Report on JPND Precision Medicine Workshop Amsterdam, March 22Nd 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Genomic Biomarkers in Predictive Medicine. an Interim Analysis
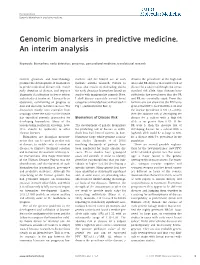
Perspective Genomic biomarkers in predictive medicine Genomic biomarkers in predictive medicine. An interim analysis Keywords: biomarkers; early detection; genomics; personalized medicine; translational research Current genomics and biotechnology markers and the limited use of such denotes the prevalence of the high-risk promise the development of biomarkers markers outside research. Failure to allele and RR denotes the relative risk of to predict individual disease risk, enable focus also results in misleading claims disease for a subject with high-risk versus early detection of disease, and improve for early detection biomarkers based on standard risk allele. Most diseases have diagnostic classification to better inform studies with inappropriate controls. Here, sufficiently low prevalences that the OR individualized treatment. I discuss these I shall discuss separately several broad and RR are essentially equal. From this objectives, commenting on progress to categories of intended use as illustrated in formula one can show that the PPV is no date and obstacles to future success. The Fig 1 (summarized in Box 1). greater than RRÃp. So if the RR is 1.22 and discussion mainly uses examples from the disease prevalence is 5% (p ¼ 0.05), oncology where the nature of the disease then the absolute risk of developing the has expedited genomic approaches for Biomarkers of Disease Risk disease for a subject with a high-risk developing biomarkers. Many of the allele is no greater than 6.1%. If the lessons being learned in oncology, how- The development of genetic biomarkers RR were 5, then the absolute risk of ever, should be applicable to other for predicting risk of disease in indivi- developing disease for a subject with a chronic diseases. -

Xai-EWS — an Explainable AI Model Predicting Acute Critical Illness
Health & Medicine ︱Simon Meyer Lauritsen Patient data Prediction module Output P-Creatinine Acute Kidney Injury: l Kidney eGFR e d o 78% m P-Potassium o t t .. xAI-EWS — an explainable u p n i AI model predicting P-Albumin time Patient data with explanations Explanation module Why? https://www.nature.com/articles/s41467-020-17431-x P-Creatinine n acute critical illness PhotoCredit: Kidney eGFR o i at P-Potassium n a he time it takes medical staff to choices of patients, providers, payers, .. xpl Early clinical predictions of . acute critical illness have a vital diagnose a patient’s acute critical etc. to achieve better outcomes in e influence on patient outcomes. Tillness has a pivotal influence terms of quality of care and its cost. P-Albumin For clinical medicine to benefit on the patient outcome. Acute critical With such high-stake applications, the from the higher predictive illness usually follows a deterioration simpler, more transparent systems are Low parameter value High Low parameter relevance High power of Artificial Intelligence, of the patient’s vital signs – the often chosen so that clinicians can easily however, explainable and routinely measured heart rate, body back-trace a prediction. This strategy, Overview of the xAI-EWS system. Based on patient data, the model makes a prediction, such as a 78% risk of acute kidney injury. The explanation transparent systems are temperature, respiration rate and blood however, can lead to negative outcomes module then explains the predictions in terms of input variables, e.g. p-creatinine, kidney eGFR, p-potassium and p-albumin. -

Inflammation, Cardiovascular Disease and Cancer: Moving Toward Predictive Medicine
Early release, published at www.cmaj.ca on November 28, 2016. Subject to revision. CMAJ Commentary Inflammation, cardiovascular disease and cancer: moving toward predictive medicine Paul M. Ridker MD MPH See also www.cmaj.ca/lookup/doi/10.1503/cmaj.160313 n this issue, Singh-Manoux and colleagues1 ity: AGP, albumin, very-low-density lipoprotein Competing interests: Paul report that measures of low-grade systemic particle size and citrate. However, because con- Ridker is listed as a co-inventor on patents held I inflammation (e.g., C-reactive protein comitant measures of CRP and IL-6 were not by the Brigham and [CRP] and interleukin-6 [IL-6]) in midlife were done in the Estonian and Finnish cohorts, clinical Women’s Hospital that strong independent predictors of all-cause, car- comparisons could not be made. These kind of relate to the use of diovascular and cancer-related mortality in the data are crucial because AGP and albumin both inflammatory biomarkers in cardiovascular disease and Whitehall II study cohort. These findings sup- correlate with systemic low-grade inflammation diabetes that have been port evidence from more than a dozen prior pro- and thus in turn with IL-6 and CRP. licensed to Seimens and spective cohort studies with regard to CRP and In this context, Singh-Manoux and colleagues AstraZeneca. He has 2 received research grants all-cause mortality and more than 50 prior report that all three inflammatory biomarkers from the US National cohort studies showing that CRP and IL-6 pre- were associated with all-cause as well as cardio- Heart, Lung, and Blood dict future myocardial infarction and stroke.3,4 vascular and cancer-related mortality, both in Institute and from Amgen, Novartis, AstraZeneca, Because CRP and IL-6 are strongly correlated univariate analyses and in analyses controlling Pfizer and Kowa. -

Worldquant Initiative for Quantitative Prediction Established at Weill Cornell Medicine
Contact: Jen Gundersen [email protected] 646-962-9497 WorldQuant Initiative for Quantitative Prediction Established at Weill Cornell Medicine Initiative Combines State-of-the-Art Molecular Profiling Technologies with Advanced Financial Algorithms and Computational Methods to Enhance Precision Medicine NEW YORK (April 28, 2017) – Weill Cornell Medicine today announced a gift made by WorldQuant, LLC (“WorldQuant”) and Igor Tulchinsky that will further realize the promise of precision medicine. The $5 million gift establishes a new initiative that will use predictive tools to enhance Weill Cornell Medicine’s capability to diagnose and treat a variety of illnesses, with the goal of improving outcomes for patients. The WorldQuant Initiative for Quantitative Prediction brings together financial and medical experts whose collaboration strives to enhance biomedical research. Weill Cornell Medicine’s scientists, working closely with researchers and technologists from WorldQuant, will deploy predictive tools and quantitative methods to deepen the understanding of genetic factors that drive disease in individual patients. Using sophisticated algorithms, the new initiative will enable the research team to analyze genomic data to identify patterns and trends that may predict patients’ future risk of developing disease, as well as potential outcomes. These insights may be used to improve the diagnosis and treatment of a variety of illnesses, including cancer, neurological disorders, cardiovascular diseases and infections. Weill Cornell Medicine researchers Dr. Christopher Mason, the WorldQuant Research Scholar, and Dr. Olivier Elemento, the Walter B. Wriston Research Scholar, will lead the initiative, which will involve joint work with physician-scientists at the Caryl and Israel Englander Institute for Precision Medicine and the Sandra and Edward Meyer Cancer Center at Weill Cornell Medicine. -

Evolution of Predictive Medicine Vladislav S.BARANOV Otts Institute of Obstetrics, Gynecology & Reproductology, Saint Petersburg, Russia
Journal of Pharmaceutical Sciences and Drug Development Abstract Evolution of Predictive Medicine Vladislav S.BARANOV Otts Institute of obstetrics, Gynecology & Reproductology, Saint Petersburg, Russia Abstract: Achievement s in deciphering of human genome , identification of many thousands of genes responsible for genetic disorders expanded a lot of our knowledge in monogenic, olygogenic & multifactor diseases thus launching the era of “predictive medicine (PM) also to 3 PM ( predictive, preventive , personified ) ( Baranov et al 2000, Baranov,Baranova, 2018) and somewhat later in 2008 after inclusion of “participatory ’by ptof. L. of Russian academy of Sci. Chief Collaborator Depart- Hood–into 4PM . Further progressive development of ment of Genomic Medicine, Ott’s Institute of Obstetric, 4PM was in line with spectacular achievements in mo- Gynecology, Reproductology. Interested in genetic and lecular genome studies . Sophisticated identification of cytogenetic aspects of early development, gene testing of “predisposition” genes by means of whole genome testing inherited predisposition to common disorders, personal- ( GWAS , NGS) o f huge healthy and affected patient ized predictive medicine, gene therapy, The author and cohorts enriched with system genetic approach and rele- co-author of 29 books and over 400 scientific papers St vant omics technologies significantly increased the prac- Petersburg. tical value of PM thus gradually converting it into trans- Publication of speakers: lation medicine(2010) which later ( 2015) gave a birth 1. Epigenetic landscape of endometriosis to “precision, individual molecular medicine” . Since the origin of PM its “sine qua non “ (dry extract) has been 2. The evolution of ideas on the biological role of represented by so called Personal Genetic Pass (GP)-the 5-methylcytosine oxidative derivatives in the mamma- individual DNA data bank incorporating personal lian genome genetic information amenable for direct practical appli- 3. -

Inflammation, Cardiovascular Disease and Cancer: Moving Toward Predictive Medicine
COMMENTARY Inflammation, cardiovascular disease and cancer: moving toward predictive medicine Paul M. Ridker MD MPH n Cite as: CMAJ 2017 March 13;189:E382-3. doi: 10.1503/cmaj.161033 See related article at www.cmaj.ca/lookup/doi/10.1503/cmaj.160313 n this issue, Singh-Manoux and colleagues1 report that mea- sures of low-grade systemic inflammation (e.g., C-reactive KEY POINTS protein [CRP] and interleukin-6 [IL-6]) in midlife were strong • Metabolomic and proteomic studies are furthering the Iindependent predictors of all-cause, cardiovascular and cancer- understanding of “predictive medicine.” related mortality in the Whitehall II study cohort. These findings • Inflammation is a biologic determinant of both cardiovascular support evidence from more than a dozen prior prospective disease and cancer and can be identified by measuring high- cohort studies with regard to CRP and all-cause mortality2 and sensitivity C-reactive protein or interleukin-6. more than 50 prior cohort studies showing that CRP and IL-6 pre- • Ongoing clinical trials will determine whether reducing dict future myocardial infarction and stroke.3,4 Because CRP and inflammation reduces vascular event rates; if so, the clinical IL-6 are strongly correlated (both reflect upstream activation community will need to modify current concepts of residual risk to encompass residual cholesterol risk as well as the emerging from interleukin-1),5 there is no clinical need to measure both concept of residual inflammatory risk. factors, and of the two, CRP measured with a high-sensitivity assay (hs-CRP) is less expensive and has regulatory approval for clinical use. -
Big Data in Healthcare
HEALTHCARE DATA INSTITUTE INTERNATIONAL THINK TANK DEDICATED TO BIG DATA IN HEALTHCARE BIG DATA AND PREVENTION FROM PREDICTION TO DEMONSTRATION NOVEMBER 2016 1 BIG DATA AND PREVENTION FROM PREDICTION TO DEMONSTRATION Acknowledgements to the authors of this White Paper: • Isabelle Barbier-Feraud, Pagamon • Jeanne Bossi Malafosse, Lawyer • Patrice Bouexel, TeraData • Catherine Commaille-Chapus, Open Health Company • Anne Gimalac, Aston Life Sciences • Guillaume Jeannerod, Epiconcept • Magali Léo, CISS • Bruno Leroy, Sanof • Bernard Nordlinger, AP-HP, Académie de Médecine • Michel Paoli, InterMutuelles Assistance • Pablo Prados, Sanof • Jean-Yves Robin, Open Health Company 2 INTRODUCTION aking action to prevent epidemics, identifying risk factors as soon as possible in order to avoid diseases or slow their development, predicting predisposition to particular infec- Ttions from birth, and so on. These are among the goals stated time and time again by scientists and representatives of the medical community. Up to now, the response to these issues has involved the use of tradi- tional research methods, which have been and are still largely based on the notion of reproducibility: using a hypothesis that serves as the basis for the collection of data, an observation makes it possible to develop a relationship among those data and to deduce new hy- potheses or new treatments, which will then be reproduced in similar cases. For a number of years, this research has been enhanced by other very diverse sources that also take into consideration the environ- ment in which the individuals are living: environmental data, so- cio-professional data, etc. This situation is now being re-examined by the sudden emergence of new data management techniques, which must adapt to the massive, exponential production of data characterised by the phenomenon of Big Data (we will come back to a defnition of this term a bit later). -

(P5) Medicine in Rotator Cuff Tears
Journal of Personalized Medicine Perspective Personalized, Predictive, Participatory, Precision, and Preventive (P5) Medicine in Rotator Cuff Tears Umile Giuseppe Longo 1,* , Arianna Carnevale 1,2 , Carlo Massaroni 2 , Daniela Lo Presti 2 , Alessandra Berton 1 , Vincenzo Candela 1, Emiliano Schena 2 and Vincenzo Denaro 1 1 Department of Orthopaedic and Trauma Surgery, Campus Bio-Medico University, Via Álvaro del Portillo, 00128 Rome, Italy; [email protected] (A.C.); [email protected] (A.B.); [email protected] (V.C.); [email protected] (V.D.) 2 Unit of Measurements and Biomedical Instrumentation, Campus Bio-Medico University, Via Álvaro del Portillo, 00128 Rome, Italy; [email protected] (C.M.); [email protected] (D.L.P.); [email protected] (E.S.) * Correspondence: [email protected] Abstract: Rotator cuff (RC) disease is a common musculoskeletal disorder of the shoulder entailing pain, with reduced functionality and quality of life. The main objective of this study was to present a perspective of the current scientific evidence about personalized, predictive, participatory, precision, and preventive approaches in the management of RC diseases. The personalized, predictive, partici- patory, precision and preventive (P5) medicine model is an interdisciplinary and multidisciplinary approach that will provide researchers and clinicians with a comprehensive patrimony of knowledge in the management of RC diseases. The ability to define genetic predispositions in conjunction with the evaluation of lifestyle and environmental factors may boost the tailoring of diagnosis and therapy Citation: Longo, U.G.; Carnevale, A.; in patients suffering from RC diseases. Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Schena, E.; Denaro, V. -

How Can We Move Clinical Genomics Beyond the Hype?
How Can We Move Clinical Genomics Beyond the Hype? Timely Analysis of Immediate Health Policy Issues October 2011 Michael L. Millenson “All of the fruits of the tremendous explosion in innovation that’s been occurring in biomedical research – which make the molecular metamorphosis possible – fulfill their purpose only when they are translated into interventions and solutions that are applied to patients.” —Dr. Andrew von Eschenbach, U.S. Food and Drug Administration Commissioner, 2006 Introduction or no value to be marketed to challenges beyond the direct doctor- providers and patients. The result of patient interaction. Health More than a decade after the this policy vacuum is a disturbing information technology systems successful mapping of the human paradox. Genomics as a field is typically possess neither the ability to genome, clinical genomics1 is beginning to demonstrate its present genomic information in a starting to permeate important parts profound potential to improve health structured way clinicians can use nor of patient care and propel ripples and health care. At the same time, the the large data storage capabilities throughout the entire U.S. health care evidence suggests that the current use such information demands. system. of clinical genomics tests and Comparative effectiveness research therapies often contributes to needs to focus on identifiable Although the field has fallen far short wasteful spending and even patient subpopulations where clinical of the transformational therapeutic harm. genomics interventions can have the impact once widely predicted, most powerful impact, but the particularly in regard to common A 2008 article in Health Affairs concept of “identifiable” can raise diseases, specific interventions have warned that the low threshold for awkward questions about race and crossed the divide between rarity and allowing “unsubstantiated [genomic] ethnicity. -

Omics-Based Medicine and Systems Pathology a New Perspective for Personalized and Predictive Medicine
H. Tanaka: Omics-based Medicine and Systems Pathology. A New Perspective for Personalized and Predictive Medicine, en 11 en11 Omics-based Medicine and Systems Pathology A New Perspective for Personalized and Predictive Medicine H. Tanaka1 1Graduate School of Biomedical Science, Tokyo Medical and Dental University, Tokyo, Japan Summary Conclusion: Omics-based medicine and Objectives systems pathology will realize a new Recent important advances in the human personalized and predictive medicine. genomics and post-genomic “omics” are now bringing about a new medical care Keywords which we call “omics-based medicine”. In Genomics, pharmacogenomics, systems this article, we investigated the pathology, Omics-based medicine, omics development and future possibilities of omics-based medicine. DOI 10.3414/ME9307 Methods We divided the development of omics- The full English version can be found in based medicine into three generations in /Methods of Information in Medicine 2010 order to clarify the main clinical goals and 49 2: 173-185/ or characteristics of informatics method of http://www.schattauer.de/de/magazine/ue each generation, together with its future bersicht/zeitschriften-a- possibilities. z/methods/issue/special/manuscript/1275 7/show.html. Results The first generation of omics-based medicine started with “genomic medicine” based on the inborn individual differences of genome. It has opened the study of genetic polymorphism of the diseases and promoted the personalized medication based on the pharmacogenetic /pharmacogenomic difference of the drug response. In the second generation of omics-based medicine, owing to the advances in the high-throughput technology, vast amount of the various post-genomic disease omics data containing comprehensive molecular information of diseased somatic cells has become available. -

Predictive and Precision Medicine with Genomic Data
Clinical Chemistry 66:1 Q&A 33–41 (2020) Predictive and Precision Medicine with Genomic Data 1* Moderator: Linnea M. Baudhuin Downloaded from https://academic.oup.com/clinchem/article-abstract/66/1/33/5688834 by Brigham & Women's Hospital user on 21 January 2020 Experts: Leslie G. Biesecker,2 Wylie Burke,3 Eric D. Green,4 and Robert C. Green5,6,7 Genome and exome analyses have become instrumental in Biesecker). Each of us cur- establishing genetic diagnoses for critically ill newborns and rently has a major leader- in cases of previous diagnostic dilemmas. Genome and ex- ship role: one as the Direc- ome sequencing of presumably healthy individuals is now tor of NHGRI (E.D. gaining traction. The roll-out of genomic medicine to the Green) and one as the cur- generally healthy population offers a new opportunity to rent President of the Amer- provide insights into the current and future healthcare of ican Society of Human individuals and their families. Indeed, numerous projects Genetics (L.G. Biesecker). such as Geisinger’s MyCode Initiative, the National Hu- From these collective van- man Genome Research Institute (NHGRI)’s8 ClinSeq®, tage points, we have a and the various Genomes2People research projects at broad view of genomics Brigham Health and Harvard Medical School are investi- research and the imple- mentation of genomic medicine—a landscape that in- gating the use of genome sequencing for apparently healthy cludes developing technologies, understanding genome individuals. However, there are many scientific and ethical structure and function, identifying disease genes, imple- questions about the benefits, harms, and costs of this ap- menting genomic-based clinical tests, and designing pre- proach. -

Whole Genome Sequencing and Its Applications in Medical Genetics
Quantitative Biology 2016, 4(2): 115–128 DOI 10.1007/s40484-016-0067-0 REVIEW Whole genome sequencing and its applications in medical genetics Jiaxin Wu, Mengmeng Wu, Ting Chen and Rui Jiang* MOE Key Laboratory of Bioinformatics, Bioinformatics Division and Center for Synthetic & Systems Biology, TNLIST; Department of Automation, Tsinghua University, Beijing 100084, China * Correspondence: [email protected] Received October 30, 2015; Revised February 4, 2016; Accepted February 4, 2016 Fundamental improvement was made for genome sequencing since the next-generation sequencing (NGS) came out in the 2000s. The newer technologies make use of the power of massively-parallel short-read DNA sequencing, genome alignment and assembly methods to digitally and rapidly search the genomes on a revolutionary scale, which enable large-scale whole genome sequencing (WGS) accessible and practical for researchers. Nowadays, whole genome sequencing is more and more prevalent in detecting the genetics of diseases, studying causative relations with cancers, making genome-level comparative analysis, reconstruction of human population history, and giving clinical implications and instructions. In this review, we first give a typical pipeline of whole genome sequencing, including the lab template preparation, sequencing, genome assembling and quality control, variants calling and annotations. We compare the difference between whole genome and whole exome sequencing (WES), and explore a wide range of applications of whole genome sequencing for both mendelian diseases and complex diseases in medical genetics. We highlight the impact of whole genome sequencing in cancer studies, regulatory variant analysis, predictive medicine and precision medicine, as well as discuss the challenges of the whole genome sequencing.