Coding/Billing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of Probable Entries Identified to Be Deleted from Electoral Roll District No & Name :- 14 Thiruvananthapuram Lac No & Name :- 134 Thiruvananthapuram
LIST OF PROBABLE ENTRIES IDENTIFIED TO BE DELETED FROM ELECTORAL ROLL DISTRICT NO & NAME :- 14 THIRUVANANTHAPURAM LAC NO & NAME :- 134 THIRUVANANTHAPURAM STATUS - S- SHIFT, E-EXPIRED , R- REPLICATION, M-MISSING, Q-DISQUALIFIED. LIST OF PROBABLE ENTRIES IDENTIFIED TO BE DELETED FROM ELECTORAL ROLL DISTRICT NO & NAME :- 14 THIRUVANANTHAPURAM LAC NO & NAME :- 134 THIRUVANANTHAPURAM PS NO & NAME :- 1 St.Joseph Lower Primary School Kochuveli(North Portion of New Building) SL.NO NAME OF ELECTOR RLN RELATION NAME SEX AGE IDCARD_NO STATUS 24 Divakaran F Sahadevan M 62 MKG1727031 E 38 Mohan M Thankamma M 55 YUC0683136 S 47 Shyni S H Sureshkumar F 29 YUC0091165 S 48 Jose F F Baby Francis M 27 YUC0080234 S 53 Aleyamma H Dharmmarajan F 34 MKG1335306 S 86 Vijayan V F Velu M 57 YUC0301341 E 132 Santhi K H Manikantan Asari F 39 FVM1276955 S 133 Jastas Gomas F Ealeeyas Gomas F 71 YUC0345967 E 208 Suresh Kumar F Nagappanasari M 48 MKG1318963 R 443 Anilkumar F Sreedharan M 45 YUC0682963 S 446 Radhamani F Anilkumar F 40 YUC0682948 S 455 Chandrasekharan F Velayudhan M 41 KL/20/135/168213 R 723 Sureshkumar F Appukkuttan M 44 YUC0676692 R 751 Santhosh S F Sasi M 24 YUC0197764 S 790 Gomathi F Kochunarayanan F 61 YUC0677765 R 791 Chandrika F Kochunarayanan F 56 YUC0677864 R 793 Chandran F Kochunarayanan M 41 KL/20/135/168551 R 809 Swamidasan F Kesavan M 48 YUC0676650 R 1145 Athul Raj B F Baby Raj D M 21 YUC0426775 R 1158 Saranya S U F Unnikrishnan S F 25 YUC0474387 R 1262 Dharmarajan F Simon M 38 MKG1128909 S STATUS - S- SHIFT, E-EXPIRED , R- REPLICATION, M-MISSING, Q-DISQUALIFIED. -

ANNEXURE 5.9 (CHAPTER V , PARA 25) FORM 10 List of Applications For
ANNEXURE 5.9 (CHAPTER V , PARA 25) FORM 10 List of Applications for objection to inclusion of names received in Form 7 Designated location identity (where Constituency (Assembly/ £ Parliamentary): Gangavalli Revision identity applications have been received) 1. List number@ 2. Period of applications (covered in this list) From date To date 18/11/2020 18/11/2020 3. Place of hearing* Serial Date of Name (in full) of Particulars of name objected at Reasons in brief Date of Time of number$ of receipt objector for objection hearing* hearing* application Part Serial Name in full number number 1 18/11/2020 SATHYA M 241 1159 SATHYA M £ In case of Union territories having no Legislative Assembly and the State of Jammu and Kashmir @ For this revision for this designated location Date of exhibition at designated Date of exhibition at Electoral * Place, time and date of hearings as fixed by electoral registration officer location under rule 15(b) Registration Officer's Office $ Running serial number is to be maintained for each revision for each under rule 16(b) designated location 23/11/2020 ANNEXURE 5.9 (CHAPTER V , PARA 25) FORM 10 List of Applications for objection to inclusion of names received in Form 7 Designated location identity (where Constituency (Assembly/ £ Parliamentary): Gangavalli Revision identity applications have been received) 1. List number@ 2. Period of applications (covered in this list) From date To date 21/11/2020 21/11/2020 3. Place of hearing* Serial Date of Name (in full) of Particulars of name objected at Reasons in brief -
2. UNIVERSITY of KERALA (Re-Accredited by NAAC with ‘A’ Grade)
1. 2. UNIVERSITY OF KERALA (Re-accredited by NAAC with ‘A’ Grade) Preliminary Minutes of the 26th Meeting of the Syndicate held on 18.03.2017 Place of Meeting : University Buildings Thiruvananthapuram Time : 10.00 AM Members present: 1. Prof.P.K.Radhakrishnan ( In the Chair) Vice– Chancellor 2. Dr.N.Veeramanikandan Pro-Vice-Chancellor 3. Sri.M.K.Abdul Rahim 4. Adv.Johnson Abraham 5. Prof.R.Mohanakrishnan 6. Sri.B.S.Jyothikumar 7. Dr.M.Jeevanlal 8. Sri.M.Sreekumar 9. Dr.Shaji.K 10. Sri.A.A.Rahim 11. Adv.K.H.Babujan 12. Adv.S.Krishnakumar 13. Sri.K.S.Gopakumar 14. Dr.P.M.Radhamany 15. Dr.Latha Devi.R 16. Sri.M.G.Ranjith Kumar 17. Sri.Bhooshan.V, Additional Secretary, GA (IT) Item No.26.01. Confirmation of the Preliminary Minutes of the 25 th meeting of the Syndicate held on 10.02-2017 – reg. (Ac.A.I) The Syndicate considered and approved the Preliminary Minutes of the 25 th Meeting of the Syndicate held on 10.02.2017 with the following modification: Item No.25.21 ‘ALSO RESOLVED that the incumbents be reverted till the posts are sanctioned by the Government’ be added after the third resolution. (Ad.A1) ========================================================================== Item No.26.02 Appointments/Career Advancement Promotion, if any - reg. (Ad.H/Ad.D.II) 2 Resolution of the Syndicate 1. Minutes of the Meeting of the Selection Committee for Selection of Assistant Professors (OBC, Open) in the Department of Communication and Journalism, University of Kerala, Kariavattom, Thiruvananthapuram held on 14.02.2017. -

FORM 11A Designated Location Identity
ANNEXURE 5.11 (CHAPTER V , PARA 25) FORM 11A Designated location identity List of applications for transposition of entry in electoral roll Received in Revision identity (where applications have been Form - 8A received) Constituency (Assembly /£Parliamentary): Edappadi 1. List number@ 2. Period of receipt of applications (covered in this list) From date To date 17/11/2020 17/11/2020 3. Place of hearing* Serial Date of Details of applicant Details of person whose entry is to be transposed Present place of Date/Time of number of receipt (As given in Part V ordinary residence hearing* application of Form 8A) Name of person Part/Serial EPIC NO. whose entry is to be no. of roll in transposed which name is included 1 17/11/2020 priyatharsini sekar priyatharsini sekar /0 , , , , NA 2 17/11/2020 dinakaran g dinakaran g /0 , , , , NA 3 17/11/2020 Thangaraji Thangaraji /0 , , , , NA £ In case of Union Territories having no Legislative Assembly and the State of Jammu & Kashmir @ For this revision for this designated location Date of exhibition at designated Date of exhibition at Electoral * Place, time and date of hearing as fixed by electoral registration officer location under rule 15(b) Registration Officer¶s Office under § Running serial number is to be maintained for each revision for each rule 16(b) designated location 23/11/2020 ANNEXURE 5.11 (CHAPTER V , PARA 25) FORM 11A Designated location identity List of applications for transposition of entry in electoral roll Received in Revision identity (where applications have been Form - 8A received) Constituency (Assembly /£Parliamentary): Edappadi 1. -

List of Probable Entries Identified to Be Deleted from Electoral Roll District No & Name :- 13 Kollam Lac No & Name :- 125 Eravipuram
LIST OF PROBABLE ENTRIES IDENTIFIED TO BE DELETED FROM ELECTORAL ROLL DISTRICT NO & NAME :- 13 KOLLAM LAC NO & NAME :- 125 ERAVIPURAM STATUS - S- SHIFT, E-EXPIRED , R- REPLICATION, M-MISSING, Q-DISQUALIFIED. LIST OF PROBABLE ENTRIES IDENTIFIED TO BE DELETED FROM ELECTORAL ROLL DISTRICT NO & NAME :- 13 KOLLAM LAC NO & NAME :- 125 ERAVIPURAM PS NO & NAME :- 1 Craven L. M. S. H. S. (Eastern Portion of Main Building) SL.NO NAME OF ELECTOR RLN RELATION NAME SEXAGEIDCARD_NO STATUS 56 Sivadasan F Kannan M 59KL/18/124/138309 E 75Oseela H Sheyck F 49DQK0939348 S 76 Sheycksayd F Muhammad Buhar M 45DQK0940403 S 90 Aju Kumar F Thankaraj M 26WLS0299651 S 123Saramma F Thomas F 84KL/18/124/138180 E 136 Mumthasbeevi F Seyyad Abdulla F 78KL/18/124/138126 S 137 Seydsadakathulla F Seyd Asdulla Sahib M 41KL/18/124/138261 S 138 Shameemunisa O Abdul Kabeer F 41WLS0048488 S 139 Rama Lakshmi H Thottappa Koundar F 67KL/18/124/138294 S 141 Gopalakrishnan F Bharggavan M 53DQK2010536 S 142 Bebi H Gopalakrishnan F 44DQK2010528 S 151Gopalan F Kumaran M 53KL/18/124/138325 S 152 Sulekha H Gopalan F 46KL/18/124/138326 S 153Anil Kumar F Gopalan M 31DQK3074606 S 167 Ashokkumar F Damodaran M 50WLS0107284 S 206 Sarasvathiammal F Subrahmanyayyar F 84DQK2169084 S 207 Radha F Subrahmanyayyar F 40DQK2169076 S 209Valsa H Manoj F 53DQK2164572 S 210 Sajuem F Muthukrishnan M 40DQK2167914 S 211Deyji H Sajuem F 38DQK2170694 S 225 Radhakrishnapilla F Vasudevanpilla M 62KL/18/124/138087 S 226 Ramadevi H Radhakrishnapilla F 53KL/18/124/138088 S 227 Ramya F Radhakrishnapilla F 30DQK2011179 S 234 Noelyn H Ravindranathan F 74WLS0459883 E 248Anjjali H Pramji F 32KCW1331719 R 251 Dali H Israyel Thomas F 52KL/20/139/171129 S 324 Ramakrishnan F Perumalnadar M 61DQK1465061 E 348Kabeer F Abdul Asees M 65DQK2131001 E 394Vinsanr F Josaf M 56KL/18/124/138478 S 395Mezhsi H Vinsanr F 46KL/18/124/138479 S 396 Muhammadkunj F Kasimkunj M 68KL/18/124/138104 E STATUS - S- SHIFT, E-EXPIRED , R- REPLICATION, M-MISSING, Q-DISQUALIFIED. -

Accused Persons Arrested in Kannur District from 12.04.2020To18.04.2020
Accused Persons arrested in Kannur district from 12.04.2020to18.04.2020 Name of Name of Name of Place at Date & Arresting the Court Name of the the father Age & Address of Cr. No & Police Sl. No. which Time of Officer, at which Accused of Sex Accused Sec of Law Station Arrested Arrest Rank & accused Accused Designation produced 1 2 3 4 5 6 7 8 9 10 11 286/2020 U/s NOTICE Sakeena 188,269,IPC 18-04- Ajith Kumar SERVED - J 35, Manzil Mukkile Anjerakandy &sec 118(e) Of Kuthuparamb 1 Sajeer M Assainar 2020 at KP, SI of F C M, Male peedika Jn KP Act&sec a (KANNUR) 19:35 Hrs Police KUTHUPARA Vellachal Bavod &sec. 4(2)(a)5 MBA KEDO 202 314/2020 U/s 269, 188 IPC & 118(e) of KP E K HOUSE, Edakkad Act & Sec. 5 NOTICE 18-04- 28, HUSSAN amsom r/w 4 of Edakkad SERVED - A 2 ASHRAF E K ASEES E K 2020 at Sheeju T K Male MUKKU, PO Hussan Kerala (KANNUR) C J M, 20:25 Hrs EDAKKAD Mukku Epidemic THALASSERY Diseases Ordinance 2020 313/2020 U/s 269, 188 IPC & 118(e) of KP Najamas, Edakkad Act & Sec. 5 NOTICE 18-04- 30, Hussan amsom r/w 4 of Edakkad SERVED - A 3 Shameel A M Mayan A P 2020 at Sheeju T K Male Mukku, Hussan Kerala (KANNUR) C J M, 20:10 Hrs Edakkad PO Mukku Epidemic THALASSERY Diseases Ordinance 2020 130/2020 U/s U/S 188 ,269 IPC and 118(e) Rubeena of KP Act and Umeshan. -

August-December 2020
MAHATMA GANDHI UNIVERSITY LIBRARY LIST OF NEW ADDITIONS August-December 2020 Acc. No. Author Title Publisher Year Call No. Arts 61039 जयदेव तनेजा (Jaidev Jaidev आधुननक भारतीय नाट्य- Radhakrishna 2015 H 792.015 Prakashan Pvt. 152 Q5 Taneja) 픿वमर्श(Jaidev Aadhunik bharatiya natya-vimarsh) Ltd. 61038 ने픿मचꅍद्र जैन रंगदर्शन(Jaidev Rangdarshan) Radhakrishna 2016 H 792.095 4 (Jaidev Nemichandra Jain) Prakashan Pvt 152 Q6 Ltd. Biography 60997 राजᴂद्रमोहन भटनागर डॉ आंबेडकर(Jaidev Dr. Jagathram & 2011 H 923.6 AMB sons 152Q1 Rajendra Mohan Ambedkar):जीवन-मम Bhatnagar) (Jaidev jeevan-marma) 60996 नानकचंद रत्तु (Jaidev Nanak डॉ आंबेडकर जीवन के अं鄿तम Kitabghar 2017 H 923.6 AMB prakashan 152Q7 Chand Rattu) कु छ वर्ष (Jaidev Dr. Ambedkar jeevan ke antim kuchh varsh) 60998 राजᴂद्रमोहन भटनागर डॉ आंबेडकर (Jaidev Dr. Jagathram & 2017 H 923.6 AMB sons 152Q71 Rajendra Mohan Ambedkar): चिंचतन और Bhatnagar) 픿वचार (Jaidev chinthan aur vichar) 60993 र्शीला झुनझुनवाला (Jaidev Shila नी तारⴂ के अनछुए Kitabghar 2013 H 927.914 Prakashan 308 152Q3 Jhunjhunwala) प्रंग (Jaidev Sine sitaron ke anchhuye prasang) 60928 अजीत कौर (Jaidev Ajeet Kaur) खानाबदोर्श Kitabghar 2013 H 928 AJE (Jaidev Kahanabadosh) Prakashan 152Q3 60929 अजीत कौर (Jaidev Ajeet Kaur) कू 蔼ा-कबा蔼ा (Jaidev Koorha- Kitabghar 2016 H 928 AJE kabaarha) Prakashan 152Q6 60967 गो픿वꅍद 픿मश्र (Jaidev Govind मेरे ाक्षा配कार (Jaidev Mere Kitabghar 2015 H 928 GOV Mishra) saakshaatkaar) Prakashan 152Q5 60972 जयदेव तनेजा (Jaidev Jaidev रंग-ाक्षा配कार (Jaidev Rang- Kitabghar 2014 H 928 JAI Taneja) saakshatkaar) Prakashan -

Annual Report 2016-17 Thunchath Ezhuthachan Malayalam University
THUNCHATH EZHUTHACHAN MALAYALAM UNIVERSITY ANNUAL REPORT 2016-17 THUNCHATH EZHUTHACHAN MALAYALAM UNIVERSITY ANNUAL REPORT CONTENTS 1. Vice Chancellor’s note 2. Aims and objectives 3. Milestones 4. ‘Akhsaram’ Campus 5. Academic activities 6. Library 7. Student’s welfare, hostels 8. Activities with social commitment 9. International co-operation., Gundert Chair 10. Projects 11. 11. Publications 12. Administration 13. Appendix Editor: Dr. P.B.Lalkar English Translation Team Prof. Madhu Eravankara ( Co-ordinator) Dr. M. Vijayalakshmy, Dr. A.P Sreeraj, Dr. Jainy Varghese, Sri K.S Hakeem Design & Lay-out : Lijeesh M.T. Printing : K.B.P.S. Kakkanad, Kochi P R E FA C E Justice (Retd.) P Sathasivam Prof. C Ravindranath K Jayakumar Chancellor Pro Chancellor Vice Chancellor It is with great pleasure that I am presenting the Annual Report of Malayalam University up to March 31, 2017. The university started functioning in 2012 and the admission formalities of the first batch of students were completed in August 2013. Initially we started with 5 M.A courses. When we look back in 2017, it is worthy to note that the university has achieved tremendous growth both in infrastructure and academic level. Within this short span of time, we could start 10 M.A. Courses and Research Programmes. The first two batches of M.A and one batch of M.Phil students are out. Amenities like Library, Studio and Theatre claims self sufficiency. 28 permanent teachers were also appointed. The year 2016-17 witnessed so many important developments. The new library- research block and Heritage Museum, were opened. The year was marked with variety of academic activities and visit of several dignitaries. -

PG IG SGC-2015-16-Website Selection.Xlsx
list of Selected Candidates for the award of Post Graduate Indira Gandhi Scholarship for Single Girl Child for the academic session 2015-16 Father's Mother's PG College/University Recommedation S.No. Candidate ID Name of applicant State Subject of the Expert Name Name Degree Name Committee Human Genetics SGC-OBC-2015-16- Andaman and 1 NUZHAT UMRAN UMRAN ALI NOOR JAHAN M.Sc. & Molecular Bharathiar University Awarded 39593 Nicobar Islands Biology SGC-GEN-2015-16- ANAPAREDDY ANAPAREDDY MONTESSORI MAHILA 2 ANAPAREDDY SYAMALA Andhra Pradesh M.Sc. MATHEMATICS Awarded 30849 RATHAIAH AKKAMMA KALASALA SGC-OBC-2015-16- SRI KRISHNADEVARAYA 3 B PRAMEELA B MADDILETI B ADILAKSHMAMMA Andhra Pradesh M.Sc. ZOOLOGY Awarded 34803 UNIVERSITY SGC-OBC-2015-16- BALAKA BALAKA BHAGYA 4 BALAKA SARANYA Andhra Pradesh M.Sc. BOTANY ANDHRA UNIVERSITY Awarded 35010 SEETHARAMAMURTY LAKSHMI SGC-OBC-2015-16- BEZAWADA BEZAWADA LAKSHMI ELECTRONICS AND 5 BEZAWADA MADHAVI Andhra Pradesh M.Sc. ANDHRA UNIVERSITY Awarded 40632 YEDUKONDALU KUMARI INSTRUMENTATION SGC-OBC-2015-16- BONU PRASANTHI 6 BONU APPALANAIDU BONU PARVATHI Andhra Pradesh M.Sc. TECH GEOPHYSICS ANDHRA UNIVERSITY Awarded 35949 KUMARI SGC-OBC-2015-16- C MURALI MOHAN 7 CHENNA MOUNA C ANANTHA LAKSHMI Andhra Pradesh M.Sc. MATHEMATICS SPMVV Awarded 31979 RAO SGC-OBC-2015-16- CHENNAM DHANA Acharya Nagarjuna 8 CHENNAM PRIYANKA CHENNAM SURIBABU Andhra Pradesh M.Com. commerce Awarded 31461 LAKSHMI University SMT.GENTELA SGC-OBC-2015-16- CHEVIRALA CHEVIRALA 9 CHEVIRALA ANUSHA Andhra Pradesh M.Sc. PHYSICS SAKUNTALAMMA Awarded 32027 VENKATESWARARAO KALAVATHI COLLEGE Chaitanya SGC-OBC-2015-16- CHIRUMALLA 10 CHIRUMALLA HARITHA SAROJANA Andhra Pradesh M.Sc. -
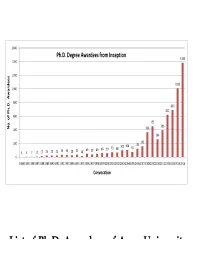
List of Ph.D. Awardees of Anna University List of Ph.D
1600 Ph.D. Degree Awardees from Inception 1385 1400 1200 1010 1000 800 690 622 600 455 396 No. of Ph.D. Awardees Awardees ofofPh.D. Ph.D. No.No. 400 366 264 200 162 101 106 124 73 68 76 36 33 35 49 39 49 60 59 3 5 7 12 17 25 25 25 28 18 0 198419851986198719881989199019911992199319941995199519961997199819992000200120022003200420052006200720082010201020122013201320142016 Convocation List of Ph.D. Awardees of Anna University List of Ph.D. Awardees of Anna University from the Inception 36th CONVOCATION HELD ON 20.01.2016 YEAR OF Sl.No Sl. NO NAME REGNO FACULTY AWARD Jan-16 1 1 Abdul Bari J 100960221002 CIVIL ENGINEERING Jan-16 2 2 Ambily P.S 1022119706 CIVIL ENGINEERING Jan-16 3 3 Arulkumaran S 10990221003 CIVIL ENGINEERING Jan-16 4 4 Arulmozhi R 10990221004 CIVIL ENGINEERING Jan-16 5 5 Arun Babu E 2713119707 CIVIL ENGINEERING Jan-16 6 6 Arun M 100930221003 CIVIL ENGINEERING Jan-16 7 7 Aruna S 2922119105 CIVIL ENGINEERING Jan-16 8 8 Aswin Sidhaarth K.R 100910211004 CIVIL ENGINEERING Jan-16 9 9 Balaji S 10960221005 CIVIL ENGINEERING Jan-16 10 10 Bhagavathi Pushpa T 20091032002 CIVIL ENGINEERING Jan-16 11 11 Divya Y 1024119111 CIVIL ENGINEERING Jan-16 12 12 Gopikrishnan T 1014119107 CIVIL ENGINEERING Jan-16 13 13 Gopikumar S 2011110104 CIVIL ENGINEERING Jan-16 14 14 Gopinathan Mj 4089023103 CIVIL ENGINEERING Jan-16 15 15 Hema S 7083022203 CIVIL ENGINEERING Jan-16 16 16 Jeevarenuka K 20091032005 CIVIL ENGINEERING Jan-16 17 17 Jerlin Regin J 2009710105 CIVIL ENGINEERING Jan-16 18 18 Kalai Selvan P 2006119701 CIVIL ENGINEERING Jan-16 19 19 Kalidasan -
2018 Session List of Candidates Allotted
DIPLOMA IN NURSING FOR WOMEN - 2017 - 2018 SESSION LIST OF CANDIDATES ALLOTTED COLLEGE : Madras Medical College SNO RANK ARNO NAME TOTAL HSC GROUP COMM. JOIN DATE MARKS 1 14 4936 MEENA E 92.50 SCIENCE MBC/DNC 2 23 3301 TAMIL ARASI M 92.00 SCIENCE BC 3 25 4138 ANITHA E 91.88 SCIENCE MBC/DNC 4 26 2458 KEERTHANA S 91.88 SCIENCE BC 5 28 4470 KANIMOZHI G 91.75 SCIENCE MBC/DNC 6 29 4629 RAMYA R 91.75 SCIENCE SC 7 52 518 SARASWATHI B 90.38 SCIENCE MBC/DNC 8 53 4387 MONIKA BALA M 90.38 SCIENCE MBC/DNC 9 69 384 NATHIYA E 89.88 SCIENCE MBC/DNC 10 76 5627 MANIMEKALAI S 89.63 SCIENCE MBC/DNC 11 78 832 SUSHMITHA C 89.63 SCIENCE MBC/DNC 12 91 596 PRIYADHARSHINI S 89.13 SCIENCE MBC/DNC 13 92 90 NEELAVENI P 89.13 SCIENCE MBC/DNC 14 99 1908 SARANYA M 88.88 SCIENCE MBC/DNC 15 101 3071 GEETHA S 88.88 SCIENCE MBC/DNC 16 105 3648 MONISHA V 88.75 SCIENCE SCA 17 114 563 MAHALAKSHMI S 88.50 SCIENCE BC 18 116 1517 JENIFA C R 88.38 SCIENCE BC 19 120 4087 VINITHA R 88.38 SCIENCE MBC/DNC 20 130 747 REVATHI C 88.13 SCIENCE BC 21 132 2662 JEBA ISWARYA G 88.00 SCIENCE BC 22 136 382 VISHNUPRIYA.J 88.00 SCIENCE MBC/DNC 23 149 1320 NIVEDHA M 87.75 SCIENCE BC 24 154 850 DHIVYA K 87.75 SCIENCE MBC/DNC 25 160 5716 GOKULAVANI A 87.63 SCIENCE MBC/DNC 26 167 3723 KALAISELVI V 87.50 SCIENCE SC 27 169 1483 ELAKKIYA G 87.50 SCIENCE MBC/DNC 28 180 2391 LATHA R 87.38 SCIENCE MBC/DNC 29 181 5262 SANGEETHA S 87.25 SCIENCE SC 30 193 1477 VINCY PRIYA.K 87.13 SCIENCE BC Page 1 of 4 DIPLOMA IN NURSING FOR WOMEN - 2017 - 2018 SESSION LIST OF CANDIDATES ALLOTTED COLLEGE : Madras Medical College SNO RANK ARNO NAME TOTAL HSC GROUP COMM. -

Current Affairs for Assistant Exam 5.Pmd
CAREERupdate CURRENT AFFAIRS 2018 SELECTED QUESTIONS AND ANSWERS - 05 Awards, Honours & Who’s who 01.Who authored the book ‘Lincoln in the Bardo’? George Saunders George Saunders won the 2017 Man Booker Prize for his historical CAREERCAREERCAREERnovel ‘Lincoln in the Bardo’. Man Booker Prize 2016 - Paul Beatty (for ‘The Sellout’) DSC Prize for South Asian Literature in 2017 - Anuk Arudpragasam of Sri Lanka for his work -’The Story of a Brief history Marriage’) 02. Who is the last winner of the Man Booker International Prize? Olga TokarczukGUIDANCEGUIDANCEGUIDANCE (in 2018, Book - Flights) Man Booker International Prize 2016 - Han Kang (Book - The Vegetarian) Pulitzer Prize for fiction for the 2018 - Less (authored by Andrew Sean Greer) 03. Who hasBUREAUBUREAUBUREAU won the Moortidevi Award for the year 2017? Joy GoswamiBUREAU (Book - Du Dondo Phowara Matro) Moortidevi Award for the year 2016 - M.P. Veerendra Kumar (Book - Hymavathabhoovil) CAREER GUIDANCE BUREAU ATTINGAL, TVPM & KOTTARAKKARA - 8590 333 999 www.careerguidancebureau.com Fresh batches for: Secretariat Assistant, Univer- sity Assistant, HSA (PS), LDC (Longe Term) Separate hostel facilities for ladies and gents for outstation candidates. 04. Who has won the Vyas Samman for the year 2017? Mamta Kalia (Sukkham Dukkham) Vyas Samman, 2016 - Surinder Verma Kalidas Samman 2017 -18 - Lekshmi Vishwanathan 05. Who has won the Harivarasanam award for the year 2017? K.S. Chithra 2016 - Gangai Amaran 06. Who authored the book ‘Shyama Madhavam’? Prabha Varma The Vallathol award for the year 2017 - Prabha Varma 2016 - Sreekumaran Thampi 07. Name the Gujarati poet to be selected for the Saraswati Samman for the year 2017. SitanshuCAREERCAREERCAREER Yashaschandra (for his work ‘Vakhar’) Saraswati Samman for the year 2016 - Mahabaleshwar Sail (for his work - Hawthan) The first recipient - Harivansh Rai Bachchan (in 1991) 08.