Cameroon Rapid Response Displacement & Cholera 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Africanprogramme for Onchocerctasts Control (Apoc)
RESERVED FOR PROTECT LOGO/HEADING COUNTRYAIOTF: CAMEROON Proiect Name: CDTI SW 2 Approval vearz 1999 Launchins vegr: 2000 Renortins Period: From: JANUARY 2008 To: DECEMBER 2008 (Month/Year) ( Mont!{eq) Proiectvearofthisrenort: (circleone) I 2 3 4 5 6 7(8) 9 l0 Date submitted: NGDO qartner: "l"""uivFzoog Sightsavers International South West 2 CDTI Project Report 2008 - Year 8. ANNUAL PROJECT TECHNICAL REPORT SUBMITTED TO TECHNICAL CONSULTATTVE COMMITTEE (TCC) DEADLINE FOR SUBMISSION: To APOC Management by 3l January for March TCC meeting To APOC Management by 31 Julv for September TCC meeting AFRICANPROGRAMME FOR ONCHOCERCTASTS CONTROL (APOC) I I RECU LE I S F[,;, ?ur], APOC iDIR ANNUAL I'II().I Ii(]'I"IIICHNICAL REPORT 't'o TECHNICAL CONSU l.',l'A]'tvE CoMMITTEE (TCC) ENDORSEMENT Please confirm you have read this report by signing in the appropriat space. OFFICERS to sign the rePort: Country: CAMEROON National Coordinator Name: Dr. Ntep Marcelline S l) u b Date: . ..?:.+/ c Ail 9ou R Regional Delegate Name: Dr. Chu + C( z z a tu Signature: n rJ ( Date 6t @ RY oF I DE LA NGDO Representative Name: Dr. Oye Joseph E Signature: .... Date:' g 2 JAN. u0g Regional Oncho Coordinator Name: Mr. Ebongo Signature: Date: 51-.12-Z This report has been prepared by Name : Mr. Ebongo Peter Designation:.OPC SWII Signature: *1.- ,l 1l Table of contents Acronyms .v Definitions vi FOLLOW UP ON TCC RECOMMENDATIONS. 7 Executive Summary.. 8 SECTION I : Background information......... 9 1.1. GrrueRruINFoRMATroN.................... 9 1.1.1 Description of the project...... 9 Location..... 9 1. 1. 2. -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -
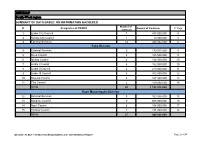
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Limbe City Council 7 475 000 000 4 2 Kumba City Council 1 10 000 000 5 3 External Services 14 440 032 000 6 Fako Division 4 External Services 9 179 015 000 8 5 Buea Council 5 125 500 000 9 6 Idenau Council 4 124 000 000 10 7 Limbe I Council 4 152 000 000 10 8 Limbe II Council 4 219 000 000 11 9 Limbe III Council 6 102 500 000 12 10 Muyuka Council 6 127 000 000 13 11 Tiko Council 5 159 000 000 14 TOTAL 43 1 188 015 000 Kupe Muanenguba Division 12 External Services 5 100 036 000 15 13 Bangem Council 9 605 000 000 15 14 Nguti Council 6 104 000 000 17 15 Tombel Council 7 131 000 000 18 TOTAL 27 940 036 000 MINMAP / PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION Page 1 of 34 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Lebialem Division 16 External Services 5 134 567 000 19 17 Alou Council 9 144 000 000 19 18 Menji Council 3 181 000 000 20 19 Wabane Council 9 168 611 000 21 TOTAL 26 628 178 000 Manyu Division 18 External Services 5 98 141 000 22 19 Akwaya Council 6 119 500 000 22 20 Eyomojock Council 6 119 000 000 23 21 Mamfe Council 5 232 000 000 24 22 Tinto Council 6 108 000 000 25 TOTAL 28 676 641 000 Meme Division 22 External Services 5 85 600 000 26 23 Mbonge Council 7 149 000 000 26 24 Konye Council 1 27 000 000 27 25 Kumba I Council 3 65 000 000 27 26 Kumba II Council 5 83 000 000 28 27 Kumba III Council 3 84 000 000 28 TOTAL 24 493 600 000 MINMAP / PUBLIC CONTRACTS -
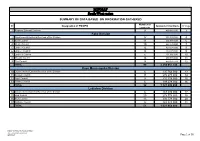
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Regional External Services 9 490 982 000 3 Fako Division 2 Départemental External Services of the Division 17 352 391 000 4 3 Buea Council 11 204 778 000 6 4 Idenau Council 10 224 778 000 7 5 Limbe I Council 12 303 778 000 8 6 Limbe II Council 13 299 279 000 9 7 Limbe III Council 6 151 900 000 10 8 Muyuka Council 16 250 778 000 11 9 Tiko Council 14 450 375 748 12 TOTAL 99 2 238 057 748 Kupe Muanenguba Division 10 Départemental External Services of the Division 6 135 764 000 13 11 Bangem Council 11 572 278 000 14 12 Nguti Council 9 215 278 000 15 13 Tombel Council 6 198 278 000 16 TOTAL 32 1 121 598 000 Lebialem Division 14 Départemental External Services of the Division 6 167 474 000 17 15 Alou Council 20 278 778 000 18 16 Menji Council 13 306 778 000 20 17 Wabane Council 12 268 928 000 21 TOTAL 51 1 021 958 000 PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION /MINMAP Page 1 of 36 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts Manyu Division 18 Départemental External Services of the Division 9 240 324 000 22 19 Akwaya Council 10 260 278 000 23 20 Eyumojock Council 6 195 778 000 24 21 Mamfe Council 7 271 103 000 24 22 Tinto Council 7 219 778 000 25 TOTAL 39 1 187 261 000 Meme Division 23 Départemental External Services of the Division 4 82 000 000 26 24 Konye Council 5 171 533 000 26 25 Kumba -

Cameroon:NW/SW Highlights Needs 690K 414K 679K1 52 $9.5M
Cameroon:NW/SW WASH Update Hand-washing sensitization in Bamenda II. Photo by WA Cameroon. September 2020 Highlights Needs In August, more than 28,800 people were reached with various WASH services 690k People in need of WASH conducted by eight WASH partners services in NW/SW namely ASWEDO, CHAMEG, EPDA, GCR, H4BF, IRC, NRC and SUDAHSER. 414k Targeted WASH partners reached 7,000 people through hygiene promotion sessions while 679k1 IDPs over 9,200 individuals were reached through COVID-19 sensitization activities. 52 WASH partners In September, more than 330 households in Bamenda 1, 2, 3 and Limbe 1 sub- $9.5m divisions benefited from distribution of WASH kits by NRC and SUDAHSER required for WASH $9.5m EPDA, in collaboration with UNICEF, constructed 42 emergency latrines that are expected to benefit at least 8,300 people in Fako and Ndian sub-divisions. $0.2M Required Funded 1 Cameroon: OCHA NW/SW Situation Report No.22, 2020 Website: https://www.humanitarianresponse.info/en/operations/cameroon/water-sanitation-hygiene For more information contact Wash Cluster Coordinator: Nchunguye Festo Vyagusa Email: [email protected] Information Management Officer: Stan Mverechena, Email [email protected] WATER In Bui (North West) and Ndian (South West), SUDAHSER formed and trained four water user committees whose responsibility is to ensure that water, sanitation and hygiene standards are maintained. CHAMEG conducted a training that was attended by 36 water user committee members in Buea, Fako division. In Wovia village, Limbe II sub-division of South West region, EPDA constructed a safe spring water catchment that will benefit at least 500 people. -

Programming of Public Contracts Awards and Execution for the 2020
PROGRAMMING OF PUBLIC CONTRACTS AWARDS AND EXECUTION FOR THE 2020 FINANCIAL YEAR CONTRACTS PROGRAMMING LOGBOOK OF DEVOLVED SERVICES AND OF REGIONAL AND LOCAL AUTHORITIES SOUTH-WEST REGION 2021 FINANCIAL YEAR SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Regional External Services 6 219 193 000 3 2 Kumba City Council 1 100 000 000 4 Fako Division 3 Divisional External Services 6 261 261 000 5 4 Buea Council 10 215 928 000 5 5 Idenau Council 10 360 000 000 6 6 Limbe I Council 12 329 000 000 7 7 Limbe II Council 9 225 499 192 8 8 Limbe III Council 13 300 180 000 9 9 Muyuka Council 10 303 131 384 10 10 Tiko Council 8 297 100 000 11 TOTAL 78 2 292 099 576 Kupe Manenguba Division 11 Divisional External Services 2 47 500 000 12 12 Bangem Council 9 267 710 000 12 13 Nguti Council 8 224 000 000 13 14 Tombel Council 10 328 050 000 13 TOTAL 29 867 260 000 Lebialem Division 15 Divisional External Services 1 32 000 000 15 16 Alou Council 13 253 000 000 15 17 Menji Council 4 235 000 000 16 18 Wabane Council 10 331 710 000 17 TOTAL 28 851 710 000 Manyu Division 19 Divisional External Services 1 22 000 000 18 20 Akwaya Council 7 339 760 000 18 21 Eyumojock Council 8 228 000 000 18 22 Mamfe Council 10 230 000 000 19 23 Tinto Council 9 301 760 000 20 TOTAL 35 1 121 520 000 MINMAP/Public Contracts Programming and Monitoring Division Page 1 of 30 SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts Meme Division 24 -

Cameroon - South-West Region ! H Administrative Breakdowns NIGER
Cameroon - South-West Region ! h Administrative Breakdowns NIGER CHAD N N " NIGERIA " 0 0 ' !Mfom ' 0 0 3 3 ° ° 6 ! Iyahe 6 !Akumaye !Ngale !Wum CAMEROON CAR !Nkim EQUATORIAL GUINEA GABON CONGO NIGERIA NORTH-WEST AKWAYA !Bafut N N " " 0 0 ' ' 0 !Acha Tugui 0 ° ° 6 6 !Ikom !Bamenda !Bali Baliben MANYU ! ! Mamfe Ayukaba ! Bachuo Akagbe ! WABANE EYUMODJOCK UPPER BAYANG LEBIALEM !Mbouda MAMFE ALOU N N " Bamougo!um " 0 0 ' ' 0 0 3 3 ° ° 5 5 ! Dschang FONTEM ! WEST ! Old Dunlop Town ! !Oban Company NGUTI ! KUPE-MANENGUBA TOKO !Kekem !Bafang !Melong SOUTH-WEST BANGEM !Passim N N " " 0 0 ' ' 0 0 ° ° 5 Calabar MUNDEMBA 5 ! !Nkongsamba !Ikot Offiong KONYE NDIAN TOMBEL !Manjo !Oron ! ISANGELE Tombel DIKOME BALUE ! Loum CAMEROON KUMBA ! KOMBO ITINDI EKONDO TITI 2ND Penja !Kumba ! KOMBO MEME !Ekondo Titi ABEDIMO KUMBA 3RD KUMBA 1ST N N " " 0 0 ' !Mbanga CENTRE ' 0 Longtoka 0 3 IDABATO ! 3 ° ° 4 BAMUSSO 4 !Ndokbélé !Mweli LITTORAL MBONGE MBONGE MUYUKA !Muyuka !Kaké !\ National capital FAKO !! Major Town WEST-COAST Bomono Gare ! BUEA ! Intermediate Town ! !Bonépoupa II ! Bomono Ba Buea ! Mbengué Small Town Mutengene ! TIKO ! International boundary Tiko Douala LIMBE !! LIMBE 2ND ! N N " 1ST Region boundary " 0 0 ' Limbe ' 0 0 ° ° 4 LIMBE 3RD 4 Department boundary Commune boundary ± River 0 10 20 E40QUATORIAL Surface Waterbody Kilometres !Edéa 8°30'0"E GUINEA 9°0'0"E 9°30'0"E 10°0'0"E Date Created: 20 Dec 2018 - Contact: [email protected] Data sources: Boundaries: OCHA, The designations employed and the presentation of material in the map(s) do not imply the expression of any opinion on the part of WFP concerning Website: www.logcluster.org - Prepared by: HQ, OSE GIS ©OpenStreetMap Contributors © World Food Programme 2018 the legal or constitutional status of any country, territory, city or sea, or Map Reference: CMR_ADMIN_SudOuest_A3P_20181128 Populated places: GeoNames concerning the delimitation of its frontiers or boundaries.. -

Proceedingsnord of the GENERAL CONFERENCE of LOCAL COUNCILS
REPUBLIC OF CAMEROON REPUBLIQUE DU CAMEROUN Peace - Work - Fatherland Paix - Travail - Patrie ------------------------- ------------------------- MINISTRY OF DECENTRALIZATION MINISTERE DE LA DECENTRALISATION AND LOCAL DEVELOPMENT ET DU DEVELOPPEMENT LOCAL Extrême PROCEEDINGSNord OF THE GENERAL CONFERENCE OF LOCAL COUNCILS Nord Theme: Deepening Decentralization: A New Face for Local Councils in Cameroon Adamaoua Nord-Ouest Yaounde Conference Centre, 6 and 7 February 2019 Sud- Ouest Ouest Centre Littoral Est Sud Published in July 2019 For any information on the General Conference on Local Councils - 2019 edition - or to obtain copies of this publication, please contact: Ministry of Decentralization and Local Development (MINDDEVEL) Website: www.minddevel.gov.cm Facebook: Ministère-de-la-Décentralisation-et-du-Développement-Local Twitter: @minddevelcamer.1 Reviewed by: MINDDEVEL/PRADEC-GIZ These proceedings have been published with the assistance of the German Federal Ministry for Economic Cooperation and Development (BMZ) through the Deutsche Gesellschaft für internationale Zusammenarbeit (GIZ) GmbH in the framework of the Support programme for municipal development (PROMUD). GIZ does not necessarily share the opinions expressed in this publication. The Ministry of Decentralisation and Local Development (MINDDEVEL) is fully responsible for this content. Contents Contents Foreword ..............................................................................................................................................................................5 -
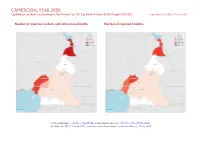
CAMEROON, YEAR 2020: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 23 March 2021
CAMEROON, YEAR 2020: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 23 March 2021 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, 6 May 2018b; administrative divisions: GADM, 6 May 2018a; incid- ent data: ACLED, 12 March 2021; coastlines and inland waters: Smith and Wessel, 1 May 2015 CAMEROON, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 23 MARCH 2021 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Violence against civilians 572 313 669 Conflict incidents by category 2 Battles 386 198 818 Development of conflict incidents from 2012 to 2020 2 Strategic developments 204 1 1 Protests 131 2 2 Methodology 3 Riots 63 28 38 Conflict incidents per province 4 Explosions / Remote 43 14 62 violence Localization of conflict incidents 4 Total 1399 556 1590 Disclaimer 5 This table is based on data from ACLED (datasets used: ACLED, 12 March 2021). Development of conflict incidents from 2012 to 2020 This graph is based on data from ACLED (datasets used: ACLED, 12 March 2021). 2 CAMEROON, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 23 MARCH 2021 Methodology on what level of detail is reported. Thus, towns may represent the wider region in which an incident occured, or the provincial capital may be used if only the province The data used in this report was collected by the Armed Conflict Location & Event is known. -

Cartography of the War in Southern Cameroons Ambazonia
Failed Decolonization of Africa and the Rise of New States: Cartography of the War in Southern Cameroons Ambazonia Roland Ngwatung Afungang* pp. 53-75 Introduction From the 1870s to the 1900s, many European countries invaded Africa and colonized almost the entire continent except Liberia and Ethiopia. African kingdoms at the time fought deadly battles with the imperialists but failed to stop them. The invaders went on and occupied Africa, an occupation that lasted up to the 1980s. After World War II, the United Nations (UN) resolution 1514 of 14 December 1960 (UN Resolution 1415 (1960), accessed on 13 Feb. 2019) obliged the colonial powers to grant independence to colonized peoples and between 1957 and 1970, over 90 percent of African countries got independence. However, decolonization was not complete as some colonial powers refused to adhere to all the provisions of the above UN resolution. For example, the Portuguese refused to grant independence to its African colonies (e.g. Angola and Mozambique). The French on their part granted conditional independence to their colonies by maintaining significant ties and control through the France-Afrique accord (an agreement signed between France and its colonies in Africa). The France-Afrique accord led to the creation of the Franc CFA, a currency produced and managed by the French treasury and used by fourteen African countries (African Business, 2012). CFA is the acronym for “Communauté Financière Africaine” which in English stands for “African Financial Community”. Other colonial powers violated the resolution by granting independence to their colonies under a merger agreement. This was the case of former British Southern Cameroons and Republic of Cameroon, South Sudan and Republic of Sudan, Eritrea and Ethiopia, Senegal and Gambia (Senegambia Confederation, 1982-1989). -

MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Regional External Services 9 329 101 000 3 Fako Division 2 Départemental External Services of the Division 10 184 301 000 4 3 Buea Council 9 148 093 000 5 4 Idenau Council 9 248 200 000 6 5 Limbe I Council 8 149 350 000 7 6 Limbe II Council 13 326 200 000 8 7 Limbe III Council 18 369 350 000 10 8 Muyuka Council 9 196 947 000 12 9 Tiko Council 12 381 200 000 13 TOTAL 88 2 003 641 000 Kupe Muanenguba Division 10 Départemental External Services of the Division 2 55 000 000 15 11 Bangem Council 10 253 700 000 15 12 Nguti Council 8 266 700 000 16 13 Tombel Council 8 395 000 000 17 TOTAL 28 970 400 000 Lebialem Division 14 Départemental External Services of the Division 2 37 000 000 19 15 Alou Council 8 277 700 000 19 16 Menji Council 5 147 700 000 20 17 Wabane Council 9 273 000 000 21 TOTAL 24 735 400 000 Manyu Division 18 Départemental External Services of the Division 2 39 500 000 23 19 Akwaya Council 11 293 842 000 23 20 Eyumojock Council 5 180 700 000 24 21 Mamfe Council 10 571 832 532 25 22 Tinto Council 11 254 769 714 26 TOTAL 39 1 340 644 246 MINMAP/Public Contracts Programming and Monitoring Division Page 1 of 42 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts Meme Division 23 Départemental External Services of the Division 5 182 000 000 28 24 Kumba I Council 6 115 134 500 28 25 Kumba II Council -

Idabato Council Development Plan
REPUBLIQUE DU CAMEROUN REPUBLIC OF CAMEROON ------------ --------- Paix – Travail – Patrie Peace – Work – Fatherland ----------- ---------- MINISTERE DE L’ECONOMIE, DE LA PLANIFICATION MINISTRY OF ECONOMY, PLANNING AND ET DE L’AMENAGEMENT DU TERRITOIRE REGIONAL DEVELOPMENT ------------- ---------- SECRETARIAT GENERAL SECRETARY GENERAL ------------ ---------- PROGRAMME NATIONAL DE DEVELOPPEMENT NATIONAL COMMUNITY DRIVEN DEVELOPMENT PARTICIPATIF PROGRAM ------------ ---------- CELLULE REGIONALE DE COORDINATION DE SUD SOUTH WEST REGIONAL COORDINATION UNIT OUEST Tel: 33322735 Fax: 33322759 Tel: 33322735 Fax: 33322759 Email: [email protected] Email: [email protected] IDABATO COUNCIL DEVELOPMENT PLAN DECEMBER 2011 EXECUTIVE SUMMARY A Development Plan for the Idabato Council was developed for the period of August 2011 to January 2012, through a Local Support Organisation (LSO), Reach Out Cameroon facilitated by the National Community-driven Development Program (PNDP). The Plan covered a wide range of development concerns of the municipality such as Health, Water schemes, Electricity, Road networks, Environment and Nature Protection, Women Empowerment and the Family and Livestock-Fishery. The municipality is located around latitude 40 30’ 14.4” (4.5040) North and longitude 80 32’ 44.2” (8.54560) East with an average elevation of approximately 64m (210 feet). The council became operational in February 1996 with Idabato II as the head quarters. The municipality comprises of some 18 villages mostly fishing ports populated by native communities of Nigerian origin. Kombo A’Munja and Jabane are the other biggest towns closest to Idabato. The following process/methodology were used for the elaboration of the Idabato Communal Development Plan (CDP): Village Diagnosis, Urban Space Diagnosis, Council Institutional Diagnosis, Strategic Planning, Programming and Resource Mobilisation. After the collection and analysis of data at each level of the process, the data was restituted to the population.