Endodontics — Certificate (Post-D.D.S.), M.S.D., M.S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D
The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D Introduction This paper came out of discussions with Hu-Friedy as we were developing new materials describing the Marwan Abou-Rass, or “MAR” microsurgical endodontic instrument line. Since I have been teaching, conducting research and performing microsurgical endodontics for many years, Hu-Friedy was interested in my perspective on the evolution of the specialty, and what the future might hold. I tried to fit it all in the sales brochure we were working on, but how can one compress decades of change into a few short paragraphs? Hence, we decided to make it a separate venture. Since graduating from dental school and completing my endodontic training, I have been immersed in university environments where dialog regarding best practices in endodontics can be collaborative, and sometimes heated -- because my academic and clinical peers are passionate about what we do. Throughout my career I have collaborated with many global peers who have combined innovation and critical thinking with willingness to risk being “wrong”. As a result, the profession has made significant advances for which we have all benefited. It is for them that I dedicate this paper. This paper outlines my perspective on how microsurgical endodontics has progressed over several decades, from its infancy in the 1940s, through developments which have shaped the practice today. I conclude with “educated guesses” regarding what the future may hold. I. The Influence of Oral Surgery Period In the 1940s, endodontic surgery was often performed by oral surgeons, adapting their methods and instruments used for oral surgery. -
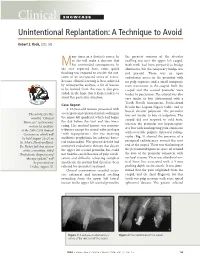
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

On Emerging Clinical Dental Specialties and Recognition Ronald S Brown*
Brown. Int J Pathol Clin Res 2015, 1:1 ISSN: 2469-5807 International Journal of Pathology and Clinical Research Commentary: Open Access On Emerging Clinical Dental Specialties and Recognition Ronald S Brown* Howard University College of Dentistry, USA *Corresponding author: Ronald S. Brown, DDS, MS, Howard University College of Dentistry, 600 W Street, NW, Rm. 406, Washington, DC 20059, USA, Tel: 202-806-0020, Fax: 202-806-0354, E-mail: [email protected] that I am an oral pathologist or oral surgeon, probably because Oral Keywords & Maxillofacial Surgery and Pathology are ADA-recognized dental Oral medicine, Emerging dental specialties, Specialty recognition specialties. It appears that patients, physicians, and even dentists do not understand the difference between these dental/oral disciplines. Commentary Oral Surgery’s main focus is the surgical management of oral and dental conditions, and Oral Pathology’s main focus is the microscopic Dentistry is mainly a surgical clinical profession and dental evaluation of oral, and dental conditions. There are a number of oral clinicians are primarily involved in the surgical management of medicine clinical areas of concern in which Oral Medicine residents oral diseases and conditions. There are a few American Dental are educated and trained, and none of the ADA-recognized clinical Association (ADA)-recognized non-surgical dental specialties such dental specialty residency programs provide education and training as Oral & Maxillofacial Pathology, Oral & Maxillofacial Radiology, [1]. Furthermore, many of these areas of concern particular to oral and Public Health Dentistry. These non-surgical dental specialties medicine clinicians, are not psychometrically evaluated by the are mainly supportive to the surgical dental specialties and general various ADA recognized clinical specialty boards. -

ADEX DENTAL EXAM SERIES: Fixed Prosthodontics and Endodontics
Developed by: Administered by: The American Board of The Commission on Dental Dental Examiners Competency Assessments ADEX DENTAL EXAM SERIES: Fixed Prosthodontics and Endodontics 2019 CANDIDATE MANUAL Please read all pertinent manuals in detail prior to attending the examination Copyright © 2018 American Board of Dental Examiners Copyright © 2018 The Commission on Dental Competency Assessments Ver 1.1- 2019 Exam Cycle Table of Contents Examination and Manual Overview 2 I. Examination Overview A. Manikin Exam Available Formats 4 B. Manikin Exam Parts 4 C. Endodontic and Prosthodontic Typodonts and Instruments 5 D. Examination Schedule Guidelines 6 1. Dates & Sites 6 2. Timely Arrival 6 E. General Manikin-Based Exam Administration Flow 7 1. Before the Exam: Candidate Orientation 7 2. Exam Day: Sample Schedule 7 3. Exam Day: Candidate Flow 8 F. Scoring Overview and Scoring Content 11 1. Section II. Endodontics Content 12 2. Section III. Fixed Prosthodontics Content 12 G. Penalties 13 II. Standards of Conduct and Infection Control A. Standards of Conduct 15 B. Infection Control Requirements 16 III. Examination Content and Criteria A. Endodontics Examination Procedures 19 B. Prosthodontics Examination Procedures 20 C. Endodontics Criteria 1. Anterior Endodontics Criteria 23 2. Posterior Endodontics Criteria 25 D. Prosthodontics Criteria 1. PFM Crown Preparation 27 2. Cast Metal Crown Preparation 29 3. Ceramic Crown Preparation 31 IV. Examination Forms A. Progress Form 34 See the Registration and DSE OSCE Manual for: • Candidate profile creation and registration • Online exam application process • DSE OSCE registration process and examination information / Prometric scheduling processes • ADEX Dental Examination Rules, Scoring, and Re-test processes 1 EXAMINATION AND MANUAL OVERVIEW The CDCA administers the ADEX dental licensure examination. -

Treatment of a Periodontic-Endodontic Lesion in a Patient with Aggressive Periodontitis
Hindawi Publishing Corporation Case Reports in Dentistry Volume 2016, Article ID 7080781, 9 pages http://dx.doi.org/10.1155/2016/7080781 Case Report Treatment of a Periodontic-Endodontic Lesion in a Patient with Aggressive Periodontitis Mina D. Fahmy,1 Paul G. Luepke,1 Mohamed S. Ibrahim,1,2 and Arndt Guentsch1,3 1 Department of Surgical Sciences, Marquette University School of Dentistry, Milwaukee, WI 53233, USA 2Department of Endodontics, Faculty of Dentistry, Mansoura University, Mansoura 35516, Egypt 3Center of Dental Medicine, Jena University Hospital, Friedrich-Schiller-University, An der Alten Post 4, 07743 Jena, Germany Correspondence should be addressed to Arndt Guentsch; [email protected] Received 7 March 2016; Revised 14 May 2016; Accepted 23 May 2016 Academic Editor: Stefan-Ioan Stratul Copyright © 2016 Mina D. Fahmy et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Case Description. This case report describes the successful management of a left mandibular first molar with acombined periodontic-endodontic lesion in a 35-year-old Caucasian woman with aggressive periodontitis using a concerted approach including endodontic treatment, periodontal therapy, and a periodontal regenerative procedure using an enamel matrix derivate. In spite of anticipated poor prognosis, the tooth lesion healed. This seca report also discusses the rationale behind different treatment interventions. Practical Implication. Periodontic-endodontic lesions can be successfully treated if dental professionals follow a concerted treatment protocol that integrates endodontic and periodontic specialties. General dentists can be the gatekeepers in managing these cases. -

Dental Clinic August 31, 2015
DOD SPACE PLANNING CRITERIA CHAPTER 320: DENTAL CLINIC AUGUST 31, 2015 Originating Component: Defense Health Agency Facilities Division Effective: August 31, 2015 Releasability: No Restrictions Purpose: This issuance: To provide space planning criteria guidance in support of planning, programming and budgeting for DoD Military Health System (MHS) facilities. DoD Space Planning Criteria Chapter 320: Dental Clinic August 31, 2015 TABLE OF CONTENTS SECTION 1: PURPOSE AND SCOPE ............................................................................................. 3 SECTION 2: OPERATING RATIONALE AND BASIS OF CRITERIA ........................................ 4 SECTION 3: PROGRAM DATA REQUIRED............................................................................... 11 3.1. Input Data Statements. ..................................................................................................... 11 SECTION 4: SPACE PLANNING CRITERIA .............................................................................. 12 4.1. FA1: Reception. .............................................................................................................. 12 4.2. FA2: General Dentistry. .................................................................................................. 13 4.3. FA3: Specialty Dentistry................................................................................................. 13 4.4. FA4: Dental Radiography. .............................................................................................. 15 -

Position Statement – Implants
Distribution Information AAE members may reprint this position statement for distribution to patients or referring dentists. Implants AAE Position Statement About This Document The following statement was Introduction prepared by the AAE Special The American Association of Endodontists has as its mission the fostering of Committee on Implants. excellence in endodontics and the highest standard of patient care. Our vision is to be a global resource in endodontic knowledge for the profession and the public. ©2007 Dentists and their patients have many alternative treatments available to preserve or replace diseased teeth. In the case of teeth with irreversible pulpal disease, endodontic therapy is a highly predictable method to retain teeth that otherwise would have been extracted. Many large studies show retention rates of more than 90 percent [1, 2]. Alternatively, extracted teeth may be replaced with implants [3-6]. Considerable progress has been made in restoring oral function for patients, but considerably less progress has been made in identifying the best strategies for selecting one treatment approach over another [7, 8], and accordingly, no guidelines set forth by the dental profession regarding endodontic versus implant therapy currently exist. This statement is intended to offer the AAE’s position on this issue. Treatment Planning Based on the Best Evidence Produces Ethical and Effective Results Although there is a lack of clinical trials that directly compare one treatment approach to another [7, 8], there are generally accepted guidelines for the ethical consideration of treatment planning and informed consent. These ethical guidelines provide a framework for all clinical decisions. Quality dental care can only be provided when treatment planning decisions are made by both the dentist and the patient, based on the patient’s general health status and specific oral health needs [9, 10]. -

Performance of Crowns and Bridges, Pan South London – Practical Study Day 11Th June 2015 EBD
Peter Briggs BDS(Hons) MSc MRD FDS RCS (Eng) Consultant in Restorative and Implant Dentistry, QMUL and Specialist Practitioner, Hodsoll House Dentistry. Performance of Crowns and Bridges, Pan South London – Practical Study Day 11th June 2015 EBD Experience Patient Evidence Needs Has the recent focus on direct and indirect adhesive dentistry and Dahl concept compounded our indecision when planning conventional crowns and bridges and being confident to prepare teeth well? Aesthetic restorations looking good comes at a biological price DBC prep = 63% off tooth PFM prep = 72% off tooth PFM prep 20% > FGC prep PFM prep x5 > Porcelain veneer (feathered) x3 > Porcelain veneer (butt joint) Edelhoff & Sorensen (2002). Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent; 87: 503-9 Edelhoff & Sorensen (2002). Tooth structure removal associated with various preparation designs for posterior teeth. Int J Periodontics Restorative Dent; 22: 241–249 The problem is if you do something rarely – unless you have got ‘god-given’ talent or are lucky – when you need to do it you will not be able to execute it well Different types of failure Direct survives less well than indirect It’s about what options we have on failure and failure cycling It is being able to identify: • Do I need conventional luting or can I utilise resin bonding • What material will work best: aesthetically, functionally & cost? • What do I need to do to make it work well? I will struggle here with moisture control – conventional cementation -

Asepsis in Operative Dentistry and Endodontics
International Journal of Public Health Science (IJPHS) Vol.3, No.1, March 2014, pp. 1~6 ISSN: 2252-8806 1 Asepsis in Operative Dentistry and Endodontics Priyanka Sriraman, Prasanna Neelakantan Saveetha Dental College, Saveetha University, Chennai, India Article Info ABSTRACT Article history: Operative (conservative) dentistry and endodontics are specialties of dentistry where the operator is exposed to various infectious agents either via Received Dec 6, 2013 contact with infected tissues, fluids or aerosol. The potential for cross Revised Jan 20, 2014 infection to happen at the dental office is great and every dentist must have a Accepted Feb 26, 2014 thorough knowledge of the concepts of sterilization and disinfection. Disposables should be used wherever possible. Furthermore, the water supply to the dental chair units and water outlets can house biofilms of Keyword: microbes and should be considered as possible sources of infection. This review discusses the importance of following strict aseptic protocols from the Disinfection perspective of operative dentistry and endodontics. Sterilization Cross infection Prions Barrier Copyright © 2014 Institute of Advanced Engineering and Science. Biofilms All rights reserved. Infection control Corresponding Author: Prasanna Neelakantan, Department of Conservative Dentistry and Endodontics, Saveetha University, 162 Poonamallee High Road, Velappanchavadi, Chennai - 600077, Tamil Nadu, India. Email; [email protected] 1. INTRODUCTION Dental professionals are exposed to a variety of micro-organisms present in the blood and saliva of patients, making infection control an issue of utmost importance. Asepsis is the state of being free from disease causing contaminants such as bacteria, viruses, fungi, parasites in addition to preventing contact with micro-organisms. The main goal of infection control is either to reduce or eliminate the chances of microbes getting transferred between the patients, doctors and the dental auxiliaries. -
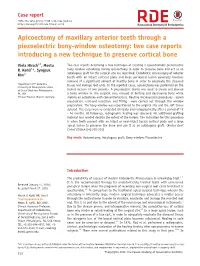
Apicoectomy of Maxillary Anterior Teeth Through a Piezoelectric Bony-Window Osteotomy: Two Case Reports Introducing a New Technique to Preserve Cortical Bone
Case report ISSN 2234-7658 (print) / ISSN 2234-7666 (online) https://doi.org/10.5395/rde.2016.41.4.310 Apicoectomy of maxillary anterior teeth through a piezoelectric bony-window osteotomy: two case reports introducing a new technique to preserve cortical bone Viola Hirsch1,2, Meetu Two case reports describing a new technique of creating a repositionable piezoelectric R. Kohli1*, Syngcuk bony window osteotomy during apicoectomy in order to preserve bone and act as an 1 autologous graft for the surgical site are described. Endodontic microsurgery of anterior Kim teeth with an intact cortical plate and large periapical lesion generally involves removal of a significant amount of healthy bone in order to enucleate the diseased 1 Department of Endodontics, tissue and manage root ends. In the reported cases, apicoectomy was performed on the University of Pennsylvania School of Dental Medicine, Philadelphia, lateral incisors of two patients. A piezoelectric device was used to create and elevate PA, USA a bony window at the surgical site, instead of drilling and destroying bone while 2Private Practice, Munich, Germany making an osteotomy with conventional burs. Routine microsurgical procedures - lesion enucleation, root-end resection, and filling - were carried out through this window preparation. The bony window was repositioned to the original site and the soft tissue sutured. The cases were re-evaluated clinically and radiographically after a period of 12 - 24 months. At follow-up, radiographic healing was observed. No additional grafting material was needed despite the extent of the lesions. The indication for this procedure is when teeth present with an intact or near-intact buccal cortical plate and a large apical lesion to preserve the bone and use it as an autologous graft. -

Principles of Periodontology Andrew R
Marquette University e-Publications@Marquette School of Dentistry Faculty Research and Dentistry, School of Publications 2-1-2013 Principles of Periodontology Andrew R. Dentino Marquette University, [email protected] Seokwoo Lee Jason Mailhot Arthur F. Hefti Marquette University, [email protected] Accepted version. Periodontology 2000, Vol. 61, No. 1 (February 2013): 16-53. DOI. © 1999-2018 John Wiley & Sons, Inc. Used with permission. Marquette University e-Publications@Marquette Dentistry Faculty Research and Publications/School of Dentistry This paper is NOT THE PUBLISHED VERSION; but the author’s final, peer-reviewed manuscript. The published version may be accessed by following the link in the citation below. Periodontology 2000, Vol. 61, No. 1 (2013): 16-53. DOI. This article is © Wiley and permission has been granted for this version to appear in e-Publications@Marquette. Wiley does not grant permission for this article to be further copied/distributed or hosted elsewhere without the express permission from Wiley. Table of Contents Abstract ......................................................................................................................................................... 3 History ........................................................................................................................................................... 5 Early Observations .................................................................................................................................... 5 From -

Paradigms Shifts in Periodontal Therapy: Implementing Evolving Protocols -Kristy Menage Bernie, RDH, MS, RYT – [email protected]
Paradigms Shifts in Periodontal Therapy: Implementing Evolving Protocols -Kristy Menage Bernie, RDH, MS, RYT – [email protected] ‐ Scientific paradigms have long been the cornerstone of clinical practice and daily care, yet many of these paradigms are not the “reality.” Emerging sciences have led to key understanding of new methods to prevent and manage periodontal disease, which has necessitated integration and implementation for the progressive clinician. This interactive session will include a review of accelerated periodontal instrumentation protocols and the new gingivitis code, and incorporate recommendations from the AAP Comprehensive Periodontal Therapy document, which will inspire attendees to unconscious competency! Our Opportunities: Gain an understanding of how change occurs and the influence of paradigms versus the realities of our professional protocols and outcomes. Review innovative and evolving technologies and products designed to prevent and treat periodontal diseases. Implement accelerated periodontal instrumentation protocols based on appropriate periodontal coding, as specified in the AAP treatment guidelines. Pre-Session Assessment: What does this seminar title mean to you? What are your expectations?: List 5 ‘changes’ that have impacted the practice of dental hygiene and/or daily life since the beginning of your career: 1. 2. 3. 4. 5. List 5 ‘changes’ in periodontal therapy you have observed and/or incorporated into practice: 1. 2. 3. 4. 5. 1 www.EducationalDesigns.com 2018© Paradigms ‐ in the philosophy of science, a generally accepted model of how ideas relate to one another, forming a conceptual framework within which scientific research is carried out. vs. Reality ‐ everything that actually does or could exist or happen in real life (practice).