Sound Judgment: Choosing Effective Speech Therapy Techniques And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Brief Description of Consonants in Modern Standard Arabic
Linguistics and Literature Studies 2(7): 185-189, 2014 http://www.hrpub.org DOI: 10.13189/lls.2014.020702 A Brief Description of Consonants in Modern Standard Arabic Iram Sabir*, Nora Alsaeed Al-Jouf University, Sakaka, KSA *Corresponding Author: [email protected] Copyright © 2014 Horizon Research Publishing All rights reserved. Abstract The present study deals with “A brief Modern Standard Arabic. This study starts from an description of consonants in Modern Standard Arabic”. This elucidation of the phonetic bases of sounds classification. At study tries to give some information about the production of this point shows the first limit of the study that is basically Arabic sounds, the classification and description of phonetic rather than phonological description of sounds. consonants in Standard Arabic, then the definition of the This attempt of classification is followed by lists of the word consonant. In the present study we also investigate the consonant sounds in Standard Arabic with a key word for place of articulation in Arabic consonants we describe each consonant. The criteria of description are place and sounds according to: bilabial, labio-dental, alveolar, palatal, manner of articulation and voicing. The attempt of velar, uvular, and glottal. Then the manner of articulation, description has been made to lead to the drawing of some the characteristics such as phonation, nasal, curved, and trill. fundamental conclusion at the end of the paper. The aim of this study is to investigate consonant in MSA taking into consideration that all 28 consonants of Arabic alphabets. As a language Arabic is one of the most 2. -
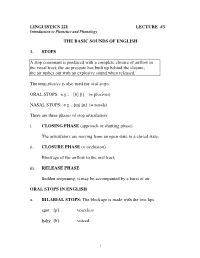
LINGUISTICS 221 LECTURE #3 the BASIC SOUNDS of ENGLISH 1. STOPS a Stop Consonant Is Produced with a Complete Closure of Airflow
LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology THE BASIC SOUNDS OF ENGLISH 1. STOPS A stop consonant is produced with a complete closure of airflow in the vocal tract; the air pressure has built up behind the closure; the air rushes out with an explosive sound when released. The term plosive is also used for oral stops. ORAL STOPS: e.g., [b] [t] (= plosives) NASAL STOPS: e.g., [m] [n] (= nasals) There are three phases of stop articulation: i. CLOSING PHASE (approach or shutting phase) The articulators are moving from an open state to a closed state; ii. CLOSURE PHASE (= occlusion) Blockage of the airflow in the oral tract; iii. RELEASE PHASE Sudden reopening; it may be accompanied by a burst of air. ORAL STOPS IN ENGLISH a. BILABIAL STOPS: The blockage is made with the two lips. spot [p] voiceless baby [b] voiced 1 b. ALVEOLAR STOPS: The blade (or the tip) of the tongue makes a closure with the alveolar ridge; the sides of the tongue are along the upper teeth. lamino-alveolar stops or Check your apico-alveolar stops pronunciation! stake [t] voiceless deep [d] voiced c. VELAR STOPS: The closure is between the back of the tongue (= dorsum) and the velum. dorso-velar stops scar [k] voiceless goose [g] voiced 2. NASALS (= nasal stops) The air is stopped in the oral tract, but the velum is lowered so that the airflow can go through the nasal tract. All nasals are voiced. NASALS IN ENGLISH a. BILABIAL NASAL: made [m] b. ALVEOLAR NASAL: need [n] c. -

8. Eligibility for Special Education Services A
8. Eligibility for Special Education Services a. Fact Sheets on i. ADHD Fact Sheet on Disabilities from NICHCY (http://nichcy.org/disability) ii. Autism Spectrum Disorders Fact Sheet iii. Blindness/Visual Impairment Fact Sheet iv. Cerebral Palsy Fact Sheet v. Deaf-Blindness Fact Sheet vi. Deafness and Hearing Loss Fact Sheet vii. Developmental Delay Fact Sheet viii. Down Syndrome Fact Sheet ix. Emotional Disturbance Fact Sheet x. Epilepsy Fact Sheet xi. Intellectual Disabilities Fact Sheet xii. Learning Disabilities Fact Sheet xiii. Other Health Impairment Fact Sheet xiv. Traumatic Brain Injury Fact Sheet b. Disability Worksheets for Eligibility for Special Education (from OSSE/DCPS) i. Other Health Impairment Disability Worksheet ii. Specific Learning Disability Worksheet iii. Emotional Disturbance Disability Worksheet Attention-Deficit/ Hyperactivity Disorder NICHCY Disability Fact Sheet #19 Updated March 2012 break down his lessons into gets to choose something fun several parts. Then they have he’d like to do. Having a him do each part one at a child with AD/HD is still a Mario’s Story time. This helps Mario keep challenge, but things are his attention on his work. looking better. Mario is 10 years old. When he was 7, his family At home, things have learned he had AD/HD. At changed, too. Now his What is AD/HD? the time, he was driving parents know why he’s so everyone crazy. At school, he active. They are careful to Attention-deficit/hyperac- couldn’t stay in his seat or praise him when he does tivity disorder (AD/HD) is a keep quiet. At home, he something well. -

Medically Necessary Orthodontic Treatment – Dental
UnitedHealthcare® Dental Coverage Guideline Medically Necessary Orthodontic Treatment Guideline Number: DCG003.08 Effective Date: November 1, 2020 Instructions for Use Table of Contents Page Related Medical Policy Coverage Rationale ....................................................................... 1 • Orthognathic (Jaw) Surgery Definitions ...................................................................................... 1 Applicable Codes .......................................................................... 3 Description of Services ................................................................. 3 References ..................................................................................... 3 Guideline History/Revision Information ....................................... 4 Instructions for Use ....................................................................... 4 Coverage Rationale Orthodontic treatment is medically necessary when the following criteria have been met: All services must be approved by the plan; and The member is under the age 19 (through age 18, unless the member specific benefit plan document indicates a different age); and Services are related to the treatment of a severe craniofacial deformity that results in a physically Handicapping Malocclusion, including but not limited to the following conditions: o Cleft Lip and/or Cleft Palate; o Crouzon Syndrome/Craniofacial Dysostosis; o Hemifacial Hypertrophy/Congenital Hemifacial Hyperplasia; o Parry-Romberg Syndrome/Progressive Hemifacial Atrophy; -

Research Article
z Available online at http://www.journalcra.com INTERNATIONAL JOURNAL OF CURRENT RESEARCH International Journal of Current Research Vol. 10, Issue, 07, pp.71222-71228, July, 2018 ISSN: 0975-833X RESEARCH ARTICLE THE TONGUE SPEAKS A LOT OF HEALTH. 1,*Dr. Firdous Shaikh, 2Dr. Sonia Sodhi, 3Dr Zeenat Fatema Farooqui and 4Dr. Lata Kale 1PG Student, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad 2Professor, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad 3Fatema Farooqui, Chief Medical Officer, Sri Ram Homeopathic Clinic and Research Center, Solapur 4Professor and Head, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad ARTICLE INFO ABSTRACT Article History: Multifunctional organ of the human body without a bone yet strong is the tongue. It mainly consists Received 26th April, 2018 of the functional portion of muscle mass, mucosa, fat and the specialized tissue of taste i.e. the Received in revised form papillae. Diseases may either result from internal/ systemic causes of extrinsic causes like trauma, 14th May, 2018 infection, etc. A new method for classification has been proposed in this review for diseases of Accepted 09th June, 2018 tongue. This review mainly focuses on encompassing almost each aspect that the body reflects via its th Published online 30 July, 2018 mirror in mouth, the tongue. Key Words: Tongue, Diseases of Tongue, Discoloration of Tongue, Oral health, Hairy Tongue. Copyright © 2018, Firdous Shaikh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -

Medical Science 2321–7367
ANALYSISANALYSIS ARTICLE 24(106), November - December, 2020 ISSN 2321–7359 EISSN Medical Science 2321–7367 Diagnostic value of five cephalometric analysis in recognition of class I, II, and III sagittal patterns Abdolmohammad Gachkooban1, Mina Moalemnia2 1Assistant Professor, Department of Orthodontics, School of Dentistry, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. 2Graduate Resident, Department of Restorative Dentistry, School of Dentistry, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran Corresponding author Department of Restorative Dentistry, School of Dentistry, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran. Email: [email protected] Article History Received: 21 September 2020 Reviewed & Revised: 22/September/2020 to 31/October/2020 Accepted: 31 October 2020 E-publication: 10 November 2020 P-Publication: November - December 2020 Citation Abdolmohammad Gachkooban, Mina Moalemnia. Diagnostic value of five cephalometric analysis in recognition of class I, II, and III sagittal patterns. Medical Science, 2020, 24(106), 4116-4124 Publication License This work is licensed under a Creative Commons Attribution 4.0 International License. General Note Article is recommended to print as color digital version in recycled paper. ABSTRACT Background and Objective: Controversy exists over superiority of cephalometric analyses in diagnosis of skeletal classes. The aim of the present study was to compare diagnostic value of cephalometric analyses of class I, II, III anteroposterior jaw discrepancies. 4116 Materials and methods: A total of 90 cephalographs (n=90×3) were retrieved from the database of radiological clinic and classified into three study groups: Group I (Class I, n=30), Group II (Class II, n=30), and Group III (Class III, n=30). The cephalographs were Page traced manually. -

Disease/Medical Condition
Disease/Medical Condition HYPOTHYROIDISM Date of Publication: January 27, 2017 (also known as “underactive thyroid disease”; includes congenital hypothyroidism [also known as “neonatal hypothyroidism”] and Hashimoto’s thyroiditis [also known as “autoimmune thyroiditis”]; may manifest as “cretinism” [if onsets during fetal or early life; also known as “congenital myxedema”] or “myxedema” [if onset occurs in older children and adults]) Is the initiation of non-invasive dental hygiene procedures* contra-indicated? No. ◼ Is medical consult advised? – Yes, if previously undiagnosed hypothyroidism or enlarged (or shrunken) thyroid gland is suspected1, in which case the patient/client should see his/her primary care physician. Detection early in childhood can prevent permanent intellectual impairment. – Yes, if previously diagnosed hypothyroidism is suspected to be undermedicated (with manifest signs/symptoms of hypothyroidism) or overmedicated (with manifest signs/symptoms of hyperthyroidism2), in which case the patient/client should see his/her primary care physician or endocrinologist. Major stress or illness sometimes necessitates an increase in prescribed thyroid hormone. Is the initiation of invasive dental hygiene procedures contra-indicated?** Possibly, depending on the certainty of diagnosis and level of control. ◼ Is medical consult advised? – See above. ◼ Is medical clearance required? – Yes, if undiagnosed or severe hypothyroidism is suspected. ◼ Is antibiotic prophylaxis required? – No. ◼ Is postponing treatment advised? – Yes, if undiagnosed hypothyroidism is suspected (necessitating medical assessment/management) or severe hypothyroidism is suspected (necessitating urgent medical assessment/management in order to avoid risk of myxedema coma). In general, the patient/client with mild symptoms of untreated hypothyroidism is not in danger when receiving dental hygiene therapy, and the well managed (euthyroid) patient/client requires no special regard. -

Orofacial Myology Is a Specialized Professional Discipline That Evaluates and Treats a Variety Of
What is Orofacial Myology? Orofacial myology is a specialized professional discipline that evaluates and treats a variety of oral and facial (orofacial) muscles, (myo-) postural and functional disorders and oral habits that may disrupt normal dental development and also create cosmetic problems. The principles involved with the evaluation and treatment of orofacial Myofunctional disorders are based upon dental science tenets; however, orofacial Myofunctional therapy is not dental treatment. Myofunctional therapy can be basically described as correcting an oro-facial muscular unbalance, including correction of the position of the tongue at rest and during swallowing. Specific treatments involve establishing and stabilizing normal rest position of the tongue and lips, eliminating deviate (abnormal) oral habits and correcting swallowing patterns when tongue thrusting is involved. Improvements in appearance are observed during and following therapy. What are Myofunctional disorders and how are they corrected? An oral Myofunctional disorder includes a variety of oral habits, postures and functional activities that may open the normal dental bite or may lead to deformation of the dental arches. • Thumb and finger sucking • an open-mouth posture with lips apart • a forward rest posture of the tongue • Tongue thrusting during speaking and swallowing Above mentioned oral habits characterize Myofunctional disorders. Such disorders can lead to a disruption of normal dental development in both children and adults. The consequence of postural and functional variations involving the lips and tongue are associated with dental malocclusion, cosmetic problems, and deformities in the growth of the dental arches. How Prevalent Are Orofacial Myofunctional Disorders (OMD)? Research examining various populations found 38% have orofacial Myofunctional disorders and, as mentioned above, an incidence of 81% has been found in children exhibiting speech/articulation problems. -

Singing in English in the 21St Century: a Study Comparing
SINGING IN ENGLISH IN THE 21ST CENTURY: A STUDY COMPARING AND APPLYING THE TENETS OF MADELEINE MARSHALL AND KATHRYN LABOUFF Helen Dewey Reikofski Dissertation Prepared for the Degree of DOCTOR OF MUSICAL ARTS UNIVERSITY OF NORTH TEXAS August 2015 APPROVED:….……………….. Jeffrey Snider, Major Professor Stephen Dubberly, Committee Member Benjamin Brand, Committee Member Stephen Austin, Committee Member and Chair of the Department of Vocal Studies … James C. Scott, Dean of the College of Music Costas Tsatsoulis, Interim Dean of the Toulouse Graduate School Reikofski, Helen Dewey. Singing in English in the 21st Century: A Study Comparing and Applying the Tenets of Madeleine Marshall and Kathryn LaBouff. Doctor of Musical Arts (Performance), August 2015, 171 pp., 6 tables, 21 figures, bibliography, 141 titles. The English diction texts by Madeleine Marshall and Kathryn LaBouff are two of the most acclaimed manuals on singing in this language. Differences in style between the two have separated proponents to be primarily devoted to one or the other. An in- depth study, comparing the precepts of both authors, and applying their principles, has resulted in an understanding of their common ground, as well as the need for the more comprehensive information, included by LaBouff, on singing in the dialect of American Standard, and changes in current Received Pronunciation, for British works, and Mid- Atlantic dialect, for English language works not specifically North American or British. Chapter 1 introduces Marshall and The Singer’s Manual of English Diction, and LaBouff and Singing and Communicating in English. An overview of selected works from Opera America’s resources exemplifies the need for three dialects in standardized English training. -

Speech/Language Impairment Sheet
West Virginia State Department of Education Office of Special Education * 1-800-558-2696 * http://wvde.state.wv.us/osp/ Fact Speech/Language Impairment Sheet DEFINITION Voice: Speech impairment where the child’s voice has an IDEA defines a speech or language impairment as a abnormal quality of pitch, resonance, or loudness. communication disorder, such as stuttering, impaired articulation, a language impairment, or a voice Persistent voice issues can indicate problems such as impairment that adversely affects a child’s educational vocal cord nodules, which should be addressed. Some performance. students who have structural abnormalities, such as cleft palate or palatal insufficiency, may exhibit a nasal SPEECH DISORDERS sound to their speech. An otolaryngologist must verify Speech Sound Disorders: Speech impairment where the the absence or existence of structural or functional child has difficulty producing sounds. Most children pathology before voice therapy can be provided. make some mistakes as they learn to say new words. A speech sound disorder occurs when mistakes continue Dysphagia: Some children may have difficulty eating past a certain age. Every sound has a different range of (chewing and swallowing food) and drinking without ages when the child should make the sound correctly. aspiration. The speech-language pathologist may be involved in developing a plan, along with other team Speech sound disorders include problems with members, to ensure that the child is provided with safe articulation (making sounds) and phonological nourishment and hydration during school hours. processes (patterns of sounds). COMMUNICATION DISORDERS Sounds can be substituted (saying “tat” for “cat”), left Augmentative and Alternative Communication: the use off (saying “ca” instead of “cat”), added (saying “kwat” of an alternative to speaking as a substitute for speech instead of “cat”) or changed (saying the sound or to supplement speech. -

Of Elves and Men Simon J
Journal of Tolkien Research Volume 3 | Issue 1 Article 1 2016 Fantasy Incarnate: Of Elves and Men Simon J. Cook Dr. None, [email protected] Follow this and additional works at: http://scholar.valpo.edu/journaloftolkienresearch Part of the Esthetics Commons, Intellectual History Commons, and the Literature in English, British Isles Commons Recommended Citation Cook, Simon J. Dr. (2016) "Fantasy Incarnate: Of Elves and Men," Journal of Tolkien Research: Vol. 3: Iss. 1, Article 1. Available at: http://scholar.valpo.edu/journaloftolkienresearch/vol3/iss1/1 This Peer-Reviewed Article is brought to you for free and open access by the Library Services at ValpoScholar. It has been accepted for inclusion in Journal of Tolkien Research by an authorized administrator of ValpoScholar. For more information, please contact a ValpoScholar staff member at [email protected]. Cook: Fantasy Incarnate Fantasy Incarnate: Of Elves and Men Introduction The following essay arises out of sustained engagement with the section of J.R.R. Tolkien’s On Fairy Stories entitled ‘Origins’. This section is dense, often elliptical, sometimes cryptic, with depths that have yet to be plumbed. It defies easy exegesis. My attempt to understand the ideas behind the text have led me far afield – into other sections of the essay, into other writings by Tolkien, and into works by other scholars which, in varying degrees, illuminate Tolkien’s thought. I have yet to exhaust this material and more remains to be said. What fruit I now present from my exegetical labour boils down to two claims: that loss of historical memory plays a vital role in Tolkien’s account of mythology, and that the notion of incarnation provides a key to his conception of fantasy.1 The essay consists of four main sections. -

Locutour Guide to Letters, Sounds, and Symbols
LOCUTOUROUR® Guide to Letters, Sounds, and Symbols LOCUTOUR ABEL LASSIFICATION LACE OR RTICULATION PELLED AS XAMPLES S PELLINGP E L L I N G L C P A IPA S E Consonants p bilabial plosive voiceless lips /p/ p, pp pit, puppy b bilabial plosive voiced lips /b/ b, bb bat, ebb t lingua-alveolar plosive voiceless tongue tip + upper gum ridge /t/ t, ed, gth, th, tt, tw tan, tipped, tight, thyme, attic, two d lingua-alveolar plosive voiced tongue tip + upper gum ridge /d/ d, dd, ed dad, ladder, bagged k lingua-velar plosive voiceless back of tongue and soft palate /k/ c, cc, ch, ck cab, occur, school, duck que, k mosque, kit g lingua-velar plosive voiced back of tongue and soft palate /g/ g, gg, gh, gu, gue hug, bagged, Ghana, guy, morgue f labiodental fricative voiceless lower lip + upper teeth /f/ f, ff , gh, ph feet, fl u uff, enough, phone v labiodental fricative voiced lower lip + upper teeth /v/ v, vv, f, ph vet, savvy, of, Stephen th linguadental fricative voiceless tongue + teeth /T/ th thin th linguadental fricative voiced tongue + teeth /D/ th, the them, bathe s lingua-alveolar fricative voiceless tongue tip + upper gum ridge or /s/ s, ss, sc, ce, ci, sit, hiss, scenic, ace, city tongue tip + lower gum ridge cy, ps, z cycle, psychology, pizza z lingua-alveolar fricative voiced tongue tip + upper gum ridge or /z/ z, zz, s, ss, x, cz Zen, buzz, is, scissors, tongue tip + lower gum ridge Xerox, czar sh linguapalatal fricative voiceless tongue blade and hard palate /S/ sh, ce, ch, ci, sch, si, sheep, ocean, chef, glacier, kirsch ss, su,