Simplifying Respiratory Drug Regimen Presentation Handouts.Pptx
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Medicaid Policy Change
MEDICAID POLICY CHANGE IMMINENT PERIL JUSTIFICATION September 25, 2019 ADVAIR: POLICY CHANGE: LDH is changing the preferred drug list to switch the diskus inhaled powder from preferred to non-preferred and adding the HFA inhaler to the preferred list instead. JUSTIFICATION: This product is used to control symptoms and prevent complications caused by asthma or chronic obstructive pulmonary disease. This change is necessary to make an easier delivery device available for recipients to aid with treatment. Without preferred status, recipients would be required to obtain prior authorization which could delay necessary treatment. This change is needed by 10/1/19 due to the coming seasonal change in weather, including influenza and allergy season, that can significantly exacerbate chronic lung diseases, and so this presents an imminent peril to public health. EFFECTIVE DATE: October 1, 2019 LA Medicaid Preferred Drug List (PDL)/Non-Preferred Drug List (NPDL) Effective Date: July 15October 1, 2019 AG – Authorized Generic DR – Concurrent Prescriptions Must Be Written by Same Prescriber PU – Prior Use of Other Medication is Required AL – Age Limits DS – Maximum Days’ Supply Allowed QL – Quantity Limits BH – Behavioral Health Clinical Authorization Required for Children Younger Than 6 DT – Duration of Therapy Limit RX – Specific Prescription Requirements Years Old BY – Diagnosis Codes Bypass Some Requirements DX – Diagnosis Code Requirements TD – Therapeutic Duplication UN – Drug Use Not Warranted (Needs Appropriate CL – More Detailed Clinical Information -

Chronic Obstructive Lung Disease
Chronic Obstructive Lung Disease Amita Vasoya, DO FACOI FCCP FAASM Christiana Care Pulmonary Associates Clinical Assistant Professor of Medicine Sidney Kimmel Medical College of Thomas Jefferson University Rowan University School of Osteopathic Medicine ACOI Board Review 2019 Disclosures No Disclosures Obstructive Lung Diseases COPD Chronic ◦ Chronic Bronchitis Bronchitis Emphysema ◦ Emphysema Asthma Other ◦ Bronchiectasis Asthma ◦ Bronchiolitis ◦ Cystic Fibrosis ◦ Alpha 1 anti-trypsin deficiency Inter-relationship: Inflammation and Bronchial Hyperreactivity ATS GOLD CHEST 2002; 121: 121S-126S COPD THIRD leading cause of death worldwide It is the only leading cause of death whose prevalence is increasing! http://www.who.int/mediacentre/factsheets COPD Risk Factors Cigarette smoking Occupational exposures ◦ Silica, formaldehyde, toluene, nickel, cadmium, cotton, dust, etc Air pollution Biomass fuel Hyperresponsive airway Asthma Genetic factors Pathogenesis of COPD ATS Pulmonary Board Review 2015 Inflammatory Mediators: COPD ATS Pulmonary Board Review 2015 INFLAMMATION Small Airway Disease Parenchyma destruction Airway inflammation Loss of alveolar attachments Airway remodeling Decreased elastic recoil AIRFLOW LIMITATION ATS Pulmonary Board Review 2015 COPD Phenotypes Non-exacerbator Exacerbator with emphysema Exacerbator with chronic bronchitis Frequent exacerbator Alpha 1 Antitrypsin deficiency ACOS BCOS www.eclipse-copd.com, Lange P. Int J COPD 2016. 11: 3-12 Hurst JR. NEJM 2010. 363: 1128-38 Morphologic Types of -

Study Protocol and Statistical Analysis Plan
Propranolol and Gene Expression in HCT Protocol v3.0, January 15, 2016 RANDOMIZED CONTROLLED PILOT STUDY USING PROPRANOLOL TO DECREASE GENE EXPRESSION OF STRESS-MEDIATED BETA- ADRENERGIC PATHWAYS IN HEMATOPOIETIC STEM CELL TRANSPLANT RECIPIENTS Version 3.0 Principal Investigator: Jennifer M. Knight, MD Medical College of Wisconsin 8701 Watertown Plank Road Milwaukee, WI 53226 Telephone: 414-955-8908 Fax: 414-955-6285 Email: [email protected] Co-Investigator: J. Douglas Rizzo, MD, MS CIBMTR Froedtert and the Medical College of Wisconsin Clinical Cancer Center 9200 W. Wisconsin Avenue Suite C5500 Milwaukee, WI 53226 Telephone: 414-805-0700 Fax: 414-805-0714 Email: [email protected] Co-Investigator: Parameswaran Hari, MD, MS Froedtert and the Medical College of Wisconsin Clinical Cancer Center 9200 W. Wisconsin Avenue Suite C5500 Milwaukee, WI 53226 Telephone: 414-805-4600 Fax: 414-805-4606 Email: [email protected] Consultant Steve W. Cole, PhD and Statistician: UCLA-David Geffen School of Medicine 10833 LeConte Ave 11-934 Factor Bldg Los Angeles, CA 90095-1678 Telephone: 310-267-4243 Email: [email protected] 1 Propranolol and Gene Expression in HCT Protocol v3.0, January 15, 2016 Sponsor: Medical College of Wisconsin Funding Sponsor: This project has an offer of sponsorship from the National Cancer Institute, National Institutes of Health, under Contract No. HHSN261200800001E. 2 Propranolol and Gene Expression in HCT Protocol v3.0, January 15, 2016 PROTOCOL SYNOPSIS Randomized Controlled Pilot Study Using Propranolol to Decrease Gene Expression of Stress-Mediated Beta-Adrenergic Pathways in Hematopoietic Stem Cell Transplant Recipients Principal Investigator: Jennifer M. Knight, MD Study Design: This is a randomized controlled pilot study designed to evaluate whether the beta-adrenergic antagonist propranolol is effective in decreasing gene expression of stress-mediated beta-adrenergic pathways among a cohort of individuals receiving an autologous hematopoietic stem cell transplant (HCT) for multiple myeloma. -

Prediction of Premature Termination Codon Suppressing Compounds for Treatment of Duchenne Muscular Dystrophy Using Machine Learning
Prediction of Premature Termination Codon Suppressing Compounds for Treatment of Duchenne Muscular Dystrophy using Machine Learning Kate Wang et al. Supplemental Table S1. Drugs selected by Pharmacophore-based, ML-based and DL- based search in the FDA-approved drugs database Pharmacophore WEKA TF 1-Palmitoyl-2-oleoyl-sn-glycero-3- 5-O-phosphono-alpha-D- (phospho-rac-(1-glycerol)) ribofuranosyl diphosphate Acarbose Amikacin Acetylcarnitine Acetarsol Arbutamine Acetylcholine Adenosine Aldehydo-N-Acetyl-D- Benserazide Acyclovir Glucosamine Bisoprolol Adefovir dipivoxil Alendronic acid Brivudine Alfentanil Alginic acid Cefamandole Alitretinoin alpha-Arbutin Cefdinir Azithromycin Amikacin Cefixime Balsalazide Amiloride Cefonicid Bethanechol Arbutin Ceforanide Bicalutamide Ascorbic acid calcium salt Cefotetan Calcium glubionate Auranofin Ceftibuten Cangrelor Azacitidine Ceftolozane Capecitabine Benserazide Cerivastatin Carbamoylcholine Besifloxacin Chlortetracycline Carisoprodol beta-L-fructofuranose Cilastatin Chlorobutanol Bictegravir Citicoline Cidofovir Bismuth subgallate Cladribine Clodronic acid Bleomycin Clarithromycin Colistimethate Bortezomib Clindamycin Cyclandelate Bromotheophylline Clofarabine Dexpanthenol Calcium threonate Cromoglicic acid Edoxudine Capecitabine Demeclocycline Elbasvir Capreomycin Diaminopropanol tetraacetic acid Erdosteine Carbidopa Diazolidinylurea Ethchlorvynol Carbocisteine Dibekacin Ethinamate Carboplatin Dinoprostone Famotidine Cefotetan Dipyridamole Fidaxomicin Chlormerodrin Doripenem Flavin adenine dinucleotide -

California Essential Drug List
California Essential Drug List The Essential Drug List (formulary) includes a list of drugs covered by Health Net. The drug list is updated at least monthly and is subject to change. All previous versions are no longer in effect. You can view the most current drug list by going to our website at www.healthnet.com. Refer to Evidence of Coverage or Certificate of Insurance for specific cost share information. For California Individual & Family Plans: Drug Lists Select Health Net Large Group – Formulary (pdf). For Small Business Group: Drug Lists Select Health Net Small Business Group – Formulary (pdf). NOTE: To search the drug list online, open the (pdf) document. Hold down the “Control” (Ctrl) and “F” keys. When the search box appears, type the name of your drug and press the “Enter” key. If you have questions or need more information call us toll free. California Individual & Family Plans (off-Exchange) If you have questions about your pharmacy coverage call Customer Service at 1-800-839-2172 California Individual & Family Plans (on-Exchange) If you have questions about your pharmacy coverage call Customer Service at 1-888-926-4988 Hours of Operation 8:00am – 7:00pm Monday through Friday 8:00am – 5:00pm Saturday Small Business Group If you have questions about your pharmacy coverage call Customer Service at 1-800-361-3366 Hours of Operation 8:00am – 6:00pm Monday through Friday Updated September 1, 2021 Health Net of California, Inc. and Health Net Life Insurance Company are subsidiaries of Health Net, LLC and Centene Corporation. Health Net is a registered service mark of Health Net, LLC Table of Contents What If I Have Questions Regarding My Pharmacy Benefit? ................................... -

Therapeutic Class Overview Inhaled Anticholinergics
Therapeutic Class Overview Inhaled Anticholinergics Therapeutic Class Overview/Summary: The inhaled anticholinergics are a class of bronchodilators primarily used in the management of chronic obstructive pulmonary disease (COPD), a condition characterized by progressive airflow restrictions that are not fully reversible.1-3 Symptoms associated with COPD typically include dyspnea, cough, sputum production, wheezing and chest tightness. Specifically, inhaled anticholinergics work via the inhibition of acetylcholine at parasympathetic sites in bronchial smooth muscle causing bronchodilation. Meaningful increases in lung function can be achieved with the use of inhaled anticholinergics in patients with COPD.1-3 The available single-entity inhaled anticholinergics include aclidinium (Tudorza® Pressair), glycopyrrolate (Seebri Neohaler®), ipratropium (Atrovent®, Atrovent® HFA), tiotropium (Spiriva®, Spiriva Respimat®) and umeclidinium (Incruse Ellipta®) with the combination products including glycopyrrolate/indacaterol (Utibron Neohaler®), umeclidinium/vilanterol (Anoro Ellipta®), tiotropium/olodaterol (Stiolto Respimat®) and ipratropium/albuterol, formulated as either an inhaler (Combivent Respimat®) or nebulizer solution (DuoNeb).4-15 Ipratropium, a short-acting bronchodilator, has a duration of action of six to eight hours and requires administration four times daily. Aclidinium, glycopyrrolate, tiotropium and umeclidinium are considered long-acting bronchodilators. Aclidinium is dosed twice daily, while glycopyrrolate, tiotropium and umeclidinium -

BREO • Do Not Use in Combination with an Additional Medicine Containing a ELLIPTA Safely and Effectively
HIGHLIGHTS OF PRESCRIBING INFORMATION treat acute symptoms. (5.2) These highlights do not include all the information needed to use BREO • Do not use in combination with an additional medicine containing a ELLIPTA safely and effectively. See full prescribing information for LABA because of risk of overdose. (5.3) BREO ELLIPTA. • Candida albicans infection of the mouth and pharynx may occur. Monitor patients periodically. Advise the patient to rinse his/her mouth with water BREO ELLIPTA 100/25 (fluticasone furoate 100 mcg and vilanterol without swallowing after inhalation to help reduce the risk. (5.4) 25 mcg inhalation powder), for oral inhalation • Increased risk of pneumonia in patients with COPD. Monitor patients for BREO ELLIPTA 200/25 (fluticasone furoate 200 mcg and vilanterol signs and symptoms of pneumonia. (5.5) 25 mcg inhalation powder), for oral inhalation • Potential worsening of infections (e.g., existing tuberculosis; fungal, Initial U.S. Approval: 2013 bacterial, viral, or parasitic infections; ocular herpes simplex). Use with caution in patients with these infections. More serious or even fatal course WARNING: ASTHMA-RELATED DEATH of chickenpox or measles can occur in susceptible patients. (5.6) See full prescribing information for complete boxed warning. • Risk of impaired adrenal function when transferring from systemic • Long-acting beta2-adrenergic agonists (LABA), such as vilanterol, corticosteroids. Taper patients slowly from systemic corticosteroids if increase the risk of asthma-related death. A placebo-controlled trial transferring to BREO ELLIPTA. (5.7) with another LABA (salmeterol) showed an increase in • Hypercorticism and adrenal suppression may occur with very high asthma-related deaths. This finding with salmeterol is considered a dosages or at the regular dosage in susceptible individuals. -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used -
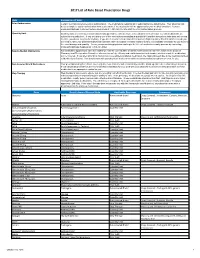
2017 List of Rule Based Prescription Drugs
2017 List of Rule Based Prescription Drugs Rule Explanation of Rule Prior Authorization Certain medications require a prior authorization. The medications requiring prior authorization are listed below. Your physician will need to complete a prior authorization form to determine if the medication will be approved for your medical condition. Contact EnvisionRXOptions Customer Service Help Desk at 1-800-361-4542 to start the Prior Authorization process. Quantity Limit Quantity limits are clinically recommended limits put in place to help ensure safe utilization of medication. Certain medications are subject to a quantity limit. If you are taking one of the medications mandating a quantity limit and the amount you take does not exceed the limit, you do not need to do anything. If you are in need of a medication that requires a higher quantity than that which is listed, you will need to have your prescribing physician submit a letter of medical necessity explaining why it is medically necessary for you to be on the exact dosage and quantity. You or your prescribing physician can begin the letter of medical necessity process by contacting EnvisionRXOptions Helpdesk at 1-800-361-4542. New-to-Market Medications Any medication approved to enter the market will only be covered after a clinical review decision has been made by the Envision Pharmacy and Therapeutics Committee who reviews safety, efficacy and cost information to determine whether or not the medication will be covered. If you attempt to fill or claim a non-covered New-to-Market medication, the claim will reject due to the medications New- to-Market classification. -

Fluticasone Furoate/Vilanterol 92/22 Μg Once-A-Day Vs Beclomethasone Dipropionate/Formoterol 100/6 Μg B.I.D
Open Access Journal of Pulmonology and Respiratory Research Research Article Fluticasone furoate/Vilanterol 92/22 μg once-a-day vs Beclomethasone dipropionate/Formoterol 100/6 μg b.i.d. in asthma patients: a 12-week pilot study Claudio Terzano* and Francesca Oriolo Respiratory Diseases Unit and School of Specialization in Respiratory Diseases Policlinico Umberto I, “Sapienza” University of Rome, Italy *Address for Correspondence: Dr Claudio Abstract Terzano, Respiratory Diseases Unit and School of Specialization in Respiratory Two of the most recent LABA/ICS combinations for treatment of persistent asthma are Fluticasone furoate/ Diseases Policlinico Umberto I, “Sapienza” Vilanterol 92/22 μg (Ellipta) and Beclomethasone dipropionate/Formoterol 100/6 μg (Nexthaler). University of Rome, Italy, Tel: 0649979051; Fax: 06499790675; Email: Objective: To compare once-daily Fluticasone/ Vilanterol combination with twice daily Beclomethasone/ [email protected] Formoterol association in moderate asthma, in terms of quality of life and lung function. Submitted: 08 September 2017 Methods: Fourty patients with moderate asthma treated with Beclomethasone/Formoterol 100/6 μg or Approved: 26 September 2017 Fluticasone/Vilanterol 92/22 μg. We revalued patients in terms of lung function and Asthma Control Test, at 4, 8 Published: 27 September 2017 and 12 weeks to assess any differences between the two groups. After 4 weeks, thirty-one of the fourty patients were evaluated in terms of respiratory function at predetermined time intervals. Copyright: 2017 Terzano C, et al. This is an open access article distributed under the Result: In patients treated with beclomethasone/formoterol FEV1 presented a mean value of 78% at the Creative Commons Attribution License, which third visit and of 79.1% during the fi nal check, compared with 74.5% and to 75.8% in patients in treatment permits unrestricted use, distribution, and with fl uticasone/vilanterol (p 0.01). -

Arformoterol Tartrate) Inhalation Solution 3 15 Mcg*/2 Ml 4 *Potency Expressed As Arformoterol 5 6 for Oral Inhalation Only 7 8 WARNING: ASTHMA RELATED DEATH
® 1 BROVANA 2 (arformoterol tartrate) Inhalation Solution 3 15 mcg*/2 mL 4 *potency expressed as arformoterol 5 6 For oral inhalation only 7 8 WARNING: ASTHMA RELATED DEATH 9 Long-acting beta2-adrenergic agonists (LABA) increase the risk of asthma-related 10 death. Data from a large placebo-controlled US study that compared the safety of 11 another long-acting beta2-adrenergic agonist (salmeterol) or placebo added to usual 12 asthma therapy showed an increase in asthma-related deaths in patients receiving 13 salmeterol. This finding with salmeterol is considered a class effect of LABA, 14 including arformoterol, the active ingredient in BROVANA (see WARNINGS). The 15 safety and efficacy of BROVANA in patients with asthma have not been established. 16 All LABA, including BROVANA, are contraindicated in patients with asthma 17 without use of a long-term asthma control medication (see 18 CONTRAINDICATIONS). 19 20 DESCRIPTION 21 BROVANA (arformoterol tartrate) Inhalation Solution is a sterile, clear, colorless, 22 aqueous solution of the tartrate salt of arformoterol, the (R,R)-enantiomer of formoterol. 23 Arformoterol is a selective beta2-adrenergic bronchodilator. The chemical name for 24 arformoterol tartrate is formamide, N-[2-hydroxy-5-[(1R)-1-hydroxy-2-[[(1R)-2 25 (4-methoxyphenyl)-1-methylethyl]amino]ethyl]phenyl]-, (2R,3R)-2,3 26 dihydroxybutanedioate (1:1 salt), and its established structural formula is as follows: OH H N . HO OH CH3 HO OCH3 HOOC COOH HN H 27 O 28 The molecular weight of arformoterol tartrate is 494.5 g/mol, and its empirical formula ٠C4H6O6 (1:1 salt). -
Medi-Cal Formulary May 2020
Formulary Medi-Cal MAY 2020 The IEHP Medi-Cal Formulary is subject to change throughout the year. All previous versions of the formulary are no longer in effect once a new formulary is available. The IEHP Medi-Cal Formulary can be found at: www.iehp.org/en/members/medical Last Updated: 04/17/2020 Inland Empire Health Plan (IEHP) Medi-Cal Formulary Table of Contents A . Foreword ..................................................................................................................... 2 B. IEHP Member Services .............................................................................................. 2 C. How to Use the Formulary .......................................................................................... 2 D. Prescription Coverage ................................................................................................. 3 D1. Quantity Limits .................................................................................................... 3 D2. Step Therapy ........................................................................................................ 3 E. Filling a Prescription and IEHP’s Pharmacy Network ............................................... 4 F. Definitions ................................................................................................................... 4 G. List of Covered Drugs .............................................................................................. 10 H. Index .......................................................................................................................