Shropshire Mental Health Needs Assessment February 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Besford Gardens, Trinity Street, Belle Vue, Shrewsbury, SY3 7PQ
ESTATE & LETTINGS AGENTS | CHARTERED SURVEYORS HOW TO FIND THIS PROPERTY From the town centre, the development is best approached over the English Bridge and around the gyratory system into Coleham Head. Continue along Belle Vue Road, eventually turning left into Trinity Street. Continue to the top of Trinity Street and Besford Gardens will be found on the right hand side. SERVICES We understand that mains water, electricity, drainage and natural gas are connected. In partnership with Floreat Homes TENURE We are advised that the properties are freehold and this will be confirmed by the vendors' solicitors during pre-contract enquiries LOCAL AUTHORITIES Shropshire Council Frankwell, Shrewsbury Tel 0345 678 9000 2014-05-23 IMPORTANT NOTICE Our particulars have been prepared with care and are checked where possible by the vendor. They are however, intended as a guide. Measurements, areas and distances are approximate. Appliances, plumbing, heating and electrical fittings are noted, but not tested. Legal matters including Rights of Way, Covenants, Easements, Wayleaves and Planning matters have not been verified and you should take advice from your legal representatives and Surveyor. DO YOU HAVE A PROPEPROPERTYRTY TO SELL ??? We will always be pleased to give you a no obligation market assessment of your existing property to help you with your decision to move DO YOU NEED A SURVEYOR ? We are Chartered Surveyors and will be pleased to give advice on Surveys, Homebuyers Reports and other professional matters. Besford Gardens, Trinity Street, Belle Vue, Shrewsbury, SY3 7PQ To view this property please call us on 01743 236800 Ref: T 4971/SL/GA 3 Bedroomed, Semi-detached House Besford Gardens is an attractive development of 11 houses, set in the popular and established conservation area of Belle Vue. -
Application No Address Proposal Applicant 1 15/03623/TPO
Shrewsbury Town Council List of Planning Applications Registered between 5 August - 1 September 2015 A B C D E Application No Address Proposal Applicant 1 1 15/03623/TPO Overdale, 25 To fell or reduce in size 2 Dr Warren Perks Ridgebourne Road, Douglas Fir trees protected Shrewsbury, by The Borough of Shropshire, SY3 9AA Shrewsbury (Ridgebourne Road) Tree Preservation 472 Order 1968. 2 15/03351/CPL 11 Longhirst Gardens, Application for a Lawful Mr E Rees Shrewsbury, Development Certificate for Shropshire, SY3 5PF erection of a single storey 473 rear extension. 3 15/03436/COU First Floor, Cirrus Change of use of first floor Morris & Company Ltd House , Lower only from D1 non residential (Mrs Elizabeth Lowe, Claremont Bank, educational use to D2 health Welsh Bridge, Shrewsbury, and fitness centre. Shrewsbury, Shropshire, 474 Shropshire, SY1 1RT SY3 8LH) 4 15/03464/FUL 9 Vane Road, Single storey extension and Ms J Cox Shrewsbury, alterations. 475 Shropshire, SY3 7HB 5 15/03424/FUL 3 Florence Close, Erection of extension to Mr And Mrs McLeish Shrewsbury, front and rear of property. 476 Shropshire, SY3 5PD 6 15/03401/FUL 83 Woodfield Road, Erection of two storey Mr & Mrs E Balmer Shrewsbury, extension to side/rear Shropshire, SY3 8HU elevations. 477 7 15/03372/FUL 217 New Park Road, Erection of two storey side Mr J Evans &Miss K Shrewsbury, extension. Cowley Shropshire, SY1 2SW 478 8 15/03319/FUL 103 Tilstock Crescent, Erection of first floor side Mr Andrew Rhodes Shrewsbury, extension. Shropshire, SY2 6HQ 479 9 15/03701/TCA Burnside House, Mill To fell 1 x Ash tree within Mr Frank Heaversedge Road, Meole Brace, Meole Brace Conservation Shrewsbury, Area. -

Shrewsbury Night Magazine Final Art.Indd 1 10/06/2015 17:21 Be Savvy in Shrewsbury
EAT MEET DANCE SLEEP DISCOVER SHREWSBURY AFTER HOURS Shrewsbury Night Magazine Final art.indd 1 10/06/2015 17:21 BE SAVVY IN SHREWSBURY • If you work locally make sure you take originalshrewsbury.co.uk your Original Shrewsbury loyalty card out and about with you /originalshrewsbury • Download the infoBeetle app for all the @originalshrews latest offers plus direct links to taxi firms to take you home originalshrewsbury • Follow Original Shrewsbury on The magazine was published by Shrewsbury BID. Images courtesy Facebook and Twitter for the latest of Danny Beath, Rachael Chidlow, updates and competitions John Kenyon, Victoria Macken and Richard Wilkinson. • Visit originalshrewsbury.co.uk for news, E: [email protected] T: 01743 358 625 events and local information W: originalshrewsbury.co.uk Shrewsbury BID • Go online and sign up for regular Windsor House, Windsor Place email newsletters Shrewsbury, SY1 2BY Shrewsbury Night Magazine Final art.indd 2 10/06/2015 17:21 WELCOME FEEL LIKE FILLING A NIGHT OUT? THIS IS YOUR GUIDE TO SHREWSBURY AFTER HOURS. FROM HAPPY HOURS TO THE BEST DEALS ON DINNER, WHERE TO GO FOR THE LATEST CINEMA SCREENINGS PLUS PLACES TO RETREAT TO SLEEP. If you like to listen to new music in very old For those trying to savour the last rays of venues, mix mojitos in cool cocktail lounges or sunshine don’t miss a sail along the River feast with friends until late, then you really will Severn or a seat in a secluded beer garden with be spoilt for choice for original night-time fi nds in a fi ne local beverage. -

Shrewsbury in Bloom Portfolio
2019 Portfolio 2019 MAYOR OF SHREWSBURY Contents Councillor Phil Gillam To plant a garden is to believe in tomorrow. So said the great A Warm Welcome 1 film actress and humanitarian Audrey Hepburn. Shrewsbury in Bloom Committee 2 I rather like that quote as it immediately turns all gardeners Review of the Year 4 - 7 and all lovers of flowers into optimists, philosophers and prophets too; and striving for a better tomorrow is surely Illustrating your Achievements something to which we can all relate. Horticultural Achievement 8 - 12 As Mayor of Shrewsbury, it is my very great pleasure to welcome you to our beautiful, historic and enchanting town. Environmental Responsibility 13 - 19 Of course, it is a real privilege to be able to promote our Community Participation 20 - 25 town’s horticultural excellence as we once again enter into the competition season. Conclusion and Future Developments I’d especially like to take this opportunity to thank the Key Achievements in 2018/19 26 volunteers, business sponsors, community groups and other organisations who work together so brilliantly on these Key Aims and Objectives for 2019/20 27 occasions, and I’d like to pay tribute to the Shrewsbury in Appendices 28-29 Bloom Committee for the way in which they encourage everyone to join together to uphold our traditions of horticultural distinction. The Shrewsbury in Bloom Committee takes its environmental responsibilities seriously, and Welcome to beautiful Shrewsbury! we have therefore printed this Bloom portfolio on 100% recycled paper using eco-friendly ink. The Shrewsbury in Bloom Committee asked members of the public to submit their favourite photos of the town as part of their annual photo competition, with the winning entries featured on the front and back covers of the Portfolio. -

SHREWSBURY TOWN COUNCIL Planning Committee Meeting Held in the Guildhall, Frankwell Quay, Shrewsbury, SY3 8HR at 6.00Pm on Thurs
SHREWSBURY TOWN COUNCIL Planning Committee Meeting held in the Guildhall, Frankwell Quay, Shrewsbury, SY3 8HR At 6.00pm on Thursday 10 March 2020 PRESENT Councillors N Green (Chairman), J Dean, Ms K Halliday, P Moseley (substituting for P Gillam), K Pardy and Mrs B Wall. IN ATTENDANCE Helen Ball (Town Clerk), Hilary Humphries (Communications Officer) and three members of the pubic. APOLOGIES Apologies were received from Councillors P Gillam, P Nutting and K Roberts. 95/19 DECLARATIONS OF INTEREST IN ACCORDANCE WITH THE CODE OF CONDUCT (i) Declarations of Pecuniary Interest There were no pecuniary interests declared. (ii) Declarations of Non-Pecuniary Interest Shropshire • Those twin-hatted members declared a personal interest in any matters Councillors relating to the Town Council’s relationship with Shropshire Council. • Declared a personal interest in application 20/00660/VAR as Shropshire Council is the applicant. Councillors J • As a member of Shropshire Council Northern Planning Committee, they Dean and N reserve the right to take a different view of the same applications Green considered in light of any additional information presented to the Northern Planning Committee. All Councillors • Declared a personal interest in application 20/00743/TCA as the Town Council is the applicant. Councillor K • Declared a personal interest in application 20/00770/FUL as he is a Pardy Governor at the school. 96/19 MINUTES OF THE LAST MEETING The minutes of the Planning Committee meeting held on 20 February 2020 were submitted as circulated and read. RESOLVED: That the minutes of the Planning Committee meeting held on 20 February 2020 be approved and signed as a correct record. -
Revised Air Quality Action Plan
Revised Air Quality Action Plan Executive Summary Shrewsbury and Atcham Borough Council’s Environmental Health Service has produced this Action Plan following the Review and Assessment of Air Quality in its district as part of its duty under the Environment Act 1995. The report follows on from the Stage III Assessment completed in 2000, Stage IV in August 2003, Detailed Assessment in July 2004 and further Detailed Assessment in March 2006. Work has continued following the declaration of 3 Air Quality Management Areas (AQMAs) at Bayston Hill (AQMA 01), Heathgates Island (AQMA 2) and Frankwell/Smithfield Road (AQMA 03). This includes further modelling and monitoring, which has indicated that Nitrogen Dioxide (NO 2) levels in these areas are likely to rise unless action is taken. An Action Plan has therefore been drawn up investigating the various options available to tackle pollution levels, in particular from road traffic. The effects of these options are examined in detail, with the most effective package of measures (the Action Plan) chosen for implementation. An in-depth study of this package takes place within this document, concluding that the Action Plan should result in a reduction in Nitrogen Dioxide levels and will work towards meeting National Air Quality Objective (NAQO) levels. The Council will continue to monitor the levels in all 3 AQMAs and around its district generally as part of its ongoing air quality management duties. The measures in this Action Plan also work towards reducing levels of NO 2 in the enlarged Air Quality Management Area (03A) in the extended town centre, encompassing AQMA 03 Frankwell/Smithfield Road. -
Appendix 15.5
Appendix 15.5 NON DWELLING NOISE SENSITIVE RECEPTORS Public 1. NOISE LEVEL CHANGES AT NON DWELLING NOISE SENSITIVE RECEPTORS Table 1-1 - Noise level changes with embedded mitigation measures only1 Non Dwelling Sensitive Receptor Do Min With Short Do Min With Long 2023 Scheme Term 2023 Scheme Term 2023 2038 Private Chapel, Berwick House, 40.5 49.8 +9.3 40.5 49.9 +9.4 Berwick Road, Upper Berwick, SY4 3HW St Georges Church, St Georges 50.6 49.6 -1.0 43.4 44.1 +0.7 Street, SY3 8QA Cadogan Gardens Meeting Room, 46.4 45.2 -1.2 48.9 50.2 +1.3 The Mount, SY3 8NU Frankwell Methodist Church, 63.5 62.3 -1.2 63.5 63.0 -0.5 Frankwell, SY3 8LG Christ Church, Welshpool Road, 46.5 50.1 +3.6 46.5 50.7 +4.2 Bicton Heath, SY3 5AH Hope Church, Grafton Mews, SY1 45.5 47.6 +2.1 45.5 48.0 +2.5 3PU Emmanuel Church, Mount Pleasant 42.8 45.2 +2.4 42.8 45.8 +3.0 Road, SY1 3HY The Church Of Jesus Christ Of Latter 64.4 63.4 -1.0 49.0 49.5 +0.5 Day Saints, Mount Pleasant Road, SY1 3HX Greenfields United Church, 51.7 50.4 -1.3 63.9 64.6 +0.7 Greenfield Street, SY1 2PZ Cricket Pavilion, County Recreation 54.1 53.1 -1.0 54.1 53.6 -0.5 Ground, Frankwell, SY3 8RF Darwin Community Centre, 64.2 63.0 -1.2 64.2 63.7 -0.5 Frankwell, SY3 8JY 1 In accordance with the LA111 assessment method, the reported façade is that predicted to experience the greatest magnitude of change, whether that be an increase or decrease in noise level in order to reflect the greatest influence that the impact of introduction of the Proposed Scheme has on the receptor in question. -

Shropshire Local Transport Plan 3 Evidence Base Part 3: Economy and Growth February 2011
Shropshire Local Transport Plan 3 Evidence Base Part 3: Economy and Growth February 2011 1. Shropshire economic portrait1 Business & enterprise Shropshire has a predominantly small business economy, with 87% of businesses employing 10 or fewer staff (compared to 85% nationally and only 2.5% of business having over 50 employees (compared to 3.5% nationally), a higher percentage than any of our statistical (or regional) neighbours. Figure 3.1 Penetration of small businesses. Statistical neighbours 2008. However, there are a few major employers which account for a disproportionately large share of the county workforce. In some smaller market towns in particular, there is heavy reliance on a small number of large employers, which can mean that the choice of employment opportunities is narrow. It also leaves these towns vulnerable should one of the main employers go out of business or relocate. There are high levels of enterprise and entrepreneurship; with higher than average new VAT registrations, and good rates of business survival. Shropshire has high levels of self- employment, 11.8% in Shropshire compared with 9.2% nationally. Many self-employed have home based businesses, Shropshire ranks second in the UK for home-based enterprise. The nature of business enterprise in Shropshire reflects its rural character with agriculture, farm diversification and tourism playing an important part and employing significant numbers of people. Although the structure of the economy has changed significantly over the last two decades, with the emphasis increasingly on service industries rather than agriculture and manufacturing, many of Shropshire’s key sectors today have their origins in the land. -

FOR SALE Mixed Investment Comprising of a Lock up Shop Unit and Three Residential Flats Prominently Located in Frankwell, a Sought After Area of Shrewsbury Price
FOR SALE ATTRACTIVE MIXED INVESTMENT OPPORTUNITY - RETAIL / RESIDENTIAL 124-125 Frankwell, Shrewsbury, Shropshire SY3 8JU Mixed investment comprising of a lock up shop unit and three residential flats Prominently located in Frankwell, a sought after area of Shrewsbury Price: £600,000 (exclusive) hallsgb.com 01743 450 700 FOR SALE MIXED INVESTMENT - SHOP & RESIDENTIAL 124-125 Frankwell, Shrewbury, Shropshire SY3 8JU Location Residential Element The property is prominently located fronting onto Ground Floor Frankwell on the edge of the town centre of Shrewsbury. Shared ground floor entrance from Frankwell into a The property is situated adjacent to the town’s theatre and in a sought after area of the Town. The property is common reception hallway located in area of mixed development close to the River Severn. Flat 1 First Floor Shrewsbury is the County Town of Shropshire and is an Reception Hallway 2232m x 7.751m administrative and tourist centre with a large catchment Bedroom 1 3.0009m x 4.735m population. The property is situated within close proximity of the town’s main car park at Frankwell. The Bathroom New University serving the town of Shrewsbury is Utility Room within close proximity to the property. Kitchen/ sitting Room 5.369m x 6.129m Description Second Floor An attractive prominently located property on the edge Bedroom 2 3.888m x 3.975m of Shrewsbury Town Centre which was comprehensively refurbished approximately 10 years ago. The property (with access onto outside seating area) comprises of a tenanted lock up shop unit with three two bedroomed tenanted flats one benefiting from an Outside integral garage. -

SHROPSHIRE .. [KELLY's Tanswell Arthur, Printer, 5 Bt
442 SB~WSBURY~ SHROPSHIRE .. [KELLY's Tanswell Arthur, printer, 5 Bt. Julian's friars Walker William Bickern, printer, bookseller, bookbinder. Tax Office (John M. Hue, surveyor; N. G. K. Jones, clerk stationer & account book manufacturer, 25 High street. to commissioners), 14 Wyle cop Walker William Henry, fishmonger, 4 Frankwell Taylor William & Co. tobacco pipe works, 52 Coleham Wall John, printer & shopkeeper, 3I St. Michael's street Taylor John; beer retailer, 2I St. Michael's street Wallett Ellen (Miss), private school, 167 Abbey foregate Taylor John, flour depot, 20 St. Michael's street Walter Samuel, grocer, 2oA, Castle foregate Taylor Rowland,shoemaker, 20 Swan hill Waiters John Oscar & Son, maltsters & wine & spirit mer- . TaylorThomas Cope, beer re~iler,33'NewPa.rk rd.Castlefields chants, 7 Glaremont hill. See advertisement Taylor William, accountant, s-Town walls Waiters Clara (Mrs.), greengrocer, Market hall Taylor William, tailor, 6 Claremont hill Waiters Edwin T. auctioneer, see Lythall, Mansell &. Taylor William, shopkeeper, IOI Longden Coleham Waiters, College hill · Taylor William, tailor, I St. Alkmond's square Waiter Frederick R. Brooke, registrar of the Pistrict Probateo Teckoe Snsan (Mrs. ),fish dealer, Gullet passage Court, 30 St. John's hill Teece Henry, grocer, 7 Castle street Walton Henry, bricklayer, IO Benyon street Thatcher Abraham, carpet maker, 5 New street, Frankwell Walton William, shopkeeper, Ditherington Theatre Royal (Mrs. Ann Maddox, proprietress), 18 Shoplatch WardJ"ulia (Mrs.), watch maker, 7 Castle gates Thomas Charles &Co. drapers, 77 Mardol Wardle Wm.& Co.printers & bookbinders,7 & 8 St. John's hill Thomas Alfred, music teacher, 7 St. George's st.Mountfields Warhurst James, music teacher, 42 Abbey foregate Thomas Catherine (Mrs.), temperance hotel, 22 Castle street Warwick George, Greyhound inn, I Chester street Thomas Charles, gasfitter, 5 Trinity place, Belle Vue road Wateridge Frederick William, auctioneer &c. -
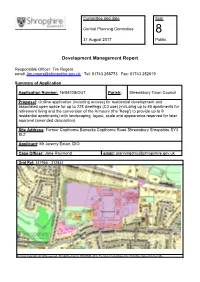
Item 8. 16 04228 out Copthorne Barracks, Item
Committee and date Item Central Planning Committee 8 31 August 2017 Public Development Management Report Responsible Officer: Tim Rogers email: [email protected] Tel: 01743 258773 Fax: 01743 252619 Summary of Application Application Number: 16/04228/OUT Parish: Shrewsbury Town Council Proposal: Outline application (including access) for residential development and associated open space for up to 228 dwellings (C3 use) (including up to 45 apartments for retirement living and the conversion of the Armoury (the 'Keep') to provide up to 9 residential apartments) with landscaping, layout, scale and appearance reserved for later approval (amended description) Site Address: Former Copthorne Barracks Copthorne Road Shrewsbury Shropshire SY3 8LZ Applicant: Mr Jeremy Eaton, DIO Case Officer: Jane Raymond email: [email protected] Grid Ref: 347955 - 312842 © Crown Copyright. All rights reserved. Shropshire Council 100049049. 2016 For reference purposes only. No further copies may be made. Central Planning Committee – 31 August 2017 Item 8 - Former Copthorne Barracks, Copthorne, Road, Shrewsbury, Shropshire Recommendation: Grant Permission subject to the conditions set out in Appendix 1 and a S106 to secure affordable housing, the funding for the provision of a controlled pedestrian crossing on Copthorne Road, a financial primary and secondary education contribution, a financial contribution to be used for improvements to Frankwell County Ground for compensation for the loss of the playing field on site and a financial contribution for use at nearby recreational grounds to compensate for a reduced level of public open space on site. REPORT 1.0 THE PROPOSAL 1.1 This application relates to outline permission for residential development and associated open space with all matters other than access reserved for later approval. -
Flood Defen - Y R
EA-MIDLANDS Shrewsbury flood defen - y r * * 0 ^ The next steps E n v ir o n m e n t A g e n c y Shrewsbury is cradled within a picturesque In addition, a substantial amount of work has been horseshoe loop of the River Severn. Over carried out on all aspects of flooding within the centuries, the river has helped to build the Severn catchment as a whole. This work is still town's character and its prosperity. However, continuing as part of the Severn Flood Management it also brings the damaging threat of Strategy, which is predominately looking at long-term flooding. solutions to flooding issues along the length of the River Severn. In recent years, flooding has become more frequent Shrewsbury flooded 2000 with increased severity, and the Environment Agency has been looking at the possibilities for alleviating the effects in Shrewsbury. The situation in Shrewsbury Following the autumn floods of 2000, the government pledged additional funds to allow work to start on defences for Shrewsbury as a priority. The Agency subsequently carried out consultations and began identifying possible solutions to the flooding problem. Whilst dams, dredging and bypass channels were considered and evaluated, it was concluded that hard defences would provide the most economic and practical flood defences within a reasonable timescale and by utilising the innovative demountable barrier system, the visual impact can be minimised. Site investigations were undertaken throughout Shrewsbury and studies carried out to help establish practical solutions. This work identified that constructing defences to keep out river water was only part of the problem.