Guidelines for the Assessment of the Impacted Maxillary Canine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Veterinary Dentistry Extraction
Veterinary Dentistry Extraction Introduction The extraction of teeth in the dog and cat require specific skills. In this chapter the basic removal technique for a single rooted incisor tooth is developed for multi-rooted and canine teeth. Deciduous teeth a nd feline teeth, particularly those affected by odontoclastic resorptive lesions, also require special attention. Good technique requires careful planning. Consider if extraction is necessary, and if so, how is it best accomplished. Review the root morphology and surrounding structures using pre-operative radiographs. Make sure you have all the equipment you need, and plan pre and post-operative management. By the end of this chapter you should be able to: ü Know the indications for extracting a tooth ü Unders tand the differing root morphology of dog and cat teeth ü Be able to select an extraction technique and equipment for any individual tooth ü Know of potential complications and how to deal with them ü Be able to apply appropriate analgesic and other treatment. Indications for Extraction Mobile Teeth Mobile teeth are caused by advanced periodontal disease and bone loss. Crowding of Teeth Retained deciduous canine. Teeth should be considered for extraction when they are interfering with occlusion or crowding others (e.g. supernumerary teeth). Retained Deciduous Teeth Never have two teeth of the same type in the same place at the same time. This is the rule of dental succession. Teeth in the Line of a Fracture Consider extracting any teeth in the line of a fracture of the mandible or maxilla. Teeth Destroyed by Disease Teeth ruined by advanced caries, feline neck lesions etc. -

A Minimally Invasive Approach Using a 4-Mm Implant Without Extraction of Impacted Maxillary Canine: Four-Year Postloading Results
819 A Minimally Invasive Approach Using a 4-mm Implant Without Extraction of Impacted Maxillary Canine: Four-Year Postloading Results Pietro Felice, MD, DDS, PhD1 The maxillary canines are the most Carlo Barausse, DDS2 commonly impacted permanent Martina Stefanini, DDS, PhD3 teeth after the third molars.1 Be- Roberto Pistilli, MD4 tween 25% and 50% of the general 5 Giovanni Zucchelli, DDS, PhD population are affected by impact- ed teeth,2 with the prevalence of The aim of this case report was to suggest an alternative minimally invasive maxillary canine impaction ranging surgical approach to an impacted maxillary canine using a 4-mm-long implant from 1% to 3%.3–5 Impactions are for a fixed prosthetic rehabilitation, avoiding tooth extraction or surgically twice as common in females (1.17%) forced extrusion and exploiting the 6 mm of coronal bone availability. At 4 as in males (0.51%); of all patients years postloading, the implant was healthy and well integrated with stable marginal bone levels. The 4-mm length of the implant reduced operative with maxillary impacted canines, it times, postsurgical morbidity, possible complications, and costs. Short implants is estimated that 8% have bilateral might be an alternative to traditional, more invasive surgical procedures impactions.4 The most common used in the rehabilitative treatment of impacted maxillary canines. Int J causes for canine impactions are Periodontics Restorative Dent 2017;37:819–824. doi: 10.11607/prd.3334 the result of any one or a combina- tion of the following factors: -

Dental Anatomy
Lecture Permanent canines General characteristic features of the canines 1.The canines are placed at the corners of the mouth, which help in keeping facial expression at the cosmetic value. 2.The canines are the longest teeth in the mouth. 3.They are the strongest teeth in the mouth. General characteristic features of the canines 4.They are the most stable teeth in the mouth because of the followings: • They have larger labio-lingual dimension. • They have long roots, which are more anchored in the alveolar bone. • The crown shape allow for “self cleansing” so they stay for longer time. 5.The middle labial lobe is highly developed incisally into a strong well-formed cusp. Principle identifying features of the permanent maxillary canine 1.Single pointed cusp. 2.The distal slope of the cusp is longer than the mesial slope. Maxillary right canine, lingual and incisal aspects. CL, Cervical line; C, cingulum; MMR, mesial marginal ridge; MLF, mesiolingual fossa; MCR, mesial cusp ridge; DCR, distal cusp ridge; LR, lingual ridge; DLF, distolingual fossa; DMR, distal marginal ridge. Principle identifying features of the permanent maxillary canine 3.Marked convex labial outline and bulky palatal cingulum. 4.Very long single root. Maxillary right canine, lingual and incisal aspects. CL, Cervical line; C, cingulum; MMR, mesial marginal ridge; MLF, mesiolingual fossa; MCR, mesial cusp ridge; DCR, distal cusp ridge; LR, lingual ridge; DLF, distolingual fossa; DMR, distal marginal ridge. Labial aspect 1.The mesial outline of the crown is convex from the cervical line to the crest of curvature, which is located at the junction of incisal and middle thirds. -

Lance Canines: an Illustrated Exploration I Would Like to Discuss a Recent Case of a Young Sheltie with a Couple of Dental Problems
Lance Canines: An Illustrated Exploration I would like to discuss a recent case of a young sheltie with a couple of dental problems. The first problem was a common one in shelties and is variably called lance canines, rostrally displaced maxillary canines or mesially displaced maxillary canines. Whatever name you choose, the problem is that the permanent maxillary canine teeth erupt pointing in the wrong direction. To understand a problem, you must first understand normal so I will review the normal relationship of the canine triad. The canine triad is composed of the maxillary lateral incisor and the canine teeth on one side and is depicted in Figure 1. In this picture, you can see that the crowns of the canine teeth are basically vertical. There is a large space between the maxillary lateral incisor and the maxillary canine and this space is known as a diastema. When the mouth is closed, the mandibular canine crown resides in the centre of the diastema so that it does not contact either of the other teeth in the triad. Figure 1: The normal canine triad. In affected shelties, one or both of the maxillary canines is malpositioned so that it is lying more horizontally. As such, the crown crosses the diastema and blocks the mandibular canine out as in Figure 2. Now on closure, the mandibular canine contacts the maxillary canine and is often forced to tip labially. Owners notice this because the mandibular canine then starts to catch on the upper lip. There is variability in the degree to which the maxillary canine is malpositioned. -

Treatment of a Patient with an Impacted Transmigrant Mandibular Canine and a Palatally Impacted Maxillary Canine
Case Report Treatment of a Patient with an Impacted Transmigrant Mandibular Canine and a Palatally Impacted Maxillary Canine Joe Rebellato, DDSa; Brian Schabelb Abstract: Very few people have seen transmigrant mandibular canines and little has been presented in the literature about this rare phenomenon. In this case report, identi®cation techniques and treatment options are presented along with the treatment results of a patient diagnosed with a transmigrant mandibular canine. This rare condition usually requires extraction of the involved tooth because orthodontic forces are seldom successful at erupting these teeth into their proper location. The treatment protocol for this patient involved a combination of orthodontic procedures, surgical extractions, gingivectomy and frenectomy, and implant replacement of the impacted transmigrant tooth. Through a collaborative effort of a team made up of an orthodontist, periodontist, prosthodontist, and oral surgeon, these techniques were used to achieve an excellent esthetic and functional outcome. (Angle Orthod 2003;73:328±336.) Key Words: Transmigrant mandibular canines; Multidisciplinary care; Implant replacement; Root re- sorption; Ankylosis; Autotransplantation; Malposition; Impaction INTRODUCTION migratory mandibular canines from 1952 to 1994, Joshi6 found that 89% were impacted, and 91% were unilateral. Impaction refers to a failure of a tooth to emerge into These teeth are generally asymptomatic7 and although the the dental arch, usually due either to space de®ciencies or tooth is far from its original site, it maintains its nerve 1 the presence of an entity blocking its path of eruption. supply from the side which it came.8 Transmigrant teeth Although heredity has long ago been described as playing usually require clinical and radiographic examination to di- 2 a role, many times the etiology is unknown. -

Chapter 15: Endodontics
Chapter 15 Endodontics. Chapter 15: Endodontics Endodontics is that branch of dentistry that deals outside dimension of the crown is established with the internal anatomy of the tooth and the early. Once the enamel is formed, the tissue that area where the inside of the tooth communicates made it goes dormant and no more enamel can with the rest of the body. ever be produced for that tooth. Teeth are composed of four main tissues. The Inside the tooth is the pulp. Lining the inside crown is covered by a thin veneer of enamel and wall of the developing tooth is a single layer of the root is covered by a thin layer of cementum. low columnar cells known as odontoblasts. Under the enamel and cementum is dentin and These cells produce the dentin. During pre- inside the dentin is a chamber filled with soft eruptive development and during eruption, the tissues known collectively as the dental pulp. odontoblasts produce primary dentin. Once the The chamber within the crown is called the pulp tooth has developed to its final length, the chamber and within the root it is called the root odontoblasts produce secondary dentin such that canal. the pulp chamber inside the tooth gets smaller as the wall of the tooth gets thicker. This The pulp is a highly organized collection of progression can be seen in the series of tissues that includes blood vessels, nerves, radiographs in Figure #15.1. Also review Figures lymphatic channels, undifferentiated cells and #7.4 to #7.8 on pages 27 to 29. -
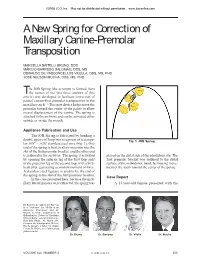
A New Spring for Correction of Maxillary Canine-Premolar Transposition
©2008 JCO, Inc. May not be distributed without permission. www.jco-online.com A New Spring for Correction of Maxillary Canine-Premolar Transposition MARCELLA BAITELLI BRUNO, DDS MÁRCIO BARROSO SALOMÃO, DDS, MS OSWALDO DE VASCONCELLOS VILELLA, DDS, MS, PHD JOSÉ NELSON MUCHA, DDS, MS, PHD he JOB Spring (the acronym is formed from Tthe names of the last three authors of this article) was developed to facilitate correction of partial canine-first premolar transposition in the maxillary arch.1-6 This new device helps move the premolar toward the center of the palate to allow mesial displacement of the canine. The spring is attached to the archwire and can be activated either outside or inside the mouth. Appliance Fabrication and Use The JOB Spring is fabricated by bending a double open-coil loop into a segment of rectangu- Fig. 1 JOB Spring. lar .019" × .026" stainless steel wire (Fig. 1). One end of the spring is bent to allow insertion into the slot of the first premolar bracket, and the other end is soldered to the archwire. The spring is activated placed on the distal side of the edentulous site. The by opening the anterior leg of the first loop and/ first premolar bracket was soldered to the distal or the posterior leg of the second loop with a bird- surface of the orthodontic band, facilitating move- beak plier, generating a constant moment of force. ment of the tooth toward the center of the palate. A stainless steel ligature is used to tie the end of the spring to the slot of the first premolar bracket. -

Maxillary Incisor Root Resorption and Interceptive Treatment
Faculty of Health Sciences Department of Clinical Dentistry Ectopic and normal maxillary canine eruption: maxillary incisor root resorption and interceptive treatment Sigurd Hadler-Olsen A dissertation for the degree of Philosophiae Doctor — Author’s name and last name A dissertation for the degree of Philosophiae Doctor – Month Year “When meditating over a disease, I never think of finding a remedy for it, but, instead, a means of preventing it”. Louis Pasteur (1822–1895) 2 1 Contents 1 Contents .............................................................................................................................. 3 2 Acknowledgements ............................................................................................................ 5 3 List of papers ...................................................................................................................... 7 4 Abbreviations and terms ..................................................................................................... 8 5 Summary ............................................................................................................................ 9 6 Introduction ...................................................................................................................... 11 6.1 Normal maxillary canine eruption ............................................................................. 11 6.2 Ectopic maxillary canine eruption ............................................................................. 12 6.2.1 Definition .......................................................................................................... -

The Use of Mandibular and Maxillary Canine Teeth in Establishing Sexual Dimorphism in the Malaysian Population of Selangor
Review Article J Forensic Sci & Criminal Inves Volume - 11 Issue 3 - March 2019 Copyright © All rights are reserved by Yuvenya Kaeswaren DOI: 10.19080/JFSCI.2019.11.555815 The Use of Mandibular and Maxillary Canine Teeth in Establishing Sexual Dimorphism in The Malaysian Population of Selangor Yuvenya Kaeswaren* and Anita Zara Weinheimer Department of Health and Life Sciences, Management & Science University, Malaysia Submission: January 18, 2019; Published: March 18, 2019 *Corresponding author: Yuvenya Kaeswaren, Faculty of Health and Life Sciences, Management & Science University, Malaysia Abstract Sex determination is one of the major roles of forensics in establishing an individual’s identity. Teeth are excellent tools in living and non- greatest sexual dimorphism. This study was conducted to investigate the effectiveness of using mandibular and maxillary canine width as well as intercanineliving victim distance identification in establishing in the field sexual of forensic dimorphism investigations. in Malaysian Amongst population all teeth, of the Selangor. mandibular The sample and maxillary comprised canine of 140 teeth Malaysian are found individuals to exhibit residing in Selangor, ages ranged between 18-30 years at a gender ratio of 1:1. The greatest mesiodistal width of the canine teeth and the intercanine distance were measured using digital vernier caliper with 0.01mm resolution. The values obtained were subjected to analysis and statistically significant sexual dimorphism was shown by the mandibular and maxillary canines. The mean values for left and right mandibular and maxillaryThe mean caninevalue for widths mandibular were less and for maxillary females intercanine than for males distances and the for differences females were were less statistically than for males significant and the (P<0.01). -

Maxillary Bilateral Canine-Premolar Transposition: a Rare Condition
Open Access Journal of Dentistry & Oral Disorders Case Report Maxillary Bilateral Canine-Premolar Transposition: A Rare Condition Agarwala P1, Agarwal V1, Rekhade R1 and Kulshrestha R2* Abstract 1Department of Orthodontics and Dentofacial Tooth transposition is very rare developmental phenomena in which Orthopaedics, Haldia Institute of Dental Sciences & the adjacent teeth are switched or have their positions changed with one Research, India another and due to this aesthetical and functional problem may be present. 2Consulting Orthodontist, Private Practice, Mumbai, The maxillary permanent canine is the tooth most frequently transposed, and India it is often transposed with the first premolar followed by the lateral incisor and *Corresponding author: Rohit Kulshrestha, lastly the central incisor in very rare cases. Several etiologic factors may lead Consulting Orthodontist, Private Practice, Mumbai, to transposition like genetics, developing tooth buds displacement, mechanical India interferences, trauma and early loss of incisors. This paper reports a case of bilateral transposition in the maxillary arch involving the first premolar and Received: March 28, 2017; Accepted: May 11, 2017; canine. Published: May 18, 2017 Keywords: Ectopic eruption; Maxillary canine; Tooth transposition Introduction interchanged positions between maxillary first premolar and canine on both right and the left sides (Figure 2). Upper left deciduous canine Tooth transposition is defined as the positional interchange in was still present and it showed decalcification on its labial aspect. spatial area of two adjacent teeth including their roots, or eruption Remaining teeth in all the other quadrants were at normal location and development of a tooth in a position normally occupied by a with normal morphology, overjet and overbite. -

The Challenging Biomechanics in a Maxillary Lateral Incisor and Canine Transposition Malocclusion
Review Article Clinician’s corner Original Article Images in Medicine Experimental Research Miscellaneous Letter to Editor DOI: 10.7860/JCDR/2019/41604.13109 Case Report Postgraduate Education The Challenging Biomechanics in a Case Series Maxillary Lateral Incisor and Canine Dentistry Section Transposition Malocclusion Short Communication ORLANDO MOTOHIRO TANAKA1, GIOVANI CERON HARTMANN2, BRUNA POVH3, FÁBIO STRAPASSON4, ANDRÉ WEISSHEIMER5 ABSTRACT Dental transposition is an alteration that occurs in dental positioning, involving two adjacent teeth. Transpositions of canines are usually accompanied by other dental anomalies such as impaction of the incisors, missing lateral incisor, peg shaped laterals, rotations or dilacerations. Twenty percent of the transpositions involve the canine and upper lateral incisors. Dental transpositions are rare and may be complete or incomplete. The aetiology of transposition is still obscure. Several populations were studied to determine the prevalence of dental transpositions. Twenty percent of the transpositions involve the canine and upper lateral incisors. A clinical case is presented here, with canine and lateral incisor transposition and the biomechanics used in orthodontic treatment for the positioning of the canine in Class I and in the line of occlusion has been described. Correction of the transposition was performed with a fixed appliance for three-dimensional biomechanical control. The root of the left lateral incisor was moved to the palatal side to allow the movement, with the inclination movement of the crown, to distal the canine. The position of the mini- implant favoured distal movement without loss of anchorage of the teeth of this hemi-arch (left). With the canine positioned in place, third-order folds were inserted in the arch to move the lateral root to the buccal side. -

Age and Sequence of Permanent Canine and Premolar Teeth Eruption in 102-174 Months Old Children in Kerman Province
Current Research in Dentistry 1 (1): 6-10, 2010 ISSN 1949-0119 © 2010 Science Publications Age and Sequence of Permanent Canine and Premolar Teeth Eruption in 102-174 Months Old Children in Kerman Province Farokhgissor Elham and Shahrzad Adhamy Department of Peadiatric Dentistry, Kerman University of Medical Science, Iran Abstract: Problem statement: The aim of this study was to investigate the eruption time of permanent canine and premolar teeth in 8.5-14.5 years (102-174 months) old boys and girls of Kerman province. Approach: The sample for this cross-sectional study consisted of 2602, 102-174 months old (8.5-14.5 years old) children form 56 primary and guidance schools in Kerman which were scattered over in 2 districts of the city. There were 1556 of girls and 1046 of boys were chosen by simple randomization and the emergence stage of each tooth was recorded. Results: The analysis indicated significantly earlier emergence ages in girls than in boys. The eruption pattern turned out to be symmetric in both sexes and no statically significant difference was detected between the right and left side. The most common observed emergence pattern in girls was mandibular canine and maxillary first premolar followed by mandibular first premolar, maxillary second premolar, then mandibular second premolar and canine and in boys it was maxillary and mandibular first premolar, mandibular canine, maxillary second premolar, mandibular second premolar and maxillary canine Conclusion: Significantly earlier emergence ages in girls seen than in boys. The sequence of eruption differs between girls and boys for mandibular canine and first premolar.