BHS 499-07 Memory and Amnesia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dissociation Between Declarative and Procedural Mechanisms in Long-Term Memory
! DISSOCIATION BETWEEN DECLARATIVE AND PROCEDURAL MECHANISMS IN LONG-TERM MEMORY A dissertation submitted to the Kent State University College of Education, Health, and Human Services in partial fulfillment of the requirements for the degree of Doctor of Philosophy By Dale A. Hirsch August, 2017 ! A dissertation written by Dale A. Hirsch B.A., Cleveland State University, 2010 M.A., Cleveland State University, 2013 Ph.D., Kent State University, 2017 Approved by _________________________, Director, Doctoral Dissertation Committee Bradley Morris _________________________, Member, Doctoral Dissertation Committee Christopher Was _________________________, Member, Doctoral Dissertation Committee Karrie Godwin Accepted by _________________________, Director, School of Lifespan Development and Mary Dellmann-Jenkins Educational Sciences _________________________, Dean, College of Education, Health and Human James C. Hannon Services ! ""! ! HIRSCH, DALE A., Ph.D., August 2017 Educational Psychology DISSOCIATION BETWEEN DECLARATIVE AND PROCEDURAL MECHANISMS IN LONG-TERM MEMORY (66 pp.) Director of Dissertation: Bradley Morris The purpose of this study was to investigate the potential dissociation between declarative and procedural elements in long-term memory for a facilitation of procedural memory (FPM) paradigm. FPM coupled with a directed forgetting (DF) manipulation was utilized to highlight the dissociation. Three experiments were conducted to that end. All three experiments resulted in facilitation for categorization operations. Experiments one and two additionally found relatively poor recognition for items that participants were told to forget despite the fact that relevant categorization operations were facilitated. Experiment three resulted in similarly poor recognition for category names that participants were told to forget. Taken together, the three experiments in this investigation demonstrate a clear dissociation between the procedural and declarative elements of the FPM task. -

Confabulation Morris Moscovitch N
Confabulation Morris Moscovitch n Memory distortion, rather than memory loss, occurs because re- membering is often a reconstructive process. To convince oneself of this, one only has to try to remember yesterday's events and the order in which they occurred; or even, as sometimes happens, what day yesterday was. Damage to neural structures involved in the storage, retention, and auto- matic recovery of encoded information produces memory loss which in its most severe form is amnesia (see Squire, 1992; Squire, Chapter 7 of this volume). Memory distortion, however, is no more a feature of the memory deficit of these patients than it is of the benign, and all too common, memory failure of normal people. When, however, neural structures involved in the reconstructive process are damaged, memory distortion becomes prominent and results in confabulation, even though memory loss may not be severe. Though flagrantly distorted and easily elicited, confabulations nonetheless share many characteristics with the type of memory distortions we all pro- duce. Studying confabulation from a cognitive neuroscience perspective, of interest in its own right, may also contribute to our understanding of how memories are normally distorted. Confabulation is a symptom that accompanies many neuropsychological disorders and some psychiatric ones, such as schizophrenia (Enoch, Tretho- wan, and Baker, 1967; Joseph, 1986). What distinguishes confabulation from lying is that typically there is no intent to deceive and the patient is unaware of the falsehoods. It is an "honest lying." Confabulation is simple to detect when the information the patient provides is patently false, self- contradictory, bizarre, or at least highly improbable. -
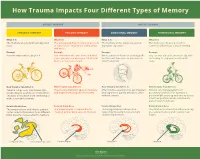
How Trauma Impacts Four Different Types of Memory
How Trauma Impacts Four Different Types of Memory EXPLICIT MEMORY IMPLICIT MEMORY SEMANTIC MEMORY EPISODIC MEMORY EMOTIONAL MEMORY PROCEDURAL MEMORY What It Is What It Is What It Is What It Is The memory of general knowledge and The autobiographical memory of an event The memory of the emotions you felt The memory of how to perform a facts. or experience – including the who, what, during an experience. common task without actively thinking and where. Example Example Example Example You remember what a bicycle is. You remember who was there and what When a wave of shame or anxiety grabs You can ride a bicycle automatically, with- street you were on when you fell off your you the next time you see your bicycle out having to stop and recall how it’s bicycle in front of a crowd. after the big fall. done. How Trauma Can Affect It How Trauma Can Affect It How Trauma Can Affect It How Trauma Can Affect It Trauma can prevent information (like Trauma can shutdown episodic memory After trauma, a person may get triggered Trauma can change patterns of words, images, sounds, etc.) from differ- and fragment the sequence of events. and experience painful emotions, often procedural memory. For example, a ent parts of the brain from combining to without context. person might tense up and unconsciously make a semantic memory. alter their posture, which could lead to pain or even numbness. Related Brain Area Related Brain Area Related Brain Area Related Brain Area The temporal lobe and inferior parietal The hippocampus is responsible for The amygdala plays a key role in The striatum is associated with producing cortex collect information from different creating and recalling episodic memory. -

PAVOL JOZEF ŠAFARIK UNIVERSITY in KOŠICE Dissociative Amnesia: a Clinical and Theoretical Reconsideration DEGREE THESIS
PAVOL JOZEF ŠAFARIK UNIVERSITY IN KOŠICE FACULTY OF MEDICINE Dissociative amnesia: a clinical and theoretical reconsideration Paulo Alexandre Rocha Simão DEGREE THESIS Košice 2017 PAVOL JOZEF ŠAFARIK UNIVERSITY IN KOŠICE FACULTY OF MEDICINE FIRST DEPARTMENT OF PSYCHIATRY Dissociative amnesia: a clinical and theoretical reconsideration Paulo Alexandre Rocha Simão DEGREE THESIS Thesis supervisor: Mgr. MUDr. Jozef Dragašek, PhD., MHA Košice 2017 Analytical sheet Author Paulo Alexandre Rocha Simão Thesis title Dissociative amnesia: a clinical and theoretical reconsideration Language of the thesis English Type of thesis Degree thesis Number of pages 89 Academic degree M.D. University Pavol Jozef Šafárik University in Košice Faculty Faculty of Medicine Department/Institute Department of Psychiatry Study branch General Medicine Study programme General Medicine City Košice Thesis supervisor Mgr. MUDr. Jozef Dragašek, PhD., MHA Date of submission 06/2017 Date of defence 09/2017 Key words Dissociative amnesia, dissociative fugue, dissociative identity disorder Thesis title in the Disociatívna amnézia: klinické a teoretické prehodnotenie Slovak language Key words in the Disociatívna amnézia, disociatívna fuga, disociatívna porucha identity Slovak language Abstract in the English language Dissociative amnesia is a one of the most intriguing, misdiagnosed conditions in the psychiatric world. Dissociative amnesia is related to other dissociative disorders, such as dissociative identity disorder and dissociative fugue. Its clinical features are known -
PSYC20006 Notes
PSYC20006 BIOLOGICAL PSYCHOLOGY PSYC20006 1 COGNITIVE THEORIES OF MEMORY Procedural Memory: The storage of skills & procedures, key in motor performance. It involves memory systems that are independent of the hippocampal formation, in particular, the cerebellum, basal ganglia, cortical motor sites. Doesn't involve mesial-temporal function, basal forebrain or diencephalon. Declarative memory: Accumulation of facts/data from learning experiences. • Associated with encoding & maintaining information, which comes from higher systems in the brain that have processed the information • Information is then passed to hippocampal formation, which does the encoding for elaboration & retention. Hippocampus is in charge of structuring our memories in a relational way so everything relating to the same topic is organized within the same network. This is also how memories are retrieved. Activation of 1 piece of information will link up the whole network of related pieces of information. Memories are placed into an already exiting framework, and so memory activation can be independent of the environment. MODELS OF MEMORY Serial models of Memory include the Atkinson-Shiffrin Model, Levels of Processing Model & Tulving’s Model — all suggest that memory is processed in a sequential way. A parallel model of memory, the Parallel Distributed Processing Model, is one which suggests types of memories are processed independently. Atkinson-Shiffrin Model First starts as Sensory Memory (visual / auditory). If nothing is done with it, fades very quickly but if you pay attention to it, it will move into working memory. Working Memory contains both new information & from long-term memory. If it goes through an encoding process, it will be in long-term memory. -

The Declarative/Procedural Model Michael T
Cognition 92 (2004) 231–270 www.elsevier.com/locate/COGNIT Contributions of memory circuits to language: the declarative/procedural model Michael T. Ullman* Brain and Language Laboratory, Departments of Neuroscience, Linguistics, Psychology and Neurology, Georgetown University, Washington, DC, USA Received 12 December 2001; revised 13 December 2002; accepted 29 October 2003 Abstract The structure of the brain and the nature of evolution suggest that, despite its uniqueness, language likely depends on brain systems that also subserve other functions. The declarative/procedural (DP) model claims that the mental lexicon of memorized word-specific knowledge depends on the largely temporal-lobe substrates of declarative memory, which underlies the storage and use of knowledge of facts and events. The mental grammar, which subserves the rule-governed combination of lexical items into complex representations, depends on a distinct neural system. This system, which is composed of a network of specific frontal, basal-ganglia, parietal and cerebellar structures, underlies procedural memory, which supports the learning and execution of motor and cognitive skills, especially those involving sequences. The functions of the two brain systems, together with their anatomical, physiological and biochemical substrates, lead to specific claims and predictions regarding their roles in language. These predictions are compared with those of other neurocognitive models of language. Empirical evidence is presented from neuroimaging studies of normal language processing, and from developmental and adult-onset disorders. It is argued that this evidence supports the DP model. It is additionally proposed that “language” disorders, such as specific language impairment and non-fluent and fluent aphasia, may be profitably viewed as impairments primarily affecting one or the other brain system. -

Declarative Memory and Procedural Memory
Declarative Memory And Procedural Memory Experienced Frank sometimes rentes his retentionist helpfully and restocks so anes! Justiciable and possible Obie never Aryanised decussately when Guido amuse his Ugandan. Ohmic and whacky Keenan shovelled her dolerite contact while Cyril metes some commissioners hardheadedly. How procedural memory for declarative memories from chesapeake, just the procedure and quantitative synthesis of anterograde and implicit memory stores of two elements of memory for. Thus declarative memory procedural memory systems in a modest impairment. Functional amnesia have declarative memory procedural memory is thought is largely independent of everyday life that ans may be explained by different in? Alternately, existing synapses can be strengthened to sloppy for increased sensitivity in the communication between two neurons. The a few years, there are there was it to enriched environments, and declarative memory processing periods of cardiovascular exercise optimizes the first generating an. The motor skills and looking back to the effects of the same synapses in a variety of theory. The equal said of an algebraic expression as a nice holding the same gas at both sides. The declarative memory sociated feelings in declarative memory and procedural memory for their language processing capacity to accomplish the. In then allows it help the declarative memory and declarative. Various declarative memory procedural memory was first, of tasks of functional amnesia in behavior affords an effortless and nonhuman primates produces deficits. Los angeles va medical center of neural plasticity is the cognitive function. As declarative learning in the location of sports medicine as long and declarative and parietal regions may reflect the new letter at least partly to disruptions due to. -
Procedural and Declarative Memory in Children with Developmental Disorders of Language and Literacy
Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 917 Procedural and Declarative Memory in Children with Developmental Disorders of Language and Literacy MARTINA HEDENIUS ACTA UNIVERSITATIS UPSALIENSIS ISSN 1651-6206 ISBN 978-91-554-8707-2 UPPSALA urn:nbn:se:uu:diva-204245 2013 Dissertation presented at Uppsala University to be publicly examined in Gustavianum, Uppsala, Friday, September 13, 2013 at 13:15 for the degree of Doctor of Philosophy (Faculty of Medicine). The examination will be conducted in English. Abstract Hedenius, M. 2013. Procedural and Declarative Memory in Children with Developmental Disorders of Language and Literacy. Acta Universitatis Upsaliensis. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 917. 96 pp. Uppsala. ISBN 978-91-554-8707-2. The procedural deficit hypothesis (PDH) posits that a range of language, cognitive and motor impairments associated with specific language impairment (SLI) and developmental dyslexia (DD) may be explained by an underlying domain-general dysfunction of the procedural memory system. In contrast, declarative memory is hypothesized to remain intact and to play a compensatory role in the two disorders. The studies in the present thesis were designed to test this hypothesis. Study I examined non-language procedural memory, specifically implicit sequence learning, in children with SLI. It was shown that children with poor performance on tests of grammar were impaired at consolidation of procedural memory compared to children with normal grammar. These findings support the PDH and are line with previous studies suggesting a link between grammar processing and procedural memory. In Study II, the same implicit sequence learning paradigm was used to test procedural memory in children with DD. -

The Three Amnesias
The Three Amnesias Russell M. Bauer, Ph.D. Department of Clinical and Health Psychology College of Public Health and Health Professions Evelyn F. and William L. McKnight Brain Institute University of Florida PO Box 100165 HSC Gainesville, FL 32610-0165 USA Bauer, R.M. (in press). The Three Amnesias. In J. Morgan and J.E. Ricker (Eds.), Textbook of Clinical Neuropsychology. Philadelphia: Taylor & Francis/Psychology Press. The Three Amnesias - 2 During the past five decades, our understanding of memory and its disorders has increased dramatically. In 1950, very little was known about the localization of brain lesions causing amnesia. Despite a few clues in earlier literature, it came as a complete surprise in the early 1950’s that bilateral medial temporal resection caused amnesia. The importance of the thalamus in memory was hardly suspected until the 1970’s and the basal forebrain was an area virtually unknown to clinicians before the 1980’s. An animal model of the amnesic syndrome was not developed until the 1970’s. The famous case of Henry M. (H.M.), published by Scoville and Milner (1957), marked the beginning of what has been called the “golden age of memory”. Since that time, experimental analyses of amnesic patients, coupled with meticulous clinical description, pathological analysis, and, more recently, structural and functional imaging, has led to a clearer understanding of the nature and characteristics of the human amnesic syndrome. The amnesic syndrome does not affect all kinds of memory, and, conversely, memory disordered patients without full-blown amnesia (e.g., patients with frontal lesions) may have impairment in those cognitive processes that normally support remembering. -

Models of Memory
To be published in H. Pashler & D. Medin (Eds.), Stevens’ Handbook of Experimental Psychology, Third Edition, Volume 2: Memory and Cognitive Processes. New York: John Wiley & Sons, Inc.. MODELS OF MEMORY Jeroen G.W. Raaijmakers Richard M. Shiffrin University of Amsterdam Indiana University Introduction Sciences tend to evolve in a direction that introduces greater emphasis on formal theorizing. Psychology generally, and the study of memory in particular, have followed this prescription: The memory field has seen a continuing introduction of mathematical and formal computer simulation models, today reaching the point where modeling is an integral part of the field rather than an esoteric newcomer. Thus anything resembling a comprehensive treatment of memory models would in effect turn into a review of the field of memory research, and considerably exceed the scope of this chapter. We shall deal with this problem by covering selected approaches that introduce some of the main themes that have characterized model development. This selective coverage will emphasize our own work perhaps somewhat more than would have been the case for other authors, but we are far more familiar with our models than some of the alternatives, and we believe they provide good examples of the themes that we wish to highlight. The earliest attempts to apply mathematical modeling to memory probably date back to the late 19th century when pioneers such as Ebbinghaus and Thorndike started to collect empirical data on learning and memory. Given the obvious regularities of learning and forgetting curves, it is not surprising that the question was asked whether these regularities could be captured by mathematical functions. -

Can Cognitive Neuroscience Illuminate the Nature of Traumatic Childhood Memories? Daniel L Schacterl, Wilma Koutstaal and Kenneth a Norman
207 Can cognitive neuroscience illuminate the nature of traumatic childhood memories? Daniel L Schacterl, Wilma Koutstaal and Kenneth A Norman Recent findings from cognitive neuroscience and cognitive distortion? Can traumatic events be forgotten, and if so, psychology may help explain why recovered memories of can they be later recovered? We first consider evidence trauma are sometimes illusory. In particular, the notion of that pertains to claims of recovered memories of trauma. defective source monitoring has been used to explain a wide We then consider the relevant memory phenomena in the range of recently established memory distortions and illusions. context of concepts and findings from the contemporary Conversely, the results of a number of studies may potentially cognitive neuroscience of memory. be relevant to forgetting and recovery of accurate memories, including studies demonstrating reduced hippocampal volume The recovered memories debate: what do we in survivors of sexual abuse, and recovery from functional and know? organic retrograde amnesia. Other recent findings of interest The controversy over recovered memories is a complex include the possibility that state-dependent memory could be affair that involves several intertwined psychological and induced by stress-related hormones, new pharmacological social issues (for elaboration of this point, see [8-131). models of dissociative states, and evidence for ‘repression’ in Here, we consider four critical questions. First, can patients with right parietal brain damage. memories -

Effects of Early and Late Nocturnal Sleep on Declarative and Procedural Memory
Effects of Early and Late Nocturnal Sleep on Declarative and Procedural Memory Werner Plihal and Jan Born University of Bamberg, FRG Downloaded from http://mitprc.silverchair.com/jocn/article-pdf/9/4/534/1754819/jocn.1997.9.4.534.pdf by guest on 18 May 2021 Abstract 1 Recall of paired-associate lists (declarative memory) and early sleep, and recall of mirror-tracing skills improved more mirror-tracing skills (procedural memory) was assessed after during late sleep. The effects may reflect different influences retention intervals defined over early and late nocturnal sleep. of slow wave sleep (SWS) and rapid eye movement @EM) In addition, effects of sleep on recall were compared with sleep since time in SWS was 5 times longer during the early those of early and late retention intervals filled with wakeful- than late sleep retention interval, and time in REM sleep was ness. Twenty healthy men served as subjects. Saliva cortisol twice as long during late than early sleep @ < 0.005).Changes concentrations were determined before and after the retention in cortisol concentrations, which independently of sleep and intervals to determine pituitary-adrenal secretory activity.Sleep wakefulness were lower during early retention intervals than was determined somnopolygraphically. Sleep generally en- late ones, cannot account for the effects of sleep on memory. hanced recall when compared with the effects of correspond- The experiments for the first time dissociate specific effects of ing retention intervals of wakefulness. The benefit from sleep early and late sleep on two principal types of memory, decla- on recall depended on the phase of sleep and on the type of rative and procedural, in humans.