Dynorphin Increases Extracellular Levels of Excitatory Amino Acids in the Brain Through a Non-Opioid Mechanism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Characterisation and Partial Purification of a Novel Prohormone Processing Enzyme from Ovine Adrenal Medulla
Volume 246, number 1,2, 44-48 FEB 06940 March 1989 Characterisation and partial purification of a novel prohormone processing enzyme from ovine adrenal medulla N. Tezapsidis and D.C. Parish Biochemistry Group, School of Biological Sciences, University of Sussex, Falmer, Brighton, Sussex, England Received 3 January 1989 An enzymatic activity has been identified which is capable of generating a product chromatographically identical with adrenorphin from the model substrate BAM 12P. This enzyme was purified by gel filtration and ion-exchange chromatog- raphy and characterised as having a molecular mass between 30 and 45 kDa and an acidic pL The enzyme is active at the acid pH expected in the secretory vesicle interior and is inhibited by EDTA, suggesting that it is a metalloprotease. This activity could not be mimicked by incubation with lysosomal fractions and it meets the criteria to be considered as a possible prohormone processing enzyme. Prohormone processing; Adrenorphin; Secretory vesiclepurification 1. INTRODUCTION The purification of an endopeptidase responsi- ble for the generation of adrenorphin was under- Active peptide hormones are released from their taken, using the ovine adrenal medulla as a source. precursors by endoproteolytic cleavage at highly Adrenorphin is known to be located in the adrenal specific sites. The commonest of these is cleavage medulla of all species so far investigated [6]. at pairs of basic residues such as lysine and Secretory vesicles (also known as chromaffin arginine [1,2]. However another common class of granules) were isolated as a preliminary purifica- processing sites are known to be at single arginine tion step, since it is known that prohormone pro- residues, adjacent to a proline [3]. -

Download Product Insert (PDF)
PRODUCT INFORMATION Dynorphin A Item No. 18169 CAS Registry No.: 80448-90-4 O O Formal Name: dynorphin A HO NH2 HO NH O O NH2 Synonym: Dynorphin A (1-17) O N O H C H N O H O NH MF: 99 155 31 23 N O O H H H N NH FW: 2,147.5 N N 2 N N N H H O O NH O O H H H H N N N ≥95% H2N H2N O Purity: N N NH NH H H O O O NH O H N Stability: ≥2 years at -20°C O N H2N N N H NH2 H H O NH2 Supplied as: A crystalline solid OH UV/Vis.: λmax: 279 nm Laboratory Procedures For long term storage, we suggest that dynorphin A be stored as supplied at -20°C. It should be stable for at least two years. Dynorphin A is supplied as a crystalline solid. A stock solution may be made by dissolving the dynorphin A in the solvent of choice. Dynorphin A is soluble in organic solvents such as DMSO and dimethyl formamide, which should be purged with an inert gas. The solubility of dynorphin A in these solvents is approximately 30 mg/ml. Further dilutions of the stock solution into aqueous buffers or isotonic saline should be made prior to performing biological experiments. Ensure that the residual amount of organic solvent is insignificant, since organic solvents may have physiological effects at low concentrations. Organic solvent-free aqueous solutions of dynorphin A can be prepared by directly dissolving the crystalline solid in aqueous buffers. -

From Opiate Pharmacology to Opioid Peptide Physiology
Upsala J Med Sci 105: 1-16,2000 From Opiate Pharmacology to Opioid Peptide Physiology Lars Terenius Experimental Alcohol and Drug Addiction Section, Department of Clinical Neuroscience, Karolinsku Institutet, S-I71 76 Stockholm, Sweden ABSTRACT This is a personal account of how studies of the pharmacology of opiates led to the discovery of a family of endogenous opioid peptides, also called endorphins. The unique pharmacological activity profile of opiates has an endogenous counterpart in the enkephalins and j3-endorphin, peptides which also are powerful analgesics and euphorigenic agents. The enkephalins not only act on the classic morphine (p-) receptor but also on the 6-receptor, which often co-exists with preceptors and mediates pain relief. Other members of the opioid peptide family are the dynor- phins, acting on the K-receptor earlier defined as precipitating unpleasant central nervous system (CNS) side effects in screening for opiate activity, A related peptide, nociceptin is not an opioid and acts on the separate NOR-receptor. Both dynorphins and nociceptin have modulatory effects on several CNS functions, including memory acquisition, stress and movement. In conclusion, a natural product, morphine and a large number of synthetic organic molecules, useful as drugs, have been found to probe a previously unknown physiologic system. This is a unique develop- ment not only in the neuropeptide field, but in physiology in general. INTRODUCTION Historical background Opiates are indispensible drugs in the pharmacologic armamentarium. No other drug family can relieve intense, deep pain and reduce suffering. Morphine, the prototypic opiate is an alkaloid extracted from the capsules of opium poppy. -

S-1203 Dynorphin a Elisa Dynorphins Are a Class of Opioid Peptides
BMA BIOMEDICALS Peninsula Laboratories S-1203 Dynorphin A Elisa Dynorphins are a class of opioid peptides. As their precursor Proenkephalin-B is cleaved during processing, its residues 207-223 (Dynorphin A) and 226-238 (Rimorphin, Dynorphin B) are released, among others. Dynorphins contain a high proportion of basic and hydrophobic residues. They are widely distributed in the central nervous system, with highest concentrations in the hypothalamus, medulla, pons, midbrain, and spinal cord, where they are also produced. Dynorphins are stored in large dense-core vesicles characteristic of opioid peptides storage. Dynorphins exert their effects primarily through the κ-opioid receptor (KOR), a G-protein- coupled receptor. They are part of the complex molecular changes in the brain leading to cocaine addiction. Dynorphins are important in maintaining homeostasis through appetite control, circadian rhythms and the regulation of body temperature. However, Dynorphin derivatives are generally considered to be of little clinical use because of their very short duration of action. This ELISA was developed with serum from rabbits immunized with Dynorphin coupled to a carrier protein. TECHNICAL AND ANALYTICAL CHARACTERISTICS Lot number: A18004 Host species: Rabbit IgG Quantity: 96 tests Format: Formulated for extracted samples (EIAH type). Shelf-life: One year from production date. Store refrigerated at 4° - 8°C. Applications: This ELISA has been validated with the included reagents. It is intended to be used with appropriately extracted samples (original protocol III, Std.Ab1hr.Bt). For research use only. Please see www.bma.ch for protocols and general information. Range: 0-5ng/ml Average IC50: 0.09ng/ml Immunogen: Synthetic peptide H-Tyr-Gly-Gly-Phe-Leu-Arg-Arg-Ile-Arg-Pro-Lys-Leu- Lys-Trp-Asp-Asn-Gln-OH coupled to carrier protein. -

Dynorphin A-( L-L 7) Induces Alterations in Free Fatty Acids, Excitatory Amino Acids, and Motor Function Through an Opiate- Receptor-Mediated Mechanism
The Journal of Neuroscience, December 1990, IO(1‘2): 37934900 Dynorphin A-( l-l 7) Induces Alterations in Free Fatty Acids, Excitatory Amino Acids, and Motor Function Through An Opiate- Receptor-Mediated Mechanism Rohit Bakshi,’ Amy H. Newman,2 and Alan I. Faden’ ‘Center for Neural Injury, Department of Neurology, University of California, San Francisco, California 94121 and Neurology Service (127), Department of Veterans Affairs, San Francisco, California 94121, and *Department of Applied Biochemistry, Walter Reed Army Institute of Research, Washington, DC. 20307-5100 The endogenous opioid dynorphin A-( l-1 7) (Dyn A) has been Phamacological studies with opioid-receptor antagonists sup- implicated as a mediator of tissue damage after traumatic port the concept that endogenous opioids contribute to the spinal cord injury (TSCI) and causes hindlimb paralysis when pathophysiology of tissue damageafter CNS trauma (Faden et administered intrathecally. Motor impairment following in- al., 1981; Flamm et al., 1982; Hayes et al., 1983; Arias, 1985; trathecal Dyn A is attenuated by antagonists of excitatory Inoue, 1986; McIntosh et al., 1987). Dynorphin A (Dyn A), a amino acids (EAAs); whether opioid receptors mediate such 17-amino acid opioid peptide thought to be an endogenous injury has been questioned. TSCI causes various biochem- ligand for the K-Opiate receptor (Chavkin and Goldstein, 1981; ical changes associated with secondary tissue damage, in- Yoshimura et al., 1982), has been implicated as a secondary cluding alterations in tissue amino acids, phospholipids, and injury factor after spinal cord (Faden et al., 1985) and brain fatty acids. Such changes reflect injury severity and corre- trauma (McIntosh et al., 1987). -

213393336.Pdf
The Development of Analytical Methods for Investigations of Dynorphin A 1-17 Metabolism in the Central Nervous System and Peripheral Tissues and Transport at the Blood Brain Barrier By Courtney D. Kuhnline Sloan B.S., Investigative and Medical Sciences and Chemistry, Saint Louis University, 2005 M.S., Pharmaceutical Chemistry, The University of Kansas, 2008 Submitted to the Department of Pharmaceutical Chemistry and the faculty of the Graduate School of the University of Kansas in partial fulfillment of the requirements for the degree of Doctor of Philosophy. ________________________________ Chairperson- Dr. Susan M. Lunte ________________________________ Dr. Kenneth L. Audus ________________________________ Dr. John F. Stobaugh ________________________________ Dr. Teruna J. Siahaan ________________________________ Dr. Jane V. Aldrich Dissertation Defense: February 11, 2011 The Dissertation Committee for Courtney Kuhnline Sloan certifies that this is the approved version of the following dissertation: The Development of Analytical Methods for Investigations of Dynorphin A 1-17 Metabolism, in the Central Nervous System and Peripheral Tissues, and Transport at the Blood Brain Barrier ________________________________ Chairperson- Dr. Susan M. Lunte Date approved:_______________________ ii This dissertation is dedicated to my parents, Pam and Mike Kuhnline, for always pushing me to do my absolute best at everything I have ever attempted, and to my husband, Patrick, for his continual encouragement and willingness to spend our first months as a married couple with me buried under my thesis. This work was possible because of the unconditional love and support I have been so fortunate to have from each of you. iii Abstract Dynorphin A 1-17 (Dyn A 1-17) is an endogenous neuropeptide that acts preferentially at the kappa opioid receptor. -
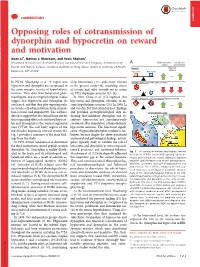
Opposing Roles of Cotransmission of Dynorphin and Hypocretin on Reward and Motivation Xuan Li1, Nathan J
COMMENTARY COMMENTARY Opposing roles of cotransmission of dynorphin and hypocretin on reward and motivation Xuan Li1, Nathan J. Marchant, and Yavin Shaham1 Behavioral Neuroscience Research Branch, Intramural Research Program, Department of A Brain stimulation Cocaine self- reward administration Health and Human Services, National Institute on Drug Abuse, National Institutes of Health, Baseline Impulsive behavior Baltimore, MD 21224 Hypocretin Dynorphin In PNAS, Muschamp et al. (1) report that sleep homeostasis (12), and—most relevant HCRTR1 antagonist: KOR signal dominates hypocretin and dynorphin are coexpressed in to the present study—the rewarding effects the same synaptic vesicles of hypothalamic of cocaine and other rewards via its action neurons. Their data from behavioral, phar- on VTA dopamine neurons (13, 14). macological, and electrophysiological studies In 2001, Chou et al. (15) reported that HCRTR1 antagonist + KOR antagonist: Balance restored suggest that hypocretin and dynorphin are hypocretin and dynorphin colocalize in the coreleased, and that they play opposing roles same hypothalamic neurons (15). In 2006, Li in cocaine self-administration, brain stimula- and van den Pol (16) extended these findings ’ tion reward, and impulsivity. The authors and provided electrophysiological data in- B Ventral tegmental area: data also suggest that the critical brain site for dicating that inhibitory dynorphin and ex- these opposing effects of coreleased hypocre- citatory hypocretin are simultaneously tin and dynorphin is the ventral tegmental coreleased after stimulation of hypothalamic area (VTA), the cell body region of the hypocretin neurons. The functional signifi- mesolimbic dopamine reward system (2). cance of hypocretin/dynorphin corelease is un- Fig. 1 provides a summary of the main find- known, because despite the above-mentioned ings from the study. -

G Protein‐Coupled Receptors
S.P.H. Alexander et al. The Concise Guide to PHARMACOLOGY 2019/20: G protein-coupled receptors. British Journal of Pharmacology (2019) 176, S21–S141 THE CONCISE GUIDE TO PHARMACOLOGY 2019/20: G protein-coupled receptors Stephen PH Alexander1 , Arthur Christopoulos2 , Anthony P Davenport3 , Eamonn Kelly4, Alistair Mathie5 , John A Peters6 , Emma L Veale5 ,JaneFArmstrong7 , Elena Faccenda7 ,SimonDHarding7 ,AdamJPawson7 , Joanna L Sharman7 , Christopher Southan7 , Jamie A Davies7 and CGTP Collaborators 1School of Life Sciences, University of Nottingham Medical School, Nottingham, NG7 2UH, UK 2Monash Institute of Pharmaceutical Sciences and Department of Pharmacology, Monash University, Parkville, Victoria 3052, Australia 3Clinical Pharmacology Unit, University of Cambridge, Cambridge, CB2 0QQ, UK 4School of Physiology, Pharmacology and Neuroscience, University of Bristol, Bristol, BS8 1TD, UK 5Medway School of Pharmacy, The Universities of Greenwich and Kent at Medway, Anson Building, Central Avenue, Chatham Maritime, Chatham, Kent, ME4 4TB, UK 6Neuroscience Division, Medical Education Institute, Ninewells Hospital and Medical School, University of Dundee, Dundee, DD1 9SY, UK 7Centre for Discovery Brain Sciences, University of Edinburgh, Edinburgh, EH8 9XD, UK Abstract The Concise Guide to PHARMACOLOGY 2019/20 is the fourth in this series of biennial publications. The Concise Guide provides concise overviews of the key properties of nearly 1800 human drug targets with an emphasis on selective pharmacology (where available), plus links to the open access knowledgebase source of drug targets and their ligands (www.guidetopharmacology.org), which provides more detailed views of target and ligand properties. Although the Concise Guide represents approximately 400 pages, the material presented is substantially reduced compared to information and links presented on the website. -

Pinning Down Neuropathic Pain
RESEARCH HIGHLIGHTS PAIN Pinning down neuropathic pain Neuropathic pain, a widespread promotes chronic pain through its calcium channels, possibly by induc- chronic condition caused by injury agonist action at bradykinin recep- ing bradykinin receptor coupling to to the nervous system, is one of the tors, could pave the way for new the Gs–cAMP–PKA pathway. most difficult syndromes to treat treatment options. Importantly, in vivo experiments successfully with Many experimental models of demonstrated that administration drugs. New thera- chronic pain show significant and of dynorphin A2–13 into the spinal peutic approaches to time-dependent regional elevation canal of rats induced reversible the treatment of this of dynorphin A, where it is known hypersensitivity and hyperalgesia, condition require a to mediate inhibitory effects on an effect that was not observed in better understanding pain regulation by binding to bradykinin-receptor-B2-knockout of the molecular opioid receptors. Dynorphin A also mice. In a model of neuropathic mechanisms mediates excitatory effects by an pain induced by spinal nerve that underlie its unknown mechanism. Now further ligation (SNL), the bradykinin development. Lai receptors for dynorphin A have been B2 antagonist HOE 140 led to a and colleagues, discovered. A des-tyrosyl fragment of reversal of the chronic pain state. reporting dynorphin A (dynorphin A2–13) with SNL induced time-dependent in Nature very low affinity for opioid receptors, upregulation of dynorphin, which Neuroscience, was shown to induce Ca2+ influx has a delayed onset and reached its have now by binding to B1 and B2 bradykinin peak 7–10 days after injury. -

The Role of Protein Convertases in Bigdynorphin and Dynorphin a Metabolic Pathway
Université de Montréal The Role of Protein Convertases in Bigdynorphin and Dynorphin A Metabolic Pathway par ALBERTO RUIZ ORDUNA Département de biomédecine vétérinaire Faculté de médecine vétérinaire Mémoire présenté à la Faculté de médecine vétérinaire en vue de l’obtention du grade de maître ès sciences (M.Sc.) en sciences vétérinaires option pharmacologie Décembre, 2015 © Alberto Ruiz Orduna, 2015 Résumé Les dynorphines sont des neuropeptides importants avec un rôle central dans la nociception et l’atténuation de la douleur. De nombreux mécanismes régulent les concentrations de dynorphine endogènes, y compris la protéolyse. Les Proprotéines convertases (PC) sont largement exprimées dans le système nerveux central et clivent spécifiquement le C-terminale de couple acides aminés basiques, ou un résidu basique unique. Le contrôle protéolytique des concentrations endogènes de Big Dynorphine (BDyn) et dynorphine A (Dyn A) a un effet important sur la perception de la douleur et le rôle de PC reste à être déterminée. L'objectif de cette étude était de décrypter le rôle de PC1 et PC2 dans le contrôle protéolytique de BDyn et Dyn A avec l'aide de fractions cellulaires de la moelle épinière de type sauvage (WT), PC1 -/+ et PC2 -/+ de souris et par la spectrométrie de masse. Nos résultats démontrent clairement que PC1 et PC2 sont impliquées dans la protéolyse de BDyn et Dyn A avec un rôle plus significatif pour PC1. Le traitement en C-terminal de BDyn génère des fragments peptidiques spécifiques incluant dynorphine 1-19, dynorphine 1-13, dynorphine 1-11 et dynorphine 1-7 et Dyn A génère les fragments dynorphine 1-13, dynorphine 1-11 et dynorphine 1-7. -

The Role of Dynorphin in the Onset of Puberty in Female Lambs
Graduate Theses, Dissertations, and Problem Reports 2015 The Role of Dynorphin in the Onset of Puberty in Female Lambs Justin Angelo Lopez Follow this and additional works at: https://researchrepository.wvu.edu/etd Recommended Citation Lopez, Justin Angelo, "The Role of Dynorphin in the Onset of Puberty in Female Lambs" (2015). Graduate Theses, Dissertations, and Problem Reports. 6110. https://researchrepository.wvu.edu/etd/6110 This Thesis is protected by copyright and/or related rights. It has been brought to you by the The Research Repository @ WVU with permission from the rights-holder(s). You are free to use this Thesis in any way that is permitted by the copyright and related rights legislation that applies to your use. For other uses you must obtain permission from the rights-holder(s) directly, unless additional rights are indicated by a Creative Commons license in the record and/ or on the work itself. This Thesis has been accepted for inclusion in WVU Graduate Theses, Dissertations, and Problem Reports collection by an authorized administrator of The Research Repository @ WVU. For more information, please contact [email protected]. The Role of Dynorphin in the Onset of Puberty in Female Lambs by Justin Angelo Lopez Thesis submitted to the Davis College of Agriculture, Natural Resources and Design at West Virginia University in partial fulfillment of the requirements for the degree of Master of Science in Reproductive Physiology Robert L. Goodman, Ph.D., Chair Stanley M. Hileman, Ph.D. Robert A. Dailey, Ph.D. Reproductive Physiology Morgantown, West Virginia 2015 Keywords: sheep, puberty, dynoprhin, kisspeptin, KNDy Copyright 2015 Justin Angelo Lopez ABSTRACT The Role of Dynorphin in the Onset of Puberty in Female Lambs Justin Angelo Lopez The neural mechanisms underlying the onset of puberty are not well understood. -

Calcitonin Gene-Related Peptide and Other Peptides
P1: KWW/KKL P2: KWW/HCN QC: KWW/FLX T1: KWW GRBT050-16 Olesen- 2057G GRBT050-Olesen-v6.cls July 9, 2005 4:30 ••Chapter 16 ◗ Calcitonin Gene-Related Peptide and Other Peptides Susan Brain and Lars Edvinsson Vasoactive peptides can be either stored or synthesized de THE CGRP FAMILY OF PEPTIDES novo before release from a range of tissues in the brain or from the walls of intracranial vasculature. In this chapter, The expression of mRNA from the calcitonin gene is tissue we concentrate on neuropeptides that are released from specific in that CGRP mRNA is predominantly expressed perivascular nerves. These include calcitonin gene-related in nerves and calcitonin mRNA in the thyroid (5). The 37 peptide (CGRP), substance P, neurokinin A, nociceptin, amino acid peptide CGRP belongs to a family that include somatostatin, and opioids (Table 16-1). The endothelium the more recently discovered peptides adrenomedullin produces the potent vasoconstrictors endothelin and an- that is primarily produced by non-neuronal tissues, espe- giotensin, and dilators such as nitric oxide, prostacyclin, cially vascular tissues and amylin that is mainly produced and endothelium-derived hyperpolarizing factors. In ad- in the pancreas. They share some structural homology (ap- dition there are circulating agents; among these the most proximately 25–40%) and also some, but not total, similar- potent is 5-hydroxytryptamine. The neuronal messengers ities in biological activities (see Brain and Grant [11] for stored in the intracranial vessels have been reviewed recent review). CGRP is abundant in the body and has a (32) and it was revealed that sympathetic nerves store wide distribution throughout the central and peripheral noradrenaline, neuropeptide Y, and ATP, the parasympa- nervous systems.