Utilization of Ancillary Studies in the Cytologic Diagnosis of Respiratory
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Medical Directors Arup Medical Directors and Consulting Faculty | 2015
MEDICAL DIRECTORS ARUP MEDICAL DIRECTORS AND CONSULTING FACULTY | 2015 MAY 2015 www.aruplab.com Information in this brochure is current as of May 2015. All content is subject to change. Please contact ARUP Client Services at (800) 522-2787 with any questions or concerns. ARUP LABORATORIES ARUP Laboratories is a national clinical and anatomic pathology reference laboratory and a nonprofit enterprise of the University of Utah and its Department of Pathology. Located in Salt Lake City, Utah, ARUP offers in excess of 3,000 tests and test combinations, ranging from routine screening tests to esoteric molecular and genetic assays. Rather than competing with its clients for physician office business, ARUP chooses instead to support clients’ existing test menus by offering complex and unique tests, with accompanying consultative support, to enhance their abilities to provide local and regional laboratory services. ARUP’s clients include many of the nation’s university teaching hospitals and children’s hospitals, as well as multihospital groups, major commercial laboratories, group purchasing organizations, military and other government facilities, and major clinics. In addition, ARUP is a worldwide leader in innovative laboratory research and development, led by the efforts of the ARUP Institute for Clinical and Experimental Pathology®. Since its formation in 1984 by the Department of Pathology at the University of Utah, ARUP has founded its reputation on reliable and consistent laboratory testing and service. This simple strategy contributes significantly to client satisfaction. When ARUP conducts surveys, clients regularly rate ARUP highly and respond that they would recommend ARUP to others. As the most responsive source of quality information and knowledge, ARUP strives to be the reference laboratory of choice for community healthcare systems. -

Clinical Microbiology Core Rotation
C:\Documents and Settings\jdnoll\Desktop\UofFCytolRot10.doc CYTOPATHOLOGY ROTATION Site: University of Florida-Gainesville/ Shands North & South Tower Faculty: Peter Drew, M.D. (4-4969) Larry J. Fowler, M.D., Cytology Director (4-4959) Jacquelyn Knapik, M.D. (4-3887) Li Lu, M.D, PhD (63-6440) Demaretta Rush, M.D. (5-3364) Edward Wilkinson, M.D. (4-4962) Anthony Yachnis, M.D., Anatomic Pathology Director (4-4951) Current Cytopathology Fellow Charlene M. Lewis, CT (ASCP) Superviser Deborah A. Carroll, CT, (ASCP) Patricia Christensen, CT (ASCP) David A. Lemire, CT (ASCP) Rotation Periods: 12 weeks for CORE Rotation broken into three 4 week rotations (a portion of the 12 weeks may be on the VA Hospital Cytology Rotation). Offered all 12 months of any training year. I. General Organization: The cytopathology core rotation consists of three 4 week rotations (total 12 weeks) routinely placed within the 1st thru 4th PGY training years of a 4 year APCP training program. The CORE rotation may also be done in one combined 12 week rotation upon special request. Cervical biopsies and local gynecologic excisions are signed out in tandem with cytology specimens (correlation of surgical and cytologic specimens). The first 4 week's rotation, residents review the day's cases at the time of sign-out with the faculty member on service. During the second and third 4 week rotations residents preview cases before sign-out, render preliminary interpretations, and receive feedback at sign out (graduated responsibility). Fellows preview the slides before sign-out and render interpretations, and have the option to attend sign-out or receive feedback from the attending pathologist later (graduated responsibility). -

Cytopathology Fellowship Faculty of Medicine, Postgraduate Medical Education
Cytopathology Fellowship Faculty of Medicine, Postgraduate Medical Education Institution: McGill University and McGill University Health Centre Location: Department of Pathology, MUHC and Duff Medical Building Type of Fellowship: One year clinical fellowship in Cytopathology Fellowship Program Director: Dr. Manon Auger Program Information Number of fellowship positions requested: One Academic affiliation: McGill University Name of hospitals involved in training: McGill University Health Centre (MUHC) Background: The fellowship will be principally based at the MUHC. This one-year post-residency clinical fellowship offers a comprehensive, integrated exposure to the field of Cytopathology. The cytological specimens handled at the MUHC include approximately 50,000 gynecological specimens per year (including approximately 7000 colposcopic specimens) as well as 10,000 non-gynecological specimens (including approximately 4000 fine needle aspirates). Exposure to liquid- based cytology is provided. Research activity and publications: The fellow will be expected to participate in at least one major research project involving, at minimum, a review of a series of cases (i.e., not simply a case report) with a view to publication in a peer-reviewed journal (i.e. not only presentation at a meeting). In addition, other research projects may be carried out, including case reports. Mission and objectives: The general mission of the fellowship is to provide training in the interpretation of cytopathology with a view to learn the entire spectrum of reactive -

The Papanicolaou and Frost 2019 Cytopathology Tutorial
Y 5 E Coun cil for Continuing Medical Education to provide continuing N 1 Statement of Need , D G . T N medical education for physicians. A Diagnostic cytopathology per forms a vital role in the O T S W N D S I di agnosis and treatment of non-neoplastic and neoplastic T Weill Cornell Medicine designates this live activity for a O T A O I R T 15. 0 1 P AMA PRA Category Credi t(s )™. P le sions. This course is intended to advance and develop S M maximum of H . R T R S I the knowledge base of pathologists in cytopathology. P Physicians should claim only the credit commensurate with E M U P Current criteria and concepts based on cytomorphologic the extent of their participation in the activity. S evaluation and approaches to differential diagnosis are the core need for the practice of cytopathology. This course is Maintenance of Certification designed to provide a practical update to cytopathologists, The American Board of Pathology has approved the Tutorial cytotechnologists, general pathologists and fellows/residents as a Self- Assessment Module (SAM) for Part II of the ABP in training. Main tenance of Certifica tion (MOC) program and designates this edu cational activity for a max imum of 10.0 SAM Course Goals and Objectives Credit(s). Physi cians should claim only the credit commen - This CME approved course will lead to improved practice surate with the extent of their participation in the activity. of cytopathology leading to enhanced pa tient care. At the conclusion of this course the at tendees will be able to: Disclosure of Relationships/ Content Validity • Evaluate cytologic criteria of various non-neoplastic It is the policy of Weill Cornell Medicine to adhere to and neoplastic lesions. -

Anesthesiology
Anesthesiology RESIDENCY PROGRAM AT Ocala Regional Medical Center Welcome to the AboutAnesthesiology HCA Healthcare Residency Program at Ocala Regional Medical Center The Anesthesiology Residency Program at Ocala Regional Medical Center is part of the HCA Healthcare Graduate Medical Education network. HCA Healthcare is the nation’s leading provider of quality, patient-centered care. We are also the leader in graduate medical education, all brought together by a single mission: Above all else, we are committed to the care and improvement of human life. ACGME ID: 401100212 Tracks & Positions Tracks NRMP # Available Positions Advanced 1587040A0 9 Salary PGY2 PGY3 PGY4 $55,456 $58,590 $60,630 Welcome and thank you for your interest in our program. In partnership with HCA Healthcare GME, we adhere to the mission statement, “Above all else, we are committed to the care and improvement of human life”. The Anesthesiology Residency Program is committed to training physicians in the science and practice of anesthesiology and perioperative medicine. In this context, we will train our colleagues in delivering evidence-based, high quality medical care emphasizing patient safety goals, and in which patient and family satisfaction is optimized. Excellence, collegiality, compassion, and integrity in patient care are the core tenets of our program education. We envision the residency program as a safe, positive and inspiring clinical environment to improve health outcomes and better serve our community. Sincerely, Ettore Crimi, MD Program Director Our faculty Ettore Crimi MD, Program Director • Anesthesiology Residency completed at MGH/Harvard • Cardiothoracic Fellowship completed at Stanford • Critical Care Fellowship completed at University of Florida • Subspecialty interests include critical care medicine, cardiothoracic anesthesia, and translational research. -

2021 Anatomic & Clinical Pathology
BEAUMONT LABORATORY 2021 ANATOMIC & CLINICAL PATHOLOGY Physician Biographies Expertise BEAUMONT LABORATORY • 800-551-0488 BEAUMONT LABORATORY ANATOMIC & CLINICAL PATHOLOGY • PHYSICIAN BIOGRAPHIES Peter Millward, M.D. Mitual Amin, M.D. Chief of Clinical Pathology, Beaumont Health Interim Chair, Pathology and Laboratory Medicine, Interim Chief of Pathology Service Line, Beaumont Health Royal Oak Interim Physician Executive, Beaumont Medical Group Interim Chair, Department of Pathology and Laboratory Medicine, Oakland University William Beaumont School Interim System Medical Director, Beaumont Laboratory of Medicine Outreach Services Board certification Associate Medical Director, Blood Bank and • Anatomic and Clinical Pathology, Transfusion Medicine, Beaumont Health American Board of Pathology Board certification Additional fellowship training • Anatomic and Clinical Pathology, • Surgical Pathology American Board of Pathology Special interests Subspecialty board certification • Breast Pathology, Genitourinary Pathology, • Blood Banking and Transfusion Medicine, Gastrointestinal Pathology American Board of Pathology Lubna Alattia, M.D. Kurt D. Bernacki, M.D. Cytopathologist and Surgical Pathologist, Trenton System Medical Director, Surgical Pathology Board certification Beaumont Health • Anatomic and Clinical Pathology, Chief, Pathology Laboratory, West Bloomfield American Board of Pathology Breast Care Center Subspecialty board certification Diagnostic Lead, Pulmonary Tumor Pathology • Cytopathology, American Board of Pathology Diagnostic -

ASC and PSC Position Statement on Use of Molecular
American Society of Cytopathology (ASC) and Papanicolaou Society of Cytopathology (PSC) Joint Position Statement on The Use of Molecular Testing on Cytologic Specimens Cytomorphologic evaluation of exfoliative and aspiration cytology specimens play an essential role in guiding the management of patients undergoing evaluation for neoplasia. In recent years, medicine has witnessed an explosive growth in our recognition and understanding of molecular genetic abnormalities that drive the development and progression of various cancers, as well as the therapeutic relevance of these abnormalities which mandates that molecular testing be performed for management decisions. Technologic advances that enable minimally invasive interventional modalities to obtain tissue for diagnosis have resulted in the increasing importance of cytologic specimens for patient management. Therefore, judicious and effective integration of molecular ancillary testing with cytopathology specimen acquisition, processing, and analysis is required in order to ensure timely and appropriate patient management. Molecular studies can serve as diagnostic adjuncts to aid in cytomorphologic classification and/or to interrogate specific relevant biomarkers, thereby providing information pertinent to prognosis and targeted therapy. Salient examples illustrating the intimate interface between cytopathology and molecular diagnostics include: (1) human papillomavirus testing on cervical cytology specimens and metastatic and primary head and neck cancers; (2) mutation panel and gene expression classifier testing on indeterminate thyroid fine needle aspirates (FNAs); (3) EGFR/ALK/ROS1 analysis on advanced‐stage lung adenocarcinoma; (4) BRAF mutational analysis in melanoma and thyroid cancer FNAs; (5) fluorescence in‐situ hybridization (FISH) testing applied to a variety of specimens such as urinary tract cytology, pancreatobiliary brushings, effusions, and cytologic samples from sarcomas and lymphomas; and (6) the application of next generation sequencing (NGS) to cytologic specimens. -
Cytopathology (Path Cyto)
path cyto 1 Pathology: Cytopathology Page updated: August 2020 This section contains information to assist providers in billing for pathology procedures related to cytopathology services. Pap Smear Tests Taking a Papanicolaou (Pap) smear sample is considered part of a pelvic examination and is not separately reimbursable. The Pap smear test is reimbursable only to the provider who performs and reads the Pap smear and issues the written report. These tests include up to three smears for Pap tests for cancer screening and/or a qualitative report on the patient’s level of estrogen. Modifiers TC and 26 Providers may use modifier TC to bill cervical or vaginal Pap smear results. When a smear is billed with modifier 26, it is reimbursable only to a hospital pathologist whose service is not covered by the hospital. Submitting a claim on one line without a modifier indicates that both the professional and technical components of the service were provided. Clinical or Hospital Laboratory Pap smears examined in a clinical or hospital laboratory can be reimbursed without a modifier only if both the professional and technical components are performed in the laboratory. Billing Restrictions CPT® code 88120 will not be reimbursed if billed in conjunction with codes 88121 or 88365; CPT code 88121 will not be reimbursed if billed in conjunction with codes 88120 or 88365. CPT codes 88142, 88143, 88147, 88148, 88150, 88152, 88153, 88164, 88165, 88166 or 88167, 88174 or 88175 may be used to bill cervical or vaginal Pap smear tests and to report physician interpretation services. Part 2 – Cytopathology path cyto 2 Page updated: August 2020 Recommended frequencies are as follows: ‹‹Recommended Frequencies CPT Codes›› CPT Codes Recommended Frequency 88142, 88143, 88147, 88148, 88150, One in 30 days 88152, 88153, 88174, 88175 88164 thru 88167 One in one year Frequency limits apply to claims billed by any provider, for the same recipient. -

Cytopathology Pathology
New York State Department of Health Clinical Laboratory Standards of Practice Specialty Requirements by Category Cytopathology Pathology Cytopathology Standard Guidance Cytopathology Standard of Practice 1 (CY S1): Staining of While the actual staining technique may vary depending on the Gynecologic Slides type of stain used and the modification of the method, any modification must include the four main steps of the standard The laboratory must use a Papanicolaou or modified Papanicolaou method: fixation, nuclear staining, cytoplasmic Papanicolaou staining method for gynecologic cytology slides. staining, and clearing. Cytopathology Standard of Practice 2 (CY S2): Prevention 10 NYCRR Subparagraph 58-1.13(b)(3)(iii) requires separate of Cross Contamination Between Specimens During the staining of gynecologic and non-gynecologic slides. Staining Process In general, all stains and solutions should be filtered or The laboratory must ensure that: changed at intervals appropriate to the laboratory’s workload to a) gynecologic and non-gynecologic cytology slides are ensure staining quality meets the laboratory’s pre-established stained separately; and criteria. Stain quality should be verified every eight (8) hours for laboratories that operate twenty-four (24) hours a day. b) non-gynecologic cytology slides that have high potential for cross-contamination are stained separately from b) A toluidine blue stain may be used to determine the other non-gynecologic slides, and the stains and cellularity of non-gynecologic specimens. solutions are filtered or changed following staining. Cytopathology Standard of Practice 3 (CY S3): Targeted Slides reviewed as part of ten (10) percent re-examination must Re-examination be included in the workload limit of the cytology supervisor or the cytotechnologist performing the re-examination. -

Cytopathology Supplemental Guide
Cytopathology Supplemental Guide Supplemental Guide: Cytopathology November 2020 1 Cytopathology Supplemental Guide TABLE OF CONTENTS INTRODUCTION ............................................................................................................................. 3 PATIENT CARE .............................................................................................................................. 4 REPORTING .................................................................................................................................... 4 CONSULTATION .............................................................................................................................. 6 PERFORMANCE OF FINE NEEDLE ASPIRATIONS ................................................................................ 8 ADEQUACY (RAPID ON-SITE EVALUATION [ROSE]) AND TRIAGE ..................................................... 10 FINE NEEDLE ASPIRATION SLIDE AND CORE BIOPSY TOUCH PREPARATIONS ................................... 12 CYTOPREPATORY TECHNIQUES ..................................................................................................... 13 MEDICAL KNOWLEDGE .............................................................................................................. 14 DIAGNOSIS ................................................................................................................................... 14 CLINICAL REASONING .................................................................................................................. -
Cytopathology: Mycobacterium Avium Complex Infection with Non-Necrotizing Granulomatous Inflammation Involving a Lymph Node
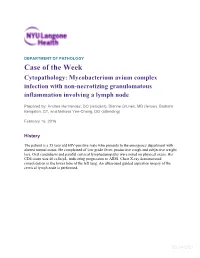
DEPARTMENT OF PATHOLOGY Case of the Week Cytopathology: Mycobacterium avium complex infection with non-necrotizing granulomatous inflammation involving a lymph node Prepared by: Andrea Hernandez, DO (resident), Dianne Grunes, MD (fellow), Barbara Bengston, CT, and Melissa Yee-Chang, DO (attending) February 16, 2016 History The patient is a 35 year old HIV-positive male who presents to the emergency department with altered mental status. He complained of low grade fever, productive cough and subjective weight loss. Oral candidiasis and painful cervical lymphadenopathy were noted on physical exam. His CD4 count was 40 cells/µL, indicating progression to AIDS. Chest X-ray demonstrated consolidation in the lower lobe of the left lung. An ultrasound guided aspiration biopsy of the cervical lymph node is performed. DC 2/4/2021 Figure. 1: (Diff-Quik stain, 400x magnification) Figure. 2: (Diff-Quik stain, 1000x magnification) DC 2/4/2021 Figure 3: (PAP stain, 40x magnification) Figure 1 - 3 Figure 1: Fine needle aspirate from the lymph node showing a histiocyte containing numerous outlines of intracellular bacilli within the cytoplasm. Figure 2: A histiocyte with abundant intracellular unstained bacilli which appear as slightly curved, colorless rods, displaying the “negative image” of the mycobacteria. Due to the striated appearance of the cellular cytoplasm, these histiocytes may be referred to as “pseudo-Gaucher cells”. Extracellular, negative-image mycobacteria are also seen within the background. Figure 3:Loose aggregate of epitheliod histiocytes forming a vague non-necrotizing granuloma, however, the mycobacteria are not readily identified as on the Diff Quik- stained smear. Diagnosis Mycobacterium avium complex infection with non-necrotizing granulomatous inflammation involving a lymph node Discussion Mycobacterium avium complex (MAC) infections are caused by one of two mycobacterial species: M. -

Cytopathology Fellowship
Cytopathology Fellowship Director: Christina Kong, MD Education content The fellow will be based at Stanford for 8 months and at the VA Palo Alto for 4 months with 2 months of elective time that can be spent at either location. Stanford Rotation During the rotation at Stanford, the fellow is responsible for running the cytopathology service. This includes daily previewing of non-gynecologic, FNA and gynecologic cases, performing fine needle aspiration biopsies with the cytology attending on-service, and participating in adequacy assessments for image-guided FNAs. The fellow is also responsible for coordinating with the AP residents on-service. Towards the end of the year, the fellow will “junior attend” on the cytology service, signing out cases with the residents which will then be finalized by the cytology attending on-service. PAVAHCS Rotation The rotation at PAVAHCS is an opportunity for cytopathology fellows to extend their technical and interpretive cytopathology skills with graduated responsibility and independence. In addition, cytopathology fellows enhance their morphologic skills and cytologic-histologic correlations by assuming graduated responsibility of “junior attending” surgical pathology sign-out. The patient population at PAVAHCS consists predominantly of aging male veterans, although increasing numbers of younger and female patients are being seen and are expected to accumulate in future years. Currently, the prevalence of malignancy is relatively high and advanced states of malignant disease are not uncommon. This setting provides excellent material for the cytologic diagnosis of a wide spectrum of malignant (and benign) disease processes. Level of supervision Cytopathology fellows have attending back-up at all times, for all procedures, cytologic interpretations and presentations.