ATSDR Toxicological Profile for Radon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Report to the Legislature: Indoor Air Pollution in California
California Environmental Protection Agency Air Resources Board Report to the California Legislature INDOOR AIR POLLUTION IN CALIFORNIA A report submitted by: California Air Resources Board July, 2005 Pursuant to Health and Safety Code § 39930 (Assembly Bill 1173, Keeley, 2002) Arnold Schwarzenegger Governor Indoor Air Pollution in California July, 2005 ii Indoor Air Pollution in California July, 2005 ACKNOWLEDGEMENTS This report was prepared with the able and dedicated support from Jacqueline Cummins, Marisa Bolander, Jeania Delaney, Elizabeth Byers, and Heather Choi. We appreciate the valuable input received from the following groups: • Many government agency representatives who provided information and thoughtful comments on draft reports, especially Jed Waldman, Sandy McNeel, Janet Macher, Feng Tsai, and Elizabeth Katz, Department of Health Services; Richard Lam and Bob Blaisdell, Office of Environmental Health Hazard Assessment; Deborah Gold and Bob Nakamura, Cal/OSHA; Bill Pennington and Bruce Maeda, California Energy Commission; Dana Papke and Kathy Frevert, California Integrated Waste Management Board; Randy Segawa, and Madeline Brattesani, Department of Pesticide Regulation; and many others. • Bill Fisk, Lawrence Berkeley National Laboratory, for assistance in assessing the costs of indoor pollution. • Susan Lum, ARB, project website management, and Chris Jakober, for general technical assistance. • Stakeholders from the public and private sectors, who attended the public workshops and shared their experiences and suggestions -
Radon-A Physician's Guide: the Health
Radon-A Physician's Guide: The Health Threat With A Simple Solution U.S. Environmental Protection Agency Office of Air and Radiation Indoor Environments Division (6609J) 1. Executive Summary 10. 2. What is Radon? 3. Characteristics and Source of Radon 4. The Health Risk o How does Radon Induce cancer? o What is the Evidence? o Is Occupational Exposure to Radon Comparable to Residential Exposure? 5. What About Smoking and Radon Exposure? The Solution o Why Should Every Home be Tested? o How Do You Obtain a Reliable Test Result? o Radon Testing Methods o Radon Test Devices o How to Test o Interpreting Radon Test Results o Basis for the 4 pCi/L Radon "Action Level" o Radon Reduction Methods 6. Other Indoor Air Pollutants o Environmental Tobacco Smoke (ETS) o Biological Air Pollutants o Volatile Organic Compounds (VOCs) o Other Combustion Products 7. Most Commonly Asked Questions about Radon 8. State and Regional Radon Contacts 9. Additional Information Sources o Radon Publications o Radon Hotlines Introduction Lung cancer's very high associated mortality rate is even more tragic because a significant portion of lung cancer is preventable. While smoking remains the number one cause of lung cancer, radon presents a significant second risk factor. That is why, in addition to encouraging patients to stop smoking, it is important for physicians to inquire about and encourage patients to test for radon levels in their homes. One way to do this is for physicians to join those health care professionals and organizations who have begun to include questions about the radon level in patients' homes on standardized patient history forms. -

Health Effects of Radon Exposure
Review Article Yonsei Med J 2019 Jul;60(7):597-603 https://doi.org/10.3349/ymj.2019.60.7.597 pISSN: 0513-5796 · eISSN: 1976-2437 Health Effects of Radon Exposure Jin-Kyu Kang1,2, Songwon Seo3, and Young Woo Jin3 1Dongnam Radiation Emergency Medical Center, 2Department of Radiation Oncology, Dongnam Institute of Radiological & Medical Sciences, Busan; 3National Radiation Emergency Medical Center, Korea Institute of Radiological & Medical Sciences, Seoul, Korea. Radon is a naturally occurring radioactive material that is formed as the decay product of uranium and thorium, and is estimated to contribute to approximately half of the average annual natural background radiation. When inhaled, it damages the lungs dur- ing radioactive decay and affects the human body. Through many epidemiological studies regarding occupational exposure among miners and residential exposure among the general population, radon has been scientifically proven to cause lung cancer, and radon exposure is the second most common cause of lung cancer after cigarette smoking. However, it is unclear whether ra- don exposure causes diseases other than lung cancer. Media reports have often dealt with radon exposure in relation to health problems, although public attention has been limited to a one-off period. However, recently in Korea, social interest and concern about radon exposure and its health effects have increased greatly due to mass media reports of high concentrations of radon be- ing released from various close-to-life products, such as mattresses and beauty masks. Accordingly, this review article is intended to provide comprehensive scientific information regarding the health effects of radon exposure. Key Words: Radon, inhalation exposure, lung neoplasm INTRODUCTION ical half-life of 55.6 seconds that comes from decay of thori- um. -

The Effects of Radon on Human Health
HEALTH EFFECTS OF RADON RADIATION & NATURE HEALTH EFFECTS OF RADON 2 WHAT IS RADON? • Natural radioactive gas without colour, smell or taste • Product of uranium decay HEALTH EFFECTS OF RADON 3 RADON PRODUCTION For Radon T1/2 = 3.8 days HEALTH EFFECTS OF RADON 4 RADON & LUNG DAMAGE HEALTH EFFECTS OF RADON 5 WHERE DO WE FIND RADON? High concentration Granite soil HEALTH EFFECTS OF RADON 6 WHY RADON GOES INSIDE HOUSES? It’s physics!!! Buildings are at a lower pressure than the surrounding air & soil. Radon & other soil gases are drawn into the building. When air is exhausted, outside air enters the building to replace it. Much of the replacement air comes from the underlying soil. HEALTH EFFECTS OF RADON 7 HOW RADON IS MEASURED? Radioactivity Becquerel (Bq) 1 Bq = 1 nucleus decay per second For Radon, we measure the amount of radioactivity in air volume for a specific amount of time! So... how many Bq in a cubic metre of air m3?! For how long?! Radon exposure: ρtracks / Cf (Bq * h / m3 ) Radon concentration: exposure /exposition time (Bq / m3) HEALTH EFFECTS OF RADON 8 RADON CONCENTRATION FACTORS The amount of radon changes: o During the day o Between summer and winter o With the air temperature More Radon: Winter & Night HEALTH EFFECTS OF RADON 9 RADON LEVELS AROUND THE WORLD HEALTH EFFECTS OF RADON 10 RADON IN ITALY HEALTH EFFECTS OF RADON 11 RADON IN WATER Exposure to radon: 95% from indoor air 1% from drinking water sources Most of this 1% is from inhalation of radon gas released from running water activities, such as bathing, showering and cleaning. -

A Living Radon Reference Manual
A LIVING RADON REFERENCE MANUAL Robert K. Lewis Pennsylvania Department of Environmental Protection Bureau of Radiation Protection, Radon Division and Paul N. Houle, PhD University Educational Services, Inc. Abstract This “living” manual is a compilation of facts, figures, tables and other information pertinent and useful to the radon practitioner, some of which can be otherwise difficult to find. It is envisioned as a useful addition to one’s desk and radon library. This reference manual is also intended to be a “living” document, where its users may supply additional information to the editors for incorporation in revisions as well as updates to this document on-line. Topics contained within the current version include radon chemistry and physics, radon units, radon fans, epidemiology, ambient radon, diagnostics, dosimetry, history, lung cancer, radon in workplace and radon statistics. In some cases motivations and explanations to the information are given. References are included. Introduction This reference manual is a compilation of facts, figures, tables and information on various aspects of radon science. It is hoped that this manual may prove useful to federal and state employees, groups such as AARST and CRCPD, and industry. There are numerous other reference manuals that have been produced on the various aspects of radon science; however, we hope that this manual will have a more “applied” use to all of the various radon practitioners who may use it. Many of the snippets on the various pages are highlights from referenced sources. The snippet will obviously only provide one with the briefest of information. To learn more about that item go to the reference and read the whole paper. -
![17 to Ill PILOT STUDY RISK ASSESSMENT ! II Rn CTT] for SELECTED PROBLEMS at the U FERNALD ENVIRONMENTAL MANAGEMENT PROJECT (FEMP)](https://docslib.b-cdn.net/cover/1170/17-to-ill-pilot-study-risk-assessment-ii-rn-ctt-for-selected-problems-at-the-u-fernald-environmental-management-project-femp-1701170.webp)
17 to Ill PILOT STUDY RISK ASSESSMENT ! II Rn CTT] for SELECTED PROBLEMS at the U FERNALD ENVIRONMENTAL MANAGEMENT PROJECT (FEMP)
;;-!iii;;JI i iiii!; I? BNL-48777 (Rev. 5/93) 17 to ill PILOT STUDY RISK ASSESSMENT ! II rn CTT] FOR SELECTED PROBLEMS AT THE u FERNALD ENVIRONMENTAL MANAGEMENT PROJECT (FEMP) L. D. Hamilton, A. F. Meinhold, S. L. Baxter, S. Holtzman, S. C. Morris, R. Pardi, M. D. Rowe, and C. Sun March 1993 Prepared for Office of Environmental Restoration and Waste Management Office of Technology Development BIOMEDICAL AND ENVIRONMENTAL ASSESSMENT GROUP ii ANALYTICAL SCIENCES DIVISION is :i; DEPARTMENT OF APPLIED SCIENCE i BROOKHAVEN NATIONAL LABORATORY UPTON, LONG ISLAND, NEW YORK 11973 JNSnUBUTfON OF THIS DOCUMENT IS UNLIMITQJ PILOT STUDY RISK ASSESSMENT FOR SELECTED PROBLEMS AT THE FERNALD ENVIRONMENTAL MANAGEMENT PROJECT (FEMP) L.D. Hamilton, A.F. Meinhold, S.L. Baxter, S. Holtzman, S.C. Morris, R. Pardi, M.D. Rowe and C. Sun March 1993 Prepared for Office of Environmental Restoration and Waste Management Office of Technology Development BIOMEDICAL AND ENVIRONMENTAL ASSESSMENT GROUP ANALYTICAL SCIENCES DIVISION DEPARTMENT OF APPLIED SCIENCE BROOKHAVEN NATIONAL LABORATORY UPTON, NY 11973 Under Contract No. DE-ACO2-76CH0O0I6 with the U.S. Department of Energy DISCLAIMER This report was prepared as an account of work sponsored by an agency of the United States Government. Neither the United States Government, no any agency thereof, nor any of their employees, nor any of their contractors, subcontractors or their employees, makes any warranty, express or implied, or assumes any legal liability or responsibility for the completeness or usefulness of any information, apparatus, product or process disclosed, or represents that its use would not infringe on privately owned rights. -

Local Efforts to Reduce Radon Risks Highlights and Lessons Learned Long-Term Exposure to Indoor Radon Can Be Deadly
Local Efforts to Reduce Radon Risks Highlights and Lessons Learned Long-term exposure to indoor radon can be deadly. Radon is the leading cause of lung cancer for non-smokers, and second only to smoking for the entire population. The U.S. Environmental Protection Agency (EPA) estimates that more than 20,000 Americans die of radon-related lung cancer every year. Radon is a colorless, odorless, naturally occurring radioactive gas. Radon seeps into homes and buildings through cracks in the foundation or walls, and can accumulate over time in homes that are not properly vented. The Surgeon General issued a health advisory for radon in 2005, stating that millions of homes have elevated radon levels. The advisory encourages everyone to test their home for radon every 2 years, and to retest after moving, making structural changes, or occupying a previously unused level of a house. EPA recommends that people take action if they find radon at levels greater than or equal to 4 picoCuries per liter (pCi/L). Visit www.epa.gov/radon for more information on how to test your home for radon. The good news is that when elevated radon levels are found they can be reduced, and new homes can be built using easy and inexpensive radon-resistant construction techniques. EPA encourages the building and real estate communities and all new home buyers to demand radon-resistant new construction (RRNC).1 EPA also urges people to test their homes for radon, and to install systems to vent radon from their homes if they find levels at or exceeding the 4 pCi/L action level. -

Genotoxicity Testing for Radon Exposure: Dolichopoda (Orthoptera, Rhaphidophoridae) As Potential Bio-Indicator of Confined Environments
Current Zoology 60 (2): 299–307, 2014 Genotoxicity testing for radon exposure: Dolichopoda (Orthoptera, Rhaphidophoridae) as potential bio-indicator of confined environments Bianca GUSTAVINO*1, Roberta MESCHINI2, Giulia FRANZETTI1, Paolo GRATTON1, Giuliana ALLEGRUCCI1, Valerio SBORDONI1 1 Department of Biology, University of Rome Tor Vergata, Via della Ricerca Scientifica 1, 00133 Rome, Italy 2 Department of Ecological and Biological Sciences, Via San Camillo De Lellis snc, University of Tuscia, 01100 Viterbo, Italy Abstract Radon represents the major source of natural radioactivity in confined environments. Despite the clear evidence of a direct association between residential exposure and human lung cancer provided by case-control studies, results relating indoor exposure and genotoxic/mutagenic effect induction are still contradictory. The present study attempts to estimate the genotoxic effects induced by exposure to radioactive radon in wild cricket populations sampled from caves where varying concentrations of radon are present. Cave crickets are also tested as possible bio-indicator organisms of genotoxic potential of contaminated resi- dential and confined environments. Six caves in Central Italy are considered covering a broad spectrum of radon radioactivity concentration (221–26,000 Bq/m3). Dolichopoda specimens were sampled from each cave; both haemocytes and brain cells taken from individuals were tested for responsiveness to DNA damage induced by radon through the Comet assay. Specimens from the least radioactive cave, housed in controlled conditions for 60 days before analysis, were used as control group. Statistically sig- nificant increase of DNA damage was found in all groups of individuals from each cave, for both cell types. Very low values of all Comet parameters were found in control group individuals, which gave indications of a good responsiveness of the organism to the variable environmental levels of radioactive contamination. -
What Is the Relationship Between Radioactivity and Radon?
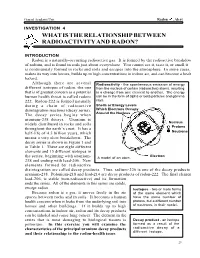
General Academic Unit Radon Alert INVESTIGATION 4 WHAT IS THE RELATIONSHIP BETWEEN RADIOACTIVITY AND RADON? INTRODUCTION Radon is a naturally-occurring radioactive gas. It is formed by the radioactive breakdow of radium, and is found in soils just about everywhere. You cannot see it, taste it, or smell it. is continuously formed in rocks and soils and escapes into the atmosphere. In some cases, makes its way into homes, builds up to high concentrations in indoor air, and can become a healt hazard. Although there are several Radioactivity - the spontaneous emission of energy different isotopes of radon, the one from the nucleus of certain (radioactive) atoms, resulting that is of greatest concern as a potential in a change from one element to another. The energy human health threat is called radon- can be in the form of alpha or beta particles and gamma 222. Radon-222 is formed naturally rays. during a chain of radioactive Shells or Energy Levels disintegration reactions (decay series). Which Electrons Occupy The decay series begins when Around the Nucleus uranium-238 decays. Uranium is widely distributed in rocks and soils Nucleus Protons throughout the earth’s crust. It has a half-life of 4.5 billion years, which Neutrons means a very slow breakdown. The decay series is shown in Figure 1 and in Table 1. There are eight different elements and 15 different isotopes in Electron the series, beginning with uranium- A model of an atom. 238 and ending with lead-206. New elements formed by radioactive disintegration are called decay products. Thus, radium-226 is one of the decay products o uranium-238. -

Attributable Risk of Lung Cancer Deaths Due to Indoor Radon Exposure Si-Heon Kim1, Won Ju Hwang2, Jeong-Sook Cho3 and Dae Ryong Kang4*
Kim et al. Annals of Occupational and Environmental Medicine (2016) 28:8 DOI 10.1186/s40557-016-0093-4 REVIEW Open Access Attributable risk of lung cancer deaths due to indoor radon exposure Si-Heon Kim1, Won Ju Hwang2, Jeong-Sook Cho3 and Dae Ryong Kang4* Abstract Exposure to radon gas is the second most common cause of lung cancer after smoking. A large number of studies have reported that exposure to indoor radon, even at low concentrations, is associated with lung cancer in the general population. This paper reviewed studies from several countries to assess the attributable risk (AR) of lung cancer death due to indoor radon exposure and the effect of radon mitigation thereon. Worldwide, 3–20 % of all lung cancer deaths are likely caused by indoor radon exposure. These values tend to be higher in countries reporting high radon concentrations, which can depend on the estimation method. The estimated number of lung cancer deaths due to radon exposure in several countries varied from 150 to 40,477 annually. In general, the percent ARs were higher among never-smokers than among ever-smokers, whereas much more lung cancer deaths attributable to radon occurred among ever-smokers because of the higher rate of lung cancers among smokers. Regardless of smoking status, the proportion of lung cancer deaths induced by radon was slightly higher among females than males. However, after stratifying populations according to smoking status, the percent ARs were similar between genders. If all homes with radon above 100 Bq/m3 were effectively remediated, studies in Germany and Canada found that 302 and 1704 lung cancer deaths could be prevented each year, respectively. -

Depleted Uranium
WHO/SDE/PHE/01.1 English only Limited Depleted uranium Sources, Exposure and Health Effects Department of Protection of the Human Environment World Health Organization Geneva April 2001 The illustration of the cover page is extracted from Rescue Mission: Planet Earth, ã Peace Child International 1994; used by permission. ã World Health Organization 2001 This document is not issued to the general public and all rights are reserved by the World Health Organization. The document may not be reviewed, abstracted, quoted, reproduced or translated, in part or in whole, without the prior written permission of WHO. No part of this document may be stored in a retrieval system or transmitted in any form or by any means – electronic, mechanical or other without the prior written permission of WHO. The views expressed in documents by named authors are solely the responsibility of those authors. Preface Depleted uranium (DU) has been used in medical and industrial applications for decades but only since its use in military conflicts in the Gulf and the Balkans has public concern been raised about potential health consequences from exposure to it. Concerns have been particularly for peacekeeping forces, humanitarian workers and local populations living and working in areas contaminated by DU following conflict. There has been a large amount of research on the health consequences to workers in the mining and milling of uranium, and on its use in nuclear power, that enables a reasonable assessment of its impact on human health1. Since DU acts chemically in the same way as uranium, and the radiological toxicity is somewhat less than uranium, this research can be used to evaluate health risks from ingestion, inhalation and contact with DU. -

Who Handbook on Indoor Radon
WHO HANDBOOK ON INDOOR RADON A PUBLIC HEALTH PERSPECTIVE WHO HANDBOOK ON INDOOR RADON A PUBLIC HEALTH PERSPECTIVE WHO Library Cataloguing-in-Publication Data WHO handbook on indoor radon: a public health perspective / edited by Hajo Zeeb, and Ferid Shannoun. 1.Radon - adverse effects. 2.Air pollutants, Radioactive. 3.Air pollution, Indoor. 4.Carcinogens, Environmental. 5.Radiation, Ionizing. 6.Lung neoplasms. 7.Environmental exposure. I.Zeeb, Hajo. II.Shannoun, Ferid. III.World Health Organization. ISBN 978 92 4 154767 3 (NLM classification: WN 615) © World Health Organization 2009 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned.