyshina 2Central Unit of Microscopy, Helmholtz Centre for Infection Research, Inhoffenstrasse 7, [email protected] Braunschweig 38124, Germany 3Winogradsky Institute of Microbiology, Russian Academy of Sciences, Prospect 60-Letiya Oktyabrya 7/2, Moscow 117312, Russia 4MARUM – Center for Marine Environmental Sciences, University of Bremen, Leobener Str., Bremen 28359, Germany Two novel cell-wall-less, acidophilic, mesophilic, organotrophic and facultatively anaerobic archaeal strains were isolated from acidic streamers formed on the surfaces of copper-ore- containing sulfidic deposits in south-west Spain and North Wales, UK. Cells of the strains varied from 0.1 to 2 mm in size and were pleomorphic, with a tendency to form filamentous structures. The optimal pH and temperature for growth for both strains were 1.0–1.2 and 2 37–40 8C, with the optimal substrates for growth being beef extract (3 g l 1) for strain S5T and 2 beef extract with tryptone (3 and 1 g l 1, respectively) for strain PM4. The lipid composition was dominated by intact polar lipids consisting of a glycerol dibiphytanyl glycerol tetraether (GDGT) core attached to predominantly glycosidic polar headgroups.