Increased Production of Lysozyme Associated with Bacterial
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Antimicrobial Activity of Cathelicidin Peptides and Defensin Against Oral Yeast and Bacteria JH Wong, TB Ng *, RCF Cheung, X Dan, YS Chan, M Hui
RESEARCH FUND FOR THE CONTROL OF INFECTIOUS DISEASES Antimicrobial activity of cathelicidin peptides and defensin against oral yeast and bacteria JH Wong, TB Ng *, RCF Cheung, X Dan, YS Chan, M Hui KEY MESSAGES Mycosphaerella arachidicola, Saccharomyces cerevisiae and C albicans with an IC value of 1. Human cathelicidin LL37 and its fragments 50 3.9, 4.0, and 8.4 μM, respectively. The peptide LL13-37 and LL17-32 were equipotent in increased fungal membrane permeability. inhibiting growth of Candida albicans. 6. LL37 did not show obvious antibacterial activity 2. LL13-37 permeabilised the membrane of yeast below a concentration of 64 μM and its fragments and hyphal forms of C albicans and adversely did not show antibacterial activity below a affected mitochondria. concentration of 128 μM. Pole bean defensin 3. Reactive oxygen species was detectable in the exerted antibacterial activity on some bacterial yeast form after LL13-37 treatment but not in species. untreated cells suggesting that the increased membrane permeability caused by LL13-37 might also lead to uptake of the peptide, which Hong Kong Med J 2016;22(Suppl 7):S37-40 might have some intracellular targets. RFCID project number: 09080432 4. LL37 and its fragments also showed antifungal 1 JH Wong, 1 TB Ng, 1 RCF Cheung, 1 X Dan, 1 YS Chan, 2 M Hui activity against C krusei, and C tropicalis. 5. A 5447-Da antifungal peptide with sequence The Chinese University of Hong Kong: 1 School of Biomedical Sciences homology to plant defensins was purified from 2 Department of Microbiology king pole beans by chromatography on Q- Sepharose and FPLC-gel filtration on Superdex * Principal applicant and corresponding author: 75. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
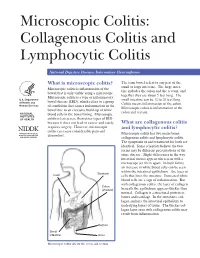
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -
Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #15 Seymour Katz, M.D., Series Editor Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease by Noel R. Fajardo and Darrell S. Pardi INTRODUCTION The prevalence of IBD, on the other hand, is higher nflammatory disorders of the intestines can be than microscopic colitis, reflecting the younger age of divided into those with macroscopic mucosal onset in patients with IBD. Ichanges (the traditional inflammatory bowel dis- In North America, the incidence of microscopic eases: ulcerative colitis and Crohn’s disease) and those colitis was 0.8/100,000 person-years from 1985 to with primarily microscopic changes. 1989, and this increased significantly to19.1/100,000 Microscopic colitis is a chronic diarrheal condi- from 1998 to 2001 (1). The incidence of collagenous tion that is separated into two main subtypes: collage- colitis and lymphocytic colitis was 5.1 and 9.8/100,000 nous colitis and lymphocytic colitis. These two condi- person-years, and the prevalence was 36 and tions have similar clinical and histologic features, but 64/100,000 persons, respectively (1). In Europe, the are distinguished by the presence or absence of a incidence of collagenous and lymphocytic colitis ranges thickened subepithelial collagen band. Inflammatory from 0.6 to 5.2/100,000 person-years with a prevalence bowel disease (IBD) is traditionally separated into two between 10 to 16/100,000 persons (2). The reason for distinct clinical entities: Crohn’s disease and ulcera- the significantly higher incidence and prevalence of MC tive colitis. Although there is considerable symptom in North America compared with Europe is not known, overlap between these diseases, there are several fea- though increasing recognition may play a role. -

Human Peptides -Defensin-1 and -5 Inhibit Pertussis Toxin
toxins Article Human Peptides α-Defensin-1 and -5 Inhibit Pertussis Toxin Carolin Kling 1, Arto T. Pulliainen 2, Holger Barth 1 and Katharina Ernst 1,* 1 Institute of Pharmacology and Toxicology, Ulm University Medical Center, 89081 Ulm, Germany; [email protected] (C.K.); [email protected] (H.B.) 2 Institute of Biomedicine, Research Unit for Infection and Immunity, University of Turku, FI-20520 Turku, Finland; arto.pulliainen@utu.fi * Correspondence: [email protected] Abstract: Bordetella pertussis causes the severe childhood disease whooping cough, by releasing several toxins, including pertussis toxin (PT) as a major virulence factor. PT is an AB5-type toxin, and consists of the enzymatic A-subunit PTS1 and five B-subunits, which facilitate binding to cells and transport of PTS1 into the cytosol. PTS1 ADP-ribosylates α-subunits of inhibitory G-proteins (Gαi) in the cytosol, which leads to disturbed cAMP signaling. Since PT is crucial for causing severe courses of disease, our aim is to identify new inhibitors against PT, to provide starting points for novel therapeutic approaches. Here, we investigated the effect of human antimicrobial peptides of the defensin family on PT. We demonstrated that PTS1 enzyme activity in vitro was inhibited by α-defensin-1 and -5, but not β-defensin-1. The amount of ADP-ribosylated Gαi was significantly reduced in PT-treated cells, in the presence of α-defensin-1 and -5. Moreover, both α-defensins decreased PT-mediated effects on cAMP signaling in the living cell-based interference in the Gαi- mediated signal transduction (iGIST) assay. -

Innate Immune System of Mallards (Anas Platyrhynchos)
Anu Helin Linnaeus University Dissertations No 376/2020 Anu Helin Eco-immunological studies of innate immunity in Mallards immunity innate of studies Eco-immunological List of papers Eco-immunological studies of innate I. Chapman, J.R., Hellgren, O., Helin, A.S., Kraus, R.H.S., Cromie, R.L., immunity in Mallards (ANAS PLATYRHYNCHOS) Waldenström, J. (2016). The evolution of innate immune genes: purifying and balancing selection on β-defensins in waterfowl. Molecular Biology and Evolution. 33(12): 3075-3087. doi:10.1093/molbev/msw167 II. Helin, A.S., Chapman, J.R., Tolf, C., Andersson, H.S., Waldenström, J. From genes to function: variation in antimicrobial activity of avian β-defensin peptides from mallards. Manuscript III. Helin, A.S., Chapman, J.R., Tolf, C., Aarts, L., Bususu, I., Rosengren, K.J., Andersson, H.S., Waldenström, J. Relation between structure and function of three AvBD3b variants from mallard (Anas platyrhynchos). Manuscript I V. Chapman, J.R., Helin, A.S., Wille, M., Atterby, C., Järhult, J., Fridlund, J.S., Waldenström, J. (2016). A panel of Stably Expressed Reference genes for Real-Time qPCR Gene Expression Studies of Mallards (Anas platyrhynchos). PLoS One. 11(2): e0149454. doi:10.1371/journal. pone.0149454 V. Helin, A.S., Wille, M., Atterby, C., Järhult, J., Waldenström, J., Chapman, J.R. (2018). A rapid and transient innate immune response to avian influenza infection in mallards (Anas platyrhynchos). Molecular Immunology. 95: 64-72. doi:10.1016/j.molimm.2018.01.012 (A VI. Helin, A.S., Wille, M., Atterby, C., Järhult, J., Waldenström, J., Chapman, N A S J.R. -

Antimicrobial Peptides in Reptiles
Pharmaceuticals 2014, 7, 723-753; doi:10.3390/ph7060723 OPEN ACCESS pharmaceuticals ISSN 1424-8247 www.mdpi.com/journal/pharmaceuticals Review Antimicrobial Peptides in Reptiles Monique L. van Hoek National Center for Biodefense and Infectious Diseases, and School of Systems Biology, George Mason University, MS1H8, 10910 University Blvd, Manassas, VA 20110, USA; E-Mail: [email protected]; Tel.: +1-703-993-4273; Fax: +1-703-993-7019. Received: 6 March 2014; in revised form: 9 May 2014 / Accepted: 12 May 2014 / Published: 10 June 2014 Abstract: Reptiles are among the oldest known amniotes and are highly diverse in their morphology and ecological niches. These animals have an evolutionarily ancient innate-immune system that is of great interest to scientists trying to identify new and useful antimicrobial peptides. Significant work in the last decade in the fields of biochemistry, proteomics and genomics has begun to reveal the complexity of reptilian antimicrobial peptides. Here, the current knowledge about antimicrobial peptides in reptiles is reviewed, with specific examples in each of the four orders: Testudines (turtles and tortosises), Sphenodontia (tuataras), Squamata (snakes and lizards), and Crocodilia (crocodilans). Examples are presented of the major classes of antimicrobial peptides expressed by reptiles including defensins, cathelicidins, liver-expressed peptides (hepcidin and LEAP-2), lysozyme, crotamine, and others. Some of these peptides have been identified and tested for their antibacterial or antiviral activity; others are only predicted as possible genes from genomic sequencing. Bioinformatic analysis of the reptile genomes is presented, revealing many predicted candidate antimicrobial peptides genes across this diverse class. The study of how these ancient creatures use antimicrobial peptides within their innate immune systems may reveal new understandings of our mammalian innate immune system and may also provide new and powerful antimicrobial peptides as scaffolds for potential therapeutic development. -
Familial Occurrence of Lymphocytic Colitis
BRIEF COMMUNICATION Familial occurrence of lymphocytic colitis Hugh J Freeman MD HJ Freeman. Familial occurrence of lymphocytic colitis. Can J Occurrence familiale de la colite Gastroenterol 2001;15(11):757-760. The familial occurrence lymphocytaire of lymphocytic colitis in a female parent and her two female children is reported. No other genetically based disorder, includ- RÉSUMÉ : On fait ici état de l’occurrence familiale de la colite lym- ing celiac disease, was evident. For both children, the age of phocytaire chez une patiente et ses deux filles. Aucune autre maladie diagnosis was more than two decades younger than the age of d’origine génétique, comme la maladie cæliaque, ne s’est manifestée. recognition of disease in the parent, and some clinical features, Pour les deux enfants, le diagnostic a été posé plus d’une vingtaine d’an- including the requirement for pharmacological agents in both nées avant l’âge qu’avait la mère au moment de son diagnostic et cer- taines caractéristiques cliniques, dont le traitement pharmacologique children, suggested that their disease severity was more signifi- chez les deux enfants, donnent à penser que leur maladie est plus grave cant than that of the involved parent. These characteristics of a que chez le parent atteint. Ces caractéristiques de la maladie familiale familial disease have been previously reported and labelled ont déjà été mentionnées et ont été appelées "anticipation génétique" ‘genetic anticipation’ in some monogenetic forms of neurologi- dans le cas de certaines formes monogénétiques de maladies neu- cal disease, as well as in other types of inflammatory bowel dis- rologiques, de même que dans d’autres types de maladies inflammatoires eases, including Crohn’s disease. -

The Unusual Resistance of Avian Defensin
The unusual resistance of avian defensin AvBD7 to proteolytic enzymes preserves its antibacterial activity Geoffrey Bailleul, Amanda Kravtzoff, Alix Joulin-Giet, Fabien Lecaille, Valérie Labas, Hervé Meudal, Karine Loth, Ana-Paula Teixeira-Mechin, Florence B. Gilbert, Laurent Coquet, et al. To cite this version: Geoffrey Bailleul, Amanda Kravtzoff, Alix Joulin-Giet, Fabien Lecaille, Valérie Labas, et al..The unusual resistance of avian defensin AvBD7 to proteolytic enzymes preserves its antibacterial activity. PLoS ONE, Public Library of Science, 2016, 11 (8), pp.1-20. 10.1371/journal.pone.0161573. hal- 01594888 HAL Id: hal-01594888 https://hal.archives-ouvertes.fr/hal-01594888 Submitted on 26 Sep 2017 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License RESEARCH ARTICLE The Unusual Resistance of Avian Defensin AvBD7 to Proteolytic Enzymes Preserves Its Antibacterial Activity Geoffrey Bailleul1, Amanda Kravtzoff2, Alix Joulin-Giet1, Fabien Lecaille2, Valérie Labas3, Hervé Meudal4, -

Vitamin D-Cathelicidin Axis: at the Crossroads Between Protective Immunity and Pathological Inflammation During Infection
Immune Netw. 2020 Apr;20(2):e12 https://doi.org/10.4110/in.2020.20.e12 pISSN 1598-2629·eISSN 2092-6685 Review Article Vitamin D-Cathelicidin Axis: at the Crossroads between Protective Immunity and Pathological Inflammation during Infection Chaeuk Chung 1, Prashanta Silwal 2,3, Insoo Kim2,3, Robert L. Modlin 4,5, Eun-Kyeong Jo 2,3,6,* 1Division of Pulmonary and Critical Care, Department of Internal Medicine, Chungnam National University School of Medicine, Daejeon 35015, Korea Received: Oct 27, 2019 2Infection Control Convergence Research Center, Chungnam National University School of Medicine, Revised: Jan 28, 2020 Daejeon 35015, Korea Accepted: Jan 30, 2020 3Department of Microbiology, Chungnam National University School of Medicine, Daejeon 35015, Korea 4Division of Dermatology, Department of Medicine, David Geffen School of Medicine at the University of *Correspondence to California, Los Angeles, Los Angeles, CA 90095, USA Eun-Kyeong Jo 5Department of Microbiology, Immunology and Molecular Genetics, University of California, Los Angeles, Department of Microbiology, Chungnam Los Angeles, CA 90095, USA National University School of Medicine, 282 6Department of Medical Science, Chungnam National University School of Medicine, Daejeon 35015, Korea Munhwa-ro, Jung-gu, Daejeon 35015, Korea. E-mail: [email protected] Copyright © 2020. The Korean Association of ABSTRACT Immunologists This is an Open Access article distributed Vitamin D signaling plays an essential role in innate defense against intracellular under the terms of the Creative Commons microorganisms via the generation of the antimicrobial protein cathelicidin. In addition Attribution Non-Commercial License (https:// to directly binding to and killing a range of pathogens, cathelicidin acts as a secondary creativecommons.org/licenses/by-nc/4.0/) messenger driving vitamin D-mediated inflammation during infection. -

The Human Cathelicidin LL-37 — a Pore-Forming Antibacterial Peptide and Host-Cell Modulator☆
Biochimica et Biophysica Acta 1858 (2016) 546–566 Contents lists available at ScienceDirect Biochimica et Biophysica Acta journal homepage: www.elsevier.com/locate/bbamem The human cathelicidin LL-37 — A pore-forming antibacterial peptide and host-cell modulator☆ Daniela Xhindoli, Sabrina Pacor, Monica Benincasa, Marco Scocchi, Renato Gennaro, Alessandro Tossi ⁎ Department of Life Sciences, University of Trieste, via Giorgeri 5, 34127 Trieste, Italy article info abstract Article history: The human cathelicidin hCAP18/LL-37 has become a paradigm for the pleiotropic roles of peptides in host de- Received 7 August 2015 fence. It has a remarkably wide functional repertoire that includes direct antimicrobial activities against various Received in revised form 30 October 2015 types of microorganisms, the role of ‘alarmin’ that helps to orchestrate the immune response to infection, the Accepted 5 November 2015 capacity to locally modulate inflammation both enhancing it to aid in combating infection and limiting it to pre- Available online 10 November 2015 vent damage to infected tissues, the promotion of angiogenesis and wound healing, and possibly also the elimi- Keywords: nation of abnormal cells. LL-37 manages to carry out all its reported activities with a small and simple, Cathelicidin amphipathic, helical structure. In this review we consider how different aspects of its primary and secondary LL-37 structures, as well as its marked tendency to form oligomers under physiological solution conditions and then hCAP-18 bind to molecular surfaces as such, explain some of its cytotoxic and immunomodulatory effects. We consider CRAMP its modes of interaction with bacterial membranes and capacity to act as a pore-forming toxin directed by our Host defence peptide organism against bacterial cells, contrasting this with the mode of action of related peptides from other species. -

Avian Antimicrobial Host Defense Peptides: from Biology to Therapeutic Applications
Pharmaceuticals 2014, 7, 220-247; doi:10.3390/ph7030220 OPEN ACCESS pharmaceuticals ISSN 1424-8247 www.mdpi.com/journal/pharmaceuticals Review Avian Antimicrobial Host Defense Peptides: From Biology to Therapeutic Applications Guolong Zhang 1,2,3,* and Lakshmi T. Sunkara 1 1 Department of Animal Science, Oklahoma State University, Stillwater, OK 74078, USA 2 Department of Biochemistry and Molecular Biology, Oklahoma State University, Stillwater, OK 74078, USA 3 Department of Physiological Sciences, Oklahoma State University, Stillwater, OK 74078, USA * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +1-405-744-6619; Fax: +1-405-744-7390. Received: 6 February 2014; in revised form: 18 February 2014 / Accepted: 19 February 2014 / Published: 27 February 2014 Abstract: Host defense peptides (HDPs) are an important first line of defense with antimicrobial and immunomoduatory properties. Because they act on the microbial membranes or host immune cells, HDPs pose a low risk of triggering microbial resistance and therefore, are being actively investigated as a novel class of antimicrobials and vaccine adjuvants. Cathelicidins and β-defensins are two major families of HDPs in avian species. More than a dozen HDPs exist in birds, with the genes in each HDP family clustered in a single chromosomal segment, apparently as a result of gene duplication and diversification. In contrast to their mammalian counterparts that adopt various spatial conformations, mature avian cathelicidins are mostly α-helical. Avian β-defensins, on the other hand, adopt triple-stranded β-sheet structures similar to their mammalian relatives. Besides classical β-defensins, a group of avian-specific β-defensin-related peptides, namely ovodefensins, exist with a different six-cysteine motif. -

Plasma Elafin, Cathelicidin, and Α-Defensins Are Increased in Paediatric Inflammatory Crohn’S Disease and Reflect Disease Location
Research letter Gastroenterology Plasma elafin, cathelicidin, and α-defensins are increased in paediatric inflammatory Crohn’s disease and reflect disease location Andrzej Wędrychowicz1, Przemysław Tomasik2, Kinga Kowalska-Duplaga1, Stanisław Pieczarkowski1, Krzysztof Fyderek1 1Department of Paediatrics, Gastroenterology, and Nutrition, Jagiellonian University Corresponding author: Medical College, Krakow, Poland Prof. Andrzej Wędrychowicz 2Department of Clinical Biochemistry, Jagiellonian University Medical College, Krakow, Department of Paediatrics, Poland Gastroenterology, and Nutrition Submitted: 10 April 2021, Accepted: 1 June 2021 Jagiellonian University Online publication: 11 June 2021 Medical College Krakow, Poland Arch Med Sci 2021; 17 (4): 1114–1117 Phone: +48 12 3339330 DOI: https://doi.org/10.5114/aoms/138349 E-mail: Copyright © 2021 Termedia & Banach [email protected] Abstract Introduction: The aim of our study was to assess antimicrobial peptides in children with Crohn’s disease (CD). Methods: Plasma elafin, cathelicidin, and α- and β-defensins were assessed in 35 children with CD using immunoassays. Phenotype and location of CD were assessed based on the results of endoscopic and radiological studies. Results: We found increased elafin, cathelicidin, and α-defensins in children with inflammatory phenotype as compared to stricturing and penetrating phenotypes of CD. Additionally, we found increased elafin and cathelicidin in colonic location and α-defensins in ileal CD locations. Conclusions: Assessing antimicrobial