Shiftwork an Annotated Bibliography
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Deep Network for Nychthemeron Cloud Image Segmentation
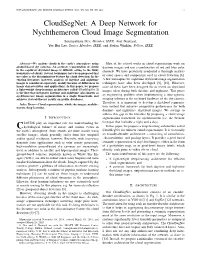
IEEE GEOSCIENCE AND REMOTE SENSING LETTERS, VOL. XX, NO. XX, XX 2019 1 CloudSegNet: A Deep Network for Nychthemeron Cloud Image Segmentation Soumyabrata Dev, Member, IEEE, Atul Nautiyal, Yee Hui Lee, Senior Member, IEEE, and Stefan Winkler, Fellow, IEEE Abstract—We analyze clouds in the earth’s atmosphere using Most of the related works in cloud segmentation work on ground-based sky cameras. An accurate segmentation of clouds daytime images and use a combination of red and blue color in the captured sky/cloud image is difficult, owing to the fuzzy channels. We have previously conducted a thorough analysis boundaries of clouds. Several techniques have been proposed that use color as the discriminatory feature for cloud detection. In the of color spaces and components used in cloud detection [8]. existing literature, however, analysis of daytime and nighttime A few techniques for nighttime sky/cloud image segmentation images is considered separately, mainly because of differences in techniques have also been developed [9], [10]. However, image characteristics and applications. In this paper, we propose none of them have been designed for or tested on sky/cloud a light-weight deep-learning architecture called CloudSegNet. It images taken during both daytime and nighttime. This poses is the first that integrates daytime and nighttime (also known as nychthemeron) image segmentation in a single framework, and an engineering problem when implementing a time-agnostic achieves state-of-the-art results on public databases. imaging solution in the on-board hardware of the sky camera. Therefore, it is important to develop a sky/cloud segmenta- Index Terms—Cloud segmentation, whole sky imager, nychthe- meron, deep learning. -

Chronobiology Meets Work Life Chronotype-Dependent Nap Behaviour and Light Exposure on Work- and Free Days
Aus dem Institut für Medizinische Psychologie der Ludwig-Maximilians-Universität München Vorstand: Frau Univ. Prof. Dr. Martha Merrow Chronobiology Meets Work Life Chronotype-dependent nap behaviour and light exposure on work- and free days Dissertation zum Erwerb des Doktorgrades der Humanbiologie an der Medizinischen Fakultät der Ludwig-Maximilians-Universität zu München vorgelegt von Joana Leonie Matera aus Koblenz Jahr 2015 Mit Genehmigung der Medizinischen Fakultät der Universität München Berichterstatter: Prof. Dr. Till Roenneberg Mitberichterstatter: Priv. Doz. Dr. Matthias Weigl Priv. Doz. Dr. Jan Rémi Mitbetreuung durch den promovierten MitarBeiter: Dekan: Prof. Dr. Reinhard Hickel Tag der mündlichen Prüfung: 05.11.2015 2 ! 9(;-//.5..)(=#-!Y-$/(=#-$7&*! ! ! ! A=#@!H%5&5!2-%&(-!,5.-$5@!-$1)?$-!#(-$8(.!5&!9(;-/!/.5..@!;5//!(=#!;(-!G%$)(-*-&;-! 4(//-$.5.(%&!8(.!;-8!X#-85S! ! "#$%&%'(%)%*+!,--./!0%$1!2(3-! !"#$%$&'()*+)()%+)%&,%-(,.)"-/0$1#,-%+,203"&,)4($51#), $%,6$#7*,-%+,8#)),+-'5, ! ! /-)'/.?&;(*! G-$35//.@! 8(=#! 57Z-$! ;-$! 5&*-*-'-&-&! 1-(&-$! :-(.-$-&! <()3/8(..-)! '-;(-&.! 7&;! 5))-! 9$1-&&.&(//-@! ;(-! 57/! ;-8! [=#$(3..78! *5&6! %;-$! 5&&?#-$&;! B'-$&%88-&!/(&;@!5)/!/%)=#-!1-&&.)(=#!*-85=#.!7&;!&5=#!(#$-$!<-$17&3.!7&.-$! R-6-(=#&7&*!;-$!>7&;/.-))-!-(&6-)&!&5=#*-:(-/-&!#5'-K!! ! A=#!-$1)?$-!;-/!0-(.-$-&@!;5//!;(-!#(-$!G%$*-)-*.-!4(//-$.5.(%&!&(=#.!(&!*)-(=#-$! %;-$! (&! ?#&)(=#-$! >%$8! '-(! -(&-$! 5&;-$-&! [.-))-! 67$! 9$)5&*7&*! -(&-/! 515;-8(/=#-&!Q$5;-/!-(&*-$-(=#.!:7$;-K! ! ! ,B&=#-&@!\IK\]K^\I_! ! ! ! TTTTTTTTTTTTTTTTTTTTTTTTTTTTTTTTTTTT! -
The Architecture of Joseph Michael Gandy (1771-1843) and Sir John Soane (1753-1837): an Exploration Into the Masonic and Occult Imagination of the Late Enlightenment
University of Pennsylvania ScholarlyCommons Publicly Accessible Penn Dissertations 2003 The Architecture of Joseph Michael Gandy (1771-1843) and Sir John Soane (1753-1837): An Exploration Into the Masonic and Occult Imagination of the Late Enlightenment Terrance Gerard Galvin University of Pennsylvania Follow this and additional works at: https://repository.upenn.edu/edissertations Part of the Architecture Commons, European History Commons, Social and Behavioral Sciences Commons, and the Theory and Criticism Commons Recommended Citation Galvin, Terrance Gerard, "The Architecture of Joseph Michael Gandy (1771-1843) and Sir John Soane (1753-1837): An Exploration Into the Masonic and Occult Imagination of the Late Enlightenment" (2003). Publicly Accessible Penn Dissertations. 996. https://repository.upenn.edu/edissertations/996 This paper is posted at ScholarlyCommons. https://repository.upenn.edu/edissertations/996 For more information, please contact [email protected]. The Architecture of Joseph Michael Gandy (1771-1843) and Sir John Soane (1753-1837): An Exploration Into the Masonic and Occult Imagination of the Late Enlightenment Abstract In examining select works of English architects Joseph Michael Gandy and Sir John Soane, this dissertation is intended to bring to light several important parallels between architectural theory and freemasonry during the late Enlightenment. Both architects developed architectural theories regarding the universal origins of architecture in an attempt to establish order as well as transcend the emerging historicism of the early nineteenth century. There are strong parallels between Soane's use of architectural narrative and his discussion of architectural 'model' in relation to Gandy's understanding of 'trans-historical' architecture. The primary textual sources discussed in this thesis include Soane's Lectures on Architecture, delivered at the Royal Academy from 1809 to 1836, and Gandy's unpublished treatise entitled the Art, Philosophy, and Science of Architecture, circa 1826. -
15 May, 30 Villages Throughout the Country Theatre Performance For
9 April - 15 May, 30 villages throughout the country Theatre performance for children: “Let me tell you a secret about the environment” Children’s Theatre Centre, Skopje (Brvenica & Sedlarce, Mlado Nagorichane & Staro Nagorichane, Chegrane & Forino, Vasilevo & Dobreici, Vatasha & Sopot, Bistrica & Kravari, Gorno Orizari, Kochilari, Leskoec & Kosel, Mogorche & Dolno Kosovrasti, Konopnica & Mozhdivnjak, Negorci & Mrzenci, Orizari, Istibanje, Ratevo & Rusinovo, Veleshta & Dobovjan and Topolcani & Kanatlarci) 20 April - Friday, 11:00-13.00 EU InfoCentre, Skopje Launching Event of EU funded cartoons: “We love Europe” Business Solutions Europa 23 April - Monday, 10:30-11:30 EU InfoCentre Press Conference on the Europe Day celebration activities 25 April - Wednesday, 14:00-16:00 Aerodrom Municipality, Skopje Drawing competition: “Europe for all generations” European Movement, Aerodrom Municipality 27 April - Friday, 12:00-14:00 Kumanovo Municipality Panel discussion: “European integration from the economic and security perspective” European Movement 30 April - Monday, Secondary schools throughout the country Open classrooms for older generations Ministry of Education and Science 30 April - Monday, Secondary schools throughout the country Essay Competition: “Why is it cool to be old?” Ministry of Education and Science 30 April - Monday, 12:00-14:00 Bitola Municipality Panel discussion: “European integration from the local perspective” European Movement 4 May - Friday, 09:30-15:00 ”Sv. Kiril i Metodij” University, Skopje Gathering of universities -

MACEDONIAN FILM NEWS FILMS RELEASED 2017/2018 FEATURE DOCUMENTARIES SHORT ANIMATIONS - No.1 - FESTIVAL DE CANNES 8-19 MAY 2018
MACEDONIAN FILM NEWS FILMS RELEASED 2017/2018 FEATURE DOCUMENTARIES SHORT ANIMATIONS www.filmagency.gov.mk - No.1 - FESTIVAL DE CANNES 8-19 MAY 2018 Address: 8 Mart no.4 Tel: + 389 2 3224 100 E-mail: contact@filmagency.gov.mk, Official page: www.filmagency.gov.mk MACEDONIAN FILMS RELEASED 2017 / 2018 FEATURE FILMS - NATIONAL PRODUCTION ГОДИНА НА МАЈМУНОТ THE YEAR OF THE MONKEY Director: Vladimir Blazevski Producer: Darko Popov Screenwriter: Vladimir Blazevski A mild political satire about a peculiar friendship between a lonely chimpanzee and an Director of Photography: Dimo Popov impoverished zoo warden, The Year of the Monkey is set in an upside-down world stuck in Editor: Blagoja Nedelkovski RELEASED transition - as seen through the eyes of the chimp, who escapes the zoo to become a rebel Sound Designer: Sasho Kalan hero in the harsh environment of the Balkans. Music Composer: Aleksandar Pejovski Cast: Igor Angelov, Behreda Reshit, Marija Kohn, Faik Mefailovski, Elena Trajkovska, Chun Lajchi www.pankfilm.mk MK, RS, SI, XK | 2018 | 109' | DCP | Black Comedy | Produced by Punk Film (MK) Co-pro- pankfi[email protected] duced by Kiselo Dete (RS), Strup (SI), Infinity (XK) The activities of the Macedonian Film Agency in recent years have mainly been focussed on supporting the production of ВРАЌАЊЕ THE RETURN Director: Kastriot Abdyli films. Other activities have included the organisation of film Producer: Kastriot Abdyli This contemporary story takes place in a Balkan village where the old and the new, Screenwriter: Kastriot Abdyli Co-Writer: Isa Qosja the traditional and the modern, eastern and western, all intertwine. Ilir, a young Alba- RELEASED festivals and the promotion of Macedonian film at international Director of Photography: Vladimir nian man from Macedonia who migrated to France, has decided to marry a French festivals and events, as well as international cooperation and Samoilovski woman by the name of Sabine (perhaps out of love, but perhaps also to secure his Production Design: Zeni Ballazhi encouraging the development of film professionals. -

Cornell Alumni Magazine, NY, and Additional Mail C/O Public Affairs Records, 130 East Seneca St., Suite 400, Ithaca, NY 14850-4353
c1-c4CAMjf11 12/16/10 10:18 AM Page c1 January | February 2011 $6.00 Alumni Corne Magazine Ghost World Photos Bridge Ithaca’s Past and Present cornellalumnimagazine.com c1-c4CAMjf11 12/16/10 10:18 AM Page c2 001-001CAMjf11toc 12/17/10 10:35 AM Page 1 January / February 2011 Volume 113 Number 4 In This Issue Corne Alumni Magazine 4 2 From David Skorton Money matters 4 The Big Picture A big blow-up 6 Correspondence Suicide prevention 9 Letter from Ithaca Shirt off their backs 10 From the Hill Oh, the humanities! 14 Sports Wrestle mania 17 Authors It’s all right 24 Summer Programs and Sports Camps 20 40 Wines of the Finger Lakes Swedish Hill Cynthia Marie Port 54 Classifieds & Cornellians in Business 55 Alma Matters 58 Class Notes 95 Alumni Deaths 48 96 Cornelliana 42 Through a Glass, Darkly Conserving a conservatory? FRANKLIN CRAWFORD Urban renewal was kinder to Ithaca than to some Upstate cities, but over the past cen- Currents tury many stately buildings have still been lost—from Ezra Cornell’s Free Circulating Library to Alonzo Cornell’s mansion to the grand old Strand Theatre. In a series of photos recently exhibited at the History Center of Tompkins County, former visiting professor Mark Iwinski captures the ghostly images of bygone structures superimposed 20 Flour Power over what stands in their place. Often, it isn’t pretty. Milling the old-fashioned way Starry Nights 48 Vegging In Cosmic storyteller BETH SAULNIER Eat Different Promoting a plant-based diet When the Moosewood Restaurant served its first meal thirty-eight years ago this month, the owners were still trying to figure out how to run the steam table (and the entrée Learning Curve was two hours late). -

Western Corn Rootworm (Diabrotica Virgifera Virgifera Leconte) in Europe: Current Status and Sustainable Pest Management
insects Review Western Corn Rootworm (Diabrotica virgifera virgifera LeConte) in Europe: Current Status and Sustainable Pest Management Renata Bažok 1 , Darija Lemi´c 1 , Francesca Chiarini 2 and Lorenzo Furlan 2,* 1 Department for Agricultural Zoology, Faculty of Agriculture, University of Zagreb, Svetosimunska 25, 10000 Zagreb, Croatia; [email protected] (R.B.); [email protected] (D.L.) 2 Veneto Agricoltura, Agricultural Research Department, 35020 Legnaro, PD, Italy; [email protected] * Correspondence: [email protected]; Tel.: +39-049-829-3879 Simple Summary: Diabrotica virgifera virgifera, also known as western corn rootworm (WCR), is a maize-specific pest that has been a serious threat in Europe since the mid-1990s. Between 1995 and 2010, European countries were involved in international projects to plan pest control strategies. However, since 2011, collaborative efforts have declined and the overview of knowledge on WCR is in great need of updating. Therefore, a review of scientific papers published between 2008 and 2020, in addition to direct interviews with experts responsible for WCR management in several European countries, was conducted to (1) summarize the research conducted over the last 12 years and (2) describe the current WCR distribution and population in the EU, and the management strategies implemented. A considerable amount of new knowledge has been gained over the last 12 years, which has contributed to the development of pest management strategies applicable in EU agricultural systems. There is no EU country reporting economic damage on a large scale. In many countries, solutions based on crop rotation are regularly implemented, avoiding insecticide Citation: Bažok, R.; Lemi´c,D.; use. -

Self-Regulation and Sleep Duration, Sleepiness, and Chronotype in Adolescents Judith A
Self-Regulation and Sleep Duration, Sleepiness, and Chronotype in Adolescents Judith A. Owens, MD, MPH, a Tracy Dearth-Wesley, PhD, MPH,b Daniel Lewin, PhD, c Gerard Gioia, PhD,d Robert C. Whitaker, MD, MPHb, e, f OBJECTIVE: To determine whether shorter school-night sleep duration, greater daytime abstract sleepiness, and greater eveningness chronotype were associated with lower self-regulation among adolescents. METHODS: An online survey of 7th- to 12th-grade students in 19 schools in Fairfax County, Virginia Public Schools was conducted in 2015. Self-regulation was measured with the Behavior Rating Inventory of Executive Function, 2nd edition, Screening Self-Report Form. Sleep measures included school night-sleep duration (hours between usual bedtime and wake time), daytime sleepiness (Sleepiness Scale in the Sleep Habits Survey, tertiles), and chronotype (Morningness–Eveningness Scale for Children, continuous score and tertiles). Sociodemographic factors and mental health conditions were analyzed as potential confounders. RESULTS: Among 2017 students surveyed, the mean age was 15.0 years (range, 12.1–18.9 years), and 21.7% slept <7 hours on school nights. In regression models adjusted for confounders, there was a significant independent association between self-regulation and both chronotype (P < .001) and daytime sleepiness (P < .001) but not sleep duration (P = .80). Compared with those in the lowest tertile of daytime sleepiness, those in the highest tertile had lower (0.59 SD units; 95% confidence interval, 0.48–0.71) self-regulation, as did those in the eveningness tertile of chronotype compared with those in the morningness tertile (0.35 SD units lower; 95% confidence interval, 0.24–0.46). -

Macedonian Films 2016/2017
MACEDONIAN FILMS 2016/2017 Through its activities over the years, the Macedonian success is yet further confirmation of the efforts of the Macedonian Film Agency, which are directed Film Agency has striven to provide comprehensive towards collaborations and partnerships in the interest of creating quality film projects that will funding for the Macedonian film industry and helped be worthy representatives of Macedonian cinematography. In the interests of promoting the latest to further develop and stimulate film production, film production, the Cannes Film Festival - Marche du film will traditionally host screenings of the international co-productions, film distribution, cinema following upcoming Macedonian films: The Year of the Monkey by Vladimir Blazevski (MK/RS/SI/ networks and film festivals, as well as encouraging the XK), Secret Ingredient by Gjorce Stavreski (MK/GR), and When the Day Had No Name by Teona writing of scripts, promoting the professional education Strugar Mitevska (MK/SI/BE) - a film which entered the official programme of this year’s Berlin of film professionals and promoting Macedonian International Film Festival. cinematography at renowned international film festivals and events by offering favourable conditions We hope that the projects presented on the following pages will attract your attention by offering a to foreign producers, thereby also promoting the Republic of Macedonia as a filming location. unique insight into Macedonian cinematography, Macedonian film professionals and the possibilities The Film Production -
A Comparison of Circadian Rhythms in Day and Night Shift Workers
Portland State University PDXScholar Dissertations and Theses Dissertations and Theses 1990 A comparison of circadian rhythms in day and night shift workers Mary Lee Blood Portland State University Follow this and additional works at: https://pdxscholar.library.pdx.edu/open_access_etds Part of the Physiology Commons, and the Psychology Commons Let us know how access to this document benefits ou.y Recommended Citation Blood, Mary Lee, "A comparison of circadian rhythms in day and night shift workers" (1990). Dissertations and Theses. Paper 3991. https://doi.org/10.15760/etd.5875 This Thesis is brought to you for free and open access. It has been accepted for inclusion in Dissertations and Theses by an authorized administrator of PDXScholar. Please contact us if we can make this document more accessible: [email protected]. AN ABSTRACT OF THE THESIS OF Mary Lee Blood for the Master of Science in Psychology presented October 29, 1990. Title: A Comparison of Circadian Rhythms in Day and Night Shift Workers. APPROVED BY THE MEMBERS OF THE THESIS COMMITTEE: Cord B. Sengstake, Chair Alfred J. Lewy Robert L. Sack Gary Brodowicz The present study examined whether and to what extent physiological rhythms of long-term . night workers become adapted to their unconventionally scheduled hours of work and sleep and how 2 the degree of adaptation would be reflected in ratings of sleep quality, mood, anxiety, energy and satisfaction. Many physiological functions such as the release of hormones, excretion of metabolites and fluctuation of core temperature follow predictable circadian (24-hour) rhythms that are regulated by a pacemaker thought to be located in the suprachiasmatic nucleus (SCN) of the hypothalamus. -

Download File
Eastern European Modernism: Works on Paper at the Columbia University Libraries and The Cornell University Library Compiled by Robert H. Davis Columbia University Libraries and Cornell University Library With a Foreword by Steven Mansbach University of Maryland, College Park With an Introduction by Irina Denischenko Georgetown University New York 2021 Cover Illustration: No. 266. Dvacáté století co dalo lidstvu. Výsledky práce lidstva XX. Věku. (Praha, 1931-1934). Part 5: Prokroky průmyslu. Photomontage wrappers by Vojtěch Tittelbach. To John and Katya, for their love and ever-patient indulgence of their quirky old Dad. Foreword ©Steven A. Mansbach Compiler’s Introduction ©Robert H. Davis Introduction ©Irina Denischenko Checklist ©Robert H. Davis Published in Academic Commons, January 2021 Photography credits: Avery Classics Library: p. vi (no. 900), p. xxxvi (no. 1031). Columbia University Libraries, Preservation Reformatting: Cover (No. 266), p.xiii (no. 430), p. xiv (no. 299, 711), p. xvi (no. 1020), p. xxvi (no. 1047), p. xxvii (no. 1060), p. xxix (no. 679), p. xxxiv (no. 605), p. xxxvi (no. 118), p. xxxix (nos. 600, 616). Cornell Division of Rare Books & Manuscripts: p. xv (no. 1069), p. xxvii (no. 718), p. xxxii (no. 619), p. xxxvii (nos. 803, 721), p. xl (nos. 210, 221), p. xli (no. 203). Compiler: p. vi (nos. 1009, 975), p. x, p. xiii (nos. 573, 773, 829, 985), p. xiv (nos. 103, 392, 470, 911), p. xv (nos. 1021, 1087), p. xvi (nos. 960, 964), p. xix (no. 615), p. xx (no. 733), p. xxviii (no. 108, 1060). F.A. Bernett Rare Books: p. xii (nos. 5, 28, 82), p. -

A Neglected Argument for the Reality of God - Wikisource 9/2/10 5:08 PM
A Neglected Argument for the Reality of God - Wikisource 9/2/10 5:08 PM A Neglected Argument for the Reality of God From Wikisource A Neglected Argument for the Reality of God by Charles Sanders Peirce 1908 [Footnote and links not in original] A NEGLECTED ARGUMENT FOR THE REALITY OF GOD. C. S. PEIRCE. I. THE word "God," so "capitalised" (as we Americans say), is the definable proper name, signifying Ens necessarium[1]; in my belief Really creator of all three Universes of Experience. Some words shall herein be capitalised when used, not as vernacular, but as terms defined. Thus an "idea" is the substance of an actual unitary thought or fancy; but "Idea," nearer Plato's idea of ἰδέα, denotes anything whose Being consists in its mere capacity for getting fully represented, regardless of any person's faculty or impotence to represent it. "Real" is a word invented in the thirteenth century to signify having Properties, i.e. characters sufficing to identify their subject, and possessing these whether they be anywise attributed to it by any single man or group of men, or not. Thus, the substance of a dream is not Real, since it was such as it was, merely in that a dreamer so dreamed it; but the fact of the dream is Real, if it was dreamed; since if so, its date, the name of the dreamer, etc., make up a set of circumstances sufficient to distinguish it from all other events; and these belong to it, i.e. would be true if predicated of it, whether A, B, or C Actually ascertains them or not.