View to Better Reveal Trends Within the Data
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supplementary Information Changes in the Plasma Proteome At
Supplementary Information Changes in the plasma proteome at asymptomatic and symptomatic stages of autosomal dominant Alzheimer’s disease Julia Muenchhoff1, Anne Poljak1,2,3, Anbupalam Thalamuthu1, Veer B. Gupta4,5, Pratishtha Chatterjee4,5,6, Mark Raftery2, Colin L. Masters7, John C. Morris8,9,10, Randall J. Bateman8,9, Anne M. Fagan8,9, Ralph N. Martins4,5,6, Perminder S. Sachdev1,11,* Supplementary Figure S1. Ratios of proteins differentially abundant in asymptomatic carriers of PSEN1 and APP Dutch mutations. Mean ratios and standard deviations of plasma proteins from asymptomatic PSEN1 mutation carriers (PSEN1) and APP Dutch mutation carriers (APP) relative to reference masterpool as quantified by iTRAQ. Ratios that significantly differed are marked with asterisks (* p < 0.05; ** p < 0.01). C4A, complement C4-A; AZGP1, zinc-α-2-glycoprotein; HPX, hemopexin; PGLYPR2, N-acetylmuramoyl-L-alanine amidase isoform 2; α2AP, α-2-antiplasmin; APOL1, apolipoprotein L1; C1 inhibitor, plasma protease C1 inhibitor; ITIH2, inter-α-trypsin inhibitor heavy chain H2. 2 A) ADAD)CSF) ADAD)plasma) B) ADAD)CSF) ADAD)plasma) (Ringman)et)al)2015)) (current)study)) (Ringman)et)al)2015)) (current)study)) ATRN↓,%%AHSG↑% 32028% 49% %%%%%%%%HC2↑,%%ApoM↓% 24367% 31% 10083%% %%%%TBG↑,%%LUM↑% 24256% ApoC1↓↑% 16565% %%AMBP↑% 11738%%% SERPINA3↓↑% 24373% C6↓↑% ITIH2% 10574%% %%%%%%%CPN2↓%% ↓↑% %%%%%TTR↑% 11977% 10970% %SERPINF2↓↑% CFH↓% C5↑% CP↓↑% 16566% 11412%% 10127%% %%ITIH4↓↑% SerpinG1↓% 11967% %%ORM1↓↑% SerpinC1↓% 10612% %%%A1BG↑%%% %%%%FN1↓% 11461% %%%%ITIH1↑% C3↓↑% 11027% 19325% 10395%% %%%%%%HPR↓↑% HRG↓% %%% 13814%% 10338%% %%% %ApoA1 % %%%%%%%%%GSN↑% ↓↑ %%%%%%%%%%%%ApoD↓% 11385% C4BPA↓↑% 18976%% %%%%%%%%%%%%%%%%%ApoJ↓↑% 23266%%%% %%%%%%%%%%%%%%%%%%%%%%ApoA2↓↑% %%%%%%%%%%%%%%%%%%%%%%%%%%%%A2M↓↑% IGHM↑,%%GC↓↑,%%ApoB↓↑% 13769% % FGA↓↑,%%FGB↓↑,%%FGG↓↑% AFM↓↑,%%CFB↓↑,%% 19143%% ApoH↓↑,%%C4BPA↓↑% ApoA4↓↑%%% LOAD/MCI)plasma) LOAD/MCI)plasma) LOAD/MCI)plasma) LOAD/MCI)plasma) (Song)et)al)2014)) (Muenchhoff)et)al)2015)) (Song)et)al)2014)) (Muenchhoff)et)al)2015)) Supplementary Figure S2. -

Plasma Kallikrein Activation and Inhibition During Typhoid Fever
Plasma Kallikrein Activation and Inhibition during Typhoid Fever Robert W. Colman, … , Cheryl F. Scott, Robert H. Gilman J Clin Invest. 1978;61(2):287-296. https://doi.org/10.1172/JCI108938. Research Article As an ancillary part of a typhoid fever vaccine study, 10 healthy adult male volunteers (nonimmunized controls) were serially bled 6 days before to 30 days after ingesting 105Salmonella typhi organisms. Five persons developed typhoid fever 6-10 days after challenge, while five remained well. During the febrile illness, significant changes (P < 0.05) in the following hematological parameters were measured: a rise in α1-antitrypsin antigen concentration and high molecular weight kininogen clotting activity; a progressive decrease of platelet count (to 60% of the predisease state), functional prekallikrein (55%) and kallikrein inhibitor (47%) with a nadir reached on day 5 of the fever and a subsequent overshoot during convalescence. Despite the drop in functional prekallikrein and kallikrein inhibitor, there was no change in factor XII clotting activity or antigenic concentrations of prekallikrein and the kallikrein inhibitors, C1 esterase inhibitor (C1-̄ INH) and α2-macroglobulin. Plasma from febrile patients subjected to immunoelectrophoresis and crossed immunoelectrophoresis contained a new complex displaying antigenic characteristics of both prekallikrein and C1-̄ INH; the α2-macroglobulin, antithrombin III, and α1-antitrypsin immunoprecipitates were unchanged. Plasma drawn from infected-well subjects showed no significant change in these components of the kinin generating system. The finding of a reduction in functional prekallikrein and kallikrein inhibitor (C1-̄ INH) and the formation of a kallikrein C1-̄ INH complex is consistent with prekallikrein activation in typhoid fever. -

Remote Ischemic Preconditioning (RIPC) Modifies Plasma Proteome in Humans
Remote Ischemic Preconditioning (RIPC) Modifies Plasma Proteome in Humans Michele Hepponstall1,2,3,4, Vera Ignjatovic1,3, Steve Binos4, Paul Monagle1,3, Bryn Jones1,2, Michael H. H. Cheung1,2,3, Yves d’Udekem1,2, Igor E. Konstantinov1,2,3* 1 Haematology Research, Murdoch Childrens Research Institute; Melbourne, Victoria, Australia, 2 Cardiac Surgery Unit and Cardiology, Royal Children’s Hospital; Melbourne, Victoria, Australia, 3 Department of Paediatrics, The University of Melbourne; Melbourne, Victoria, Australia, 4 Bioscience Research Division, Department of Primary Industries, Melbourne, Victoria, Australia Abstract Remote Ischemic Preconditioning (RIPC) induced by brief episodes of ischemia of the limb protects against multi-organ damage by ischemia-reperfusion (IR). Although it has been demonstrated that RIPC affects gene expression, the proteomic response to RIPC has not been determined. This study aimed to examine RIPC induced changes in the plasma proteome. Five healthy adult volunteers had 4 cycles of 5 min ischemia alternating with 5 min reperfusion of the forearm. Blood samples were taken from the ipsilateral arm prior to first ischaemia, immediately after each episode of ischemia as well as, at 15 min and 24 h after the last episode of ischemia. Plasma samples from five individuals were analysed using two complementary techniques. Individual samples were analysed using 2Dimensional Difference in gel electrophoresis (2D DIGE) and mass spectrometry (MS). Pooled samples for each of the time-points underwent trypsin digestion and peptides generated were analysed in triplicate using Liquid Chromatography and MS (LC-MS). Six proteins changed in response to RIPC using 2D DIGE analysis, while 48 proteins were found to be differentially regulated using LC-MS. -

Mechanism of Interleukin-1- and Tumor Necrosis Factor Α-Dependent Regulation of the Α1-Antichymotrypsin Gene in Human Astrocyt
The Journal of Neuroscience, October 15, 2000, 20(20):7510–7516 Mechanism of Interleukin-1- and Tumor Necrosis Factor ␣- ␣ Dependent Regulation of the 1-Antichymotrypsin Gene in Human Astrocytes Tomasz Kordula,1 Marcin Bugno,1 Russell E. Rydel,2 and James Travis3 1Institute of Molecular Biology, Jagiellonian University, 31-120 Krako´ w, Poland, 2Elan Pharmaceuticals, South San Francisco, California 94080, and 3Department of Biochemistry and Molecular Biology, The University of Georgia, Athens, Georgia 30602 ␣ The expression of 1-antichymotrypsin (ACT) is significantly en- which bind nuclear factor kB (NF-kB) and one that binds activat- hanced in affected brain regions in Alzheimer’s disease. This ing protein 1 (AP-1). All of these elements contribute to the full serine proteinase inhibitor specifically colocalizes with filamen- responsiveness of the ACT gene to both cytokines, as deter- tous -amyloid deposits and recently has been shown to influ- mined by deletion and mutational analysis. The 5Ј NF-kB high- ence both formation and destabilization of -amyloid fibrils. In affinity binding site and AP-1 element contribute most to the the brain, ACT is expressed in astrocytes, and interleukin-1 (IL-1), enhancement of gene transcription in response to TNF and IL-1. tumor necrosis factor ␣ (TNF), oncostatin M (OSM), and IL-6/ In addition, we demonstrate that the 5Ј untranslated region of the soluble IL-6 receptor complexes control synthesis of this inhibi- ACT mRNA does not contribute to cytokine-mediated activation. tor. Here, we characterize a molecular mechanism responsible Finally, we find that overexpression of the NF-kB inhibitor (IkB) for both IL-1 and TNF-induced expression of ACT gene in astro- totally inhibits any activation mediated by the newly identified cytes. -
Pancancer Progression Human Vjune2017
Gene Symbol Accession Alias/Prev Symbol Official Full Name AAMP NM_001087.3 - angio-associated, migratory cell protein ABI3BP NM_015429.3 NESHBP|TARSH ABI family, member 3 (NESH) binding protein ACHE NM_000665.3 ACEE|ARACHE|N-ACHE|YT acetylcholinesterase ACTG2 NM_001615.3 ACT|ACTA3|ACTE|ACTL3|ACTSG actin, gamma 2, smooth muscle, enteric ACVR1 NM_001105.2 ACTRI|ACVR1A|ACVRLK2|ALK2|FOP|SKR1|TSRI activin A receptor, type I ACVR1C NM_145259.2 ACVRLK7|ALK7 activin A receptor, type IC ACVRL1 NM_000020.1 ACVRLK1|ALK-1|ALK1|HHT|HHT2|ORW2|SKR3|TSR-I activin A receptor type II-like 1 ADAM15 NM_207195.1 MDC15 ADAM metallopeptidase domain 15 ADAM17 NM_003183.4 ADAM18|CD156B|CSVP|NISBD|TACE ADAM metallopeptidase domain 17 ADAM28 NM_014265.4 ADAM 28|ADAM23|MDC-L|MDC-Lm|MDC-Ls|MDCL|eMDC II|eMDCII ADAM metallopeptidase domain 28 ADAM8 NM_001109.4 CD156|MS2 ADAM metallopeptidase domain 8 ADAM9 NM_001005845.1 CORD9|MCMP|MDC9|Mltng ADAM metallopeptidase domain 9 ADAMTS1 NM_006988.3 C3-C5|METH1 ADAM metallopeptidase with thrombospondin type 1 motif, 1 ADAMTS12 NM_030955.2 PRO4389 ADAM metallopeptidase with thrombospondin type 1 motif, 12 ADAMTS8 NM_007037.4 ADAM-TS8|METH2 ADAM metallopeptidase with thrombospondin type 1 motif, 8 ADAP1 NM_006869.2 CENTA1|GCS1L|p42IP4 ArfGAP with dual PH domains 1 ADD1 NM_001119.4 ADDA adducin 1 (alpha) ADM2 NM_001253845.1 AM2|dJ579N16.4 adrenomedullin 2 ADRA2B NM_000682.4 ADRA2L1|ADRA2RL1|ADRARL1|ALPHA2BAR|alpha-2BAR adrenoceptor alpha 2B AEBP1 NM_001129.3 ACLP AE binding protein 1 AGGF1 NM_018046.3 GPATC7|GPATCH7|HSU84971|HUS84971|VG5Q -
Supporting Information for Proteomics DOI 10.1002/Prca.200780101
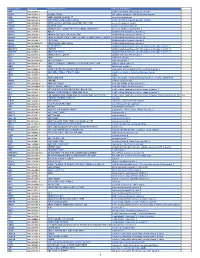
Supporting Information for Proteomics DOI 10.1002/prca.200780101 Paul Cutler, Emma L. Akuffo, Wanda M. Bodnar, Deborah M. Briggs, John B. Davis, Christine M. Debouck, Steven M. Fox, Rachel A. Gibson, Darren A. Gormley, Joanna D. Holbrook, A. Jacqueline Hunter, Emma E. Kinsey, Rabinder Prinjha, Jill C. Richardson, Allen D. Roses, Marjorie A. Smith, Nikos Tsokanas, David R. Will, Wen Wu, John W. Yates and Israel S. Gloger Proteomic identification and early validation of complement 1 inhibitor and pigment epithelium-derived factor: Two novel biomarkers of Alzheimer’s disease in human plasma ª 2007 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim www.clinical.proteomics-journal.com Supplementary Table 1: Complete list of proteins identified from spots derived from 2D gel analysis of human plasma. Each protein was observed to be in a spot showing altered expression between Alzheimer’s disease and matched control by statistical methods as described in the Methods section. Each protein is identified by the gene description and the HUGO gene symbol. The number of “changing” spots in which this protein was observed is also given. HUGO Human Gene Number of Gene Description Symbol Spots alpha-1-B glycoprotein; A1BG 5 alpha-2-macroglobulin A2M 7 afamin; AFM 1 angiotensinogen (serpin peptidase inhibitor, clade A, member 8) AGT 4 alpha-2-HS-glycoprotein AHSG 3 albumin ALB 90 alpha-1-microglobulin/bikunin precursor; AMBP 1 annexin A1 ANXA1 1 amyloid P component, serum APCS 3 apolipoprotein A-I APOA1 14 apolipoprotein A-IV APOA4 2 apolipoprotein E APOE 2 apolipoprotein -

Apolipoprotein H, an Acute Phase Protein, a Performing Tool for Ultra-Sensitive Detection and Isolation of Microorganisms from Different Origins
2 Apolipoprotein H, an Acute Phase Protein, a Performing Tool for Ultra-Sensitive Detection and Isolation of Microorganisms from Different Origins Ilias Stefas1, Gregor Dubois2, Sylvia Tigrett1, Estelle Lucarz1 and Francisco Veas2 1ApoH-Technologies Faculty of Pharmacy, University Montpellier 1, Av Charles Flahault, Montpellier 2Comparative Molecular Immuno-Physiopathology Lab. UMR-MD3 Faculty of Pharmacy, University Montpellier 1, Av Charles Flahault, Montpellier France 1. Introduction Apolipoprotein H (ApoH), also known as beta2-glycoprotein I (ß2-GPI), is a plasma glycoprotein of 50 kDa. ApoH is present in human plasma at a concentration of between 150 and 300 mg/ml (Bouma et al., 1999). In blood, ApoH circulate in free conformations or bound to lipoproteins: chylomicrons, very low-density lipoprotein (VLDL), low density lipoprotein (LDL) and high-density lipoprotein (HDL). In addition, ApoH has a high affinity for triglyceride-rich lipoproteins. The amount of ApoH associated with plasma lipoproteins in healthy individuals varies according to the authors from 4 to 13% (Gambino et al., 1999a) up to about 40% (Polz & Kostner, 1979). ApoH is able to activate lipoprotein lipases (Lee et al., 1983). ApoH was isolated from the fraction of plasma lipoproteins, and described for the first time in 1961 by H. Schultze E (Schultze, 1961). In a lesser extent, ApoH is also associated to ß2-globulin fraction. ApoH is expressed in human liver, in intestinal cells and tissues (Averna et al., 1997). In rats, other sites of synthesis in low concentrations were identified as the kidney, small intestine, brain, cardiomyocytes of the heart, and at even lower in the spleen, stomach and prostate (Ragusa et al., 2006). -

Pathophysiological Mechanisms in Antiphospholipid Syndrome
Review Pathophysiological mechanisms in antiphospholipid syndrome Antiphospholipid syndrome is a systemic autoimmune disease associated with thrombosis and recurrent fetal loss in the setting of detectable antiphospholipid (aPL) antibodies. The major antigenic target has been identified as b2-glycoprotein I (b2GPI), which mediates binding of aPL antibodies to target cells including endothelial cells, monocytes, platelets and trophoblasts, leading to prothrombotic and proinflammatory changes that ultimately result in thrombosis and fetal loss. This article summarizes recent insights into the role of b2GPI in normal hemostasis, interactions between aPL antibodies, b2GPI and cell- surface molecules, molecular prothrombotic and proinflammatory changes induced by aPL antibodies and pathogenic changes leading to fetal loss in antiphospholipid syndrome. New directions in therapy using these insights are examined. 1 n n Brock E Harper , KEYWORDS: annexin anti-b2-glycoprotein I antibody antiphospholipid antibodies n antiphospholipid syndrome n endothelial cell activation n pathogenesis n platelet Rohan Willis1 activation n pregnancy loss n thrombosis n treatment & Silvia S Pierangeli†1 1Department of Internal Medicine, Division of Rheumatology, University Antiphospholipid syndrome (APS) is a systemic and use of hormone-replacement therapy or oral of Texas Medical Branch, Galveston, autoimmune disease characterized by recurrent contraceptives [9]. By contrast, venous thrombo- TX, USA †Author for correspondence: thrombosis and fetal loss in the presence of per- sis was associated with presence of hypertriglyc- [email protected] sistently positive antiphospholipid (aPL) antibod- eridemia, presence of a hereditary thrombophilia ies (Abs) including lupus anticoagulant (LAC), or aCL IgG more than 40 IU [9]. IgG/IgM anticardiolipin (aCL) Abs and anti-b2- Antiphospholipid syndrome causes significant glycoprotein I (b2GPI) Abs [1–3]. -

Protection by Recombinant Alpha 1-Antitrypsin Ala357 Arg358 Against Arterial Hypotension Induced by Factor XII Fragment
Protection by recombinant alpha 1-antitrypsin Ala357 Arg358 against arterial hypotension induced by factor XII fragment. M Schapira, … , C Roitsch, M Courtney J Clin Invest. 1987;80(2):582-585. https://doi.org/10.1172/JCI113108. Research Article The specificity of serpin superfamily protease inhibitors such as alpha 1-antitrypsin or C1 inhibitor is determined by the amino acid residues of the inhibitor reactive center. To obtain an inhibitor that would be specific for the plasma kallikrein- kinin system enzymes, we have constructed an antitrypsin mutant having Arg at the reactive center P1 residue (position 358) and Ala at residue P2 (position 357). These modifications were made because C1 inhibitor, the major natural inhibitor of kallikrein and Factor XIIa, contains Arg at P1 and Ala at P2. In vitro, the novel inhibitor, alpha 1-antitrypsin Ala357 Arg358, was more efficient than C1 inhibitor for inhibiting kallikrein. Furthermore, Wistar rats pretreated with alpha 1-antitrypsin Ala357 Arg358 were partially protected from the circulatory collapse caused by the administration of beta- Factor XIIa. Find the latest version: https://jci.me/113108/pdf Rapid Publication Protection by Recombinant a1-Antitrypsin Ala357 Arg358 against Arterial Hypotension Induced by Factor XII Fragment Marc Schapira, Marie-Andree Ramus, Bernard Waeber, Hans R. Brunner, Sophie Jallat, Dorothee Carvallo, Carolyn Roitsch, and Michael Courtney Departments ofPathology and Medicine, Vanderbilt University, Nashville, Tennessee 37232; Division de Rhumatologie, Hbpital Cantonal Universitaire, 1211 Geneve 4, Switzerland; Division d'Hypertension, Centre Hospitalier Universitaire Vaudois, 1011 Lausanne, Switzerland; and Transgene SA, 67000 Strasbourg, France Abstract is not known whether this mechanism induces the symptoms observed in these disease states or whether activation of this The specificity of serpin superfamily protease inhibitors such as pathway merely represents an accompanying phenomenon. -

Review Article Mouse Homologues of Human Hereditary Disease
I Med Genet 1994;31:1-19 I Review article J Med Genet: first published as 10.1136/jmg.31.1.1 on 1 January 1994. Downloaded from Mouse homologues of human hereditary disease A G Searle, J H Edwards, J G Hall Abstract involve homologous loci. In this respect our Details are given of 214 loci known to be genetic knowledge of the laboratory mouse associated with human hereditary dis- outstrips that for all other non-human mam- ease, which have been mapped on both mals. The 829 loci recently assigned to both human and mouse chromosomes. Forty human and mouse chromosomes3 has now two of these have pathological variants in risen to 900, well above comparable figures for both species; in general the mouse vari- other laboratory or farm animals. In a previous ants are similar in their effects to the publication,4 102 loci were listed which were corresponding human ones, but excep- associated with specific human disease, had tions include the Dmd/DMD and Hprt/ mouse homologues, and had been located in HPRT mutations which cause little, if both species. The number has now more than any, harm in mice. Possible reasons for doubled (table 1A). Of particular interest are phenotypic differences are discussed. In those which have pathological variants in both most pathological variants the gene pro- the mouse and humans: these are listed in table duct seems to be absent or greatly 2. Many other pathological mutations have reduced in both species. The extensive been detected and located in the mouse; about data on conserved segments between half these appear to lie in conserved chromo- human and mouse chromosomes are somal segments. -

Confirmation of Pathogenic Mechanisms by SARS-Cov-2–Host
Messina et al. Cell Death and Disease (2021) 12:788 https://doi.org/10.1038/s41419-021-03881-8 Cell Death & Disease ARTICLE Open Access Looking for pathways related to COVID-19: confirmation of pathogenic mechanisms by SARS-CoV-2–host interactome Francesco Messina 1, Emanuela Giombini1, Chiara Montaldo1, Ashish Arunkumar Sharma2, Antonio Zoccoli3, Rafick-Pierre Sekaly2, Franco Locatelli4, Alimuddin Zumla5, Markus Maeurer6,7, Maria R. Capobianchi1, Francesco Nicola Lauria1 and Giuseppe Ippolito 1 Abstract In the last months, many studies have clearly described several mechanisms of SARS-CoV-2 infection at cell and tissue level, but the mechanisms of interaction between host and SARS-CoV-2, determining the grade of COVID-19 severity, are still unknown. We provide a network analysis on protein–protein interactions (PPI) between viral and host proteins to better identify host biological responses, induced by both whole proteome of SARS-CoV-2 and specific viral proteins. A host-virus interactome was inferred, applying an explorative algorithm (Random Walk with Restart, RWR) triggered by 28 proteins of SARS-CoV-2. The analysis of PPI allowed to estimate the distribution of SARS-CoV-2 proteins in the host cell. Interactome built around one single viral protein allowed to define a different response, underlining as ORF8 and ORF3a modulated cardiovascular diseases and pro-inflammatory pathways, respectively. Finally, the network-based approach highlighted a possible direct action of ORF3a and NS7b to enhancing Bradykinin Storm. This network-based representation of SARS-CoV-2 infection could be a framework for pathogenic evaluation of specific 1234567890():,; 1234567890():,; 1234567890():,; 1234567890():,; clinical outcomes. -

Recombinant Human Kininogen-1 Protein
Leader in Biomolecular Solutions for Life Science Recombinant Human Kininogen-1 Protein Catalog No.: RP01026 Recombinant Sequence Information Background Species Gene ID Swiss Prot Kininogen-1 (KNG1) is also known as high molecular weight kininogen, Alpha-2- Human 3827 P01042-2 thiol proteinase inhibitor, Fitzgerald factor, Williams-Fitzgerald-Flaujeac factor, which can be cleaved into the following 6 chains:Kininogen-1 heavy chain, T- Tags kinin, Bradykinin, Lysyl-bradykinin, Kininogen-1 light chain, Low molecular weight C-6×His growth-promoting factor. Kininogen-1 is a secreted protein which contains three cystatin domains. HMW-kininogen plays an important role in blood coagulation by Synonyms helping to position optimally prekallikrein and factor XI next to factor XII. As with BDK; BK; KNG many other coagulation proteins, the protein was initially named after the patients in whom deficiency was first observed.Patients with HWMK deficiency do not have a hemorrhagic tendency, but they exhibit abnormal surface-mediated activation of fibrinolysis. Product Information Basic Information Source Purification HEK293 cells > 97% by SDS- Description PAGE. Recombinant Human Kininogen-1 Protein is produced by HEK293 cells expression system. The target protein is expressed with sequence (Gln 19 - Ser 427 ) of human Endotoxin Kininogen-1 (Accession #NP_000884) fused with a 6×His tag at the C-terminus. < 0.1 EU/μg of the protein by LAL method. Bio-Activity Formulation Storage Lyophilized from a 0.22 μm filtered Store the lyophilized protein at -20°C to -80 °C for long term. solution of PBS, pH 7.4.Contact us for After reconstitution, the protein solution is stable at -20 °C for 3 months, at 2-8 °C customized product form or for up to 1 week.