14Th APCP and 4Th APCPN 2012
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

13491-P) CIMB Islamic Bank Berhad 200401032872 (671380-H
CIMB Bank Berhad 197201001799 (13491 -P) CIMB Islamic Bank Berhad 200401032872 (671380-H) Branches closed as at 31st March 2020 Please refer to below list of branches closed and the next nearest available branch: Branches Closed Next nearest available branch 1 CIMB Gleneagles Medini, Nusajaya Retail Branch CIMB Gelang Patah Lot 2, Jalan Medini Utara 4, Medini, 72950 Nusajaya, Retail Branch Johor Darul Takzim 25, Jalan Medan Nusa Perintis 6, Tel:07-5950388 Taman Nusa Perintis 2, 81550 Gelang Fax: 07-5950072 Patah, Johor Tel: 07-530 0000 Fax: 07-530 0017 CIMB Nusa Bestari Branch Retail Branch No 165 & 167, Jalan NB2 2/2 Taman Nusa Bistari 2, 81300 Skudai, Johor Tel: 07-554 8652 / 8471 / 8564 Fax: 07-554 8694 CIMB Perling Branch Retail Branch 382, Jalan Simbang, Taman Perling, 81200 Johor Bharu, Johor. Tel: 07-238 9770 / 6912 Fax: 07-238 0129 2 CIMB Riverson Kota Kinabalu CIMB Bundusan Square Retail Branch Retail Branch No. B-G-59 & B-1-83, Ground & 1st Floor, Lorong Lot 16 Bundusan Square, Jalan Riverson @ Sembulan Off Jalan Coastal, 88100 Kota Bundusan, 88300 Kota Kinabalu, Kinabalu, Sabah Sabah. Tel: 088-276 290 Tel: 088-732 611 / 613 / 614 / 615 Fax: 088-276 296 Fax: 088-732 618 CIMB Damai Plaza Retail Branch Lot No. 41 & 42, Ground Floor, Jalan Damai, Damai Plaza Phase 1, 88300 Kota Kinabalu, Sabah Tel: 088 - 231144 and 088 – 231146 Fax: 088 – 231170 CIMB Jalan Sagunting Preferred Branch Tingkat Bawah, Central Building, Jalan Sagunting 88000 Kota Kinabalu, Sabah Tel: 088-233 214 Fax: 088-242 794 CIMB Bank Berhad 197201001799 (13491 -P) CIMB Islamic Bank Berhad 200401032872 (671380-H) CIMB Inanam Retail Branch Lot 11-0, Inanam Point, Jalan Tuaran, 88450 Kota Kinabalu, Sabah Tel: 088-439 734 / 731 Fax: 088-439 709 CIMB Api Api Centre Retail Branch API-API Centre, Lot 4/G3, 88000 Kota Kinabalu, Sabah Tel: 088-264 287 Fax: 088-211 800 3 CIMB Teluk Panglima Garang CIMB Banting Retail Branch Retail Branch No. -

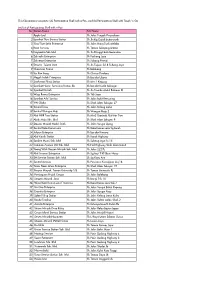
Klinik Panel Selangor
SENARAI KLINIK PANEL (OB) PERKESO YANG BERKELAYAKAN* (SELANGOR) BIL NAMA KLINIK ALAMAT KLINIK NO. TELEFON KOD KLINIK NAMA DOKTOR 20, JALAN 21/11B, SEA PARK, 1 KLINIK LOH 03-78767410 K32010A DR. LOH TAK SENG 46300 PETALING JAYA, SELANGOR. 72, JALAN OTHMAN TIMOR, 46000 PETALING JAYA, 2 KLINIK WU & TANGLIM 03-77859295 03-77859295 DR WU CHIN FOONG SELANGOR. DR.LEELA RATOS DAN RAKAN- 86, JALAN OTHMAN, 46000 PETALING JAYA, 3 03-77822061 K32018V DR. ALBERT A/L S.V.NICKAM RAKAN SELANGOR. 80 A, JALAN OTHMAN, 4 P.J. POLYCLINIC 03-77824487 K32019M DR. TAN WEI WEI 46000 PETALING JAYA, SELANGOR. 6, JALAN SS 3/35 UNIVERSITY GARDENS SUBANG, 5 KELINIK NASIONAL 03-78764808 K32031B DR. CHANDRAKANTHAN MURUGASU 47300 SG WAY PETALING JAYA, SELANGOR. 6 KLINIK NG SENDIRIAN 37, JALAN SULAIMAN, 43000 KAJANG, SELANGOR. 03-87363443 K32053A DR. HEW FEE MIEN 7 KLINIK NG SENDIRIAN 14, JALAN BESAR, 43500 SEMENYIH, SELANGOR. 03-87238218 K32054Y DR. ROSALIND NG AI CHOO 5, JALAN 1/8C, 43650 BANDAR BARU BANGI, 8 KLINIK NG SENDIRIAN 03-89250185 K32057K DR. LIM ANN KOON SELANGOR. NO. 5, MAIN ROAD, TAMAN DENGKIL, 9 KLINIK LINGAM 03-87686260 K32069V DR. RAJ KUMAR A/L S.MAHARAJAH 43800 DENGKIL, SELANGOR. NO. 87, JALAN 1/12, 46000 PETALING JAYA, 10 KLINIK MEIN DAN SURGERI 03-77827073 K32078M DR. MANJIT SINGH A/L SEWA SINGH SELANGOR. 2, JALAN 21/2, SEAPARK, 46300 PETALING JAYA, 11 KLINIK MEDIVIRON SDN BHD 03-78768334 K32101P DR. LIM HENG HUAT SELANGOR. NO. 26, JALAN MJ/1 MEDAN MAJU JAYA, BATU 7 1/2 POLIKLINIK LUDHER BHULLAR 12 JALAN KLANG LAMA, 46000 PETALING JAYA, 03-7781969 K32106V DR. -
This File Contains Two Parts: (A) Participating Shell with E-Pay, and (B) Participating Shell with Touch 'N Go
This file contains two parts: (A) Participating Shell with e-Pay, and (B) Participating Shell with Touch 'n Go (A) List of Participating Shell with e-Pay No Station Name Site Name 1 Apple Leaf Sh Jalan Tengah Perusahaan 2 Syarikat Thye Service Station Sh Jln Kg Gajah Butterworth 3 Eng Thye Setia Enterprise Sh Jalan Hang Tuah Melaka 4 Reza Services Sh Taman Selayang Utama 5 Dayapetro Sdn Bhd Sh Jln Pringgit Batu Berendam 6 Zahiedin Enterprise Sh Puchong Jaya 7 Zahienor Enterprise Sh Subang Permai 8 Stesyen Tujuan Jaya Sh Jln Tujuan Ss18 Subang Jaya 9 Chop Lian Seong Sh Balakong 10 Sin Kee Sang Sh Cheras Perdana 11 Megah Indah Enterprise Sh Bandar Utama 12 Saaharaa Filing Station Sh Mrr 2 Kepong 13 Syarikat Henry Servicing Station SB Sh Bandar Kuala Selangor 14 Syarikat Durrah Sh Jln Tuanku Abdul Rahman Kl 15 Waja Reena Enterprise Sh Ttdi Jaya 16 Syarikat Arbi Service Sh Jalan Bukit Kemuning 17 YW Global Sh Shah Alam Seksyen 27 18 Sentral Tiraz Sh Jalan Kelang Lama 19 Sentral Wangsa Maju Sh Wangsa Maju 2 20 Alaf MRR Two Station Sh Mrr2 Gombak Alaf Mrr Two 21 Abah Maju Sdn. Bhd. Sh Shah Alam Seksyen 9 22 Stesyen Minyak Mohd. Diah Sh Jalan Sungai Ujong 23 Sentral Kota Damansara Sh Kota Damansara Sg Buloh 24 Jufiyun Enterprise Sh Bandar Kinrara 25 Alaf Karak Station Sh Karak Highway 26 Spektra Murni Sdn. Bhd. Sh Subang Jaya Ss 15 27 Common Avenue (M) Sdn. Bhd. Sh Fed Highway Shah Alam Batu3 28 Yeong Wah Stesyen Minyak Sdn. -
RSPO Audit Report
RSPO Principles & Criteria Annual Surveillance Assessment Report Report Number CU821295 RSPO PRINCIPLES & CRITERIA PUBLIC SUMMARY REPORT ANNUAL SURVEILLANCE ASSESSMENT 3 Malaysia KEKAYAAN PALM OIL MILL Kuala Lumpur-Kepong Berhad 2014 Report prepared by: Simon Selvaraj Subramaniam (Lead Assessor) Certification decision by: Nurhadi (Certifier) Certifying Office Control Union (Malaysia) Sdn. Bhd. 150-A, 1st Floor, Persiaran Raja Muda Musa, Off Jalan Sg Bertih, Teluk Gadong, 41100 Klang, Selangor, Malaysia [email protected] Tel: +603-3377 1600 / 1700 Control Union Certifications Control Union Certifications is a member of the Control Union World Group - an international inspection and certification body. CUC performs assessments and certification in many agricultural based fields such as FSC, RSPO, and Organic production, Sustainable Textile Production, Organic Exchange, GLOBALGAP, HACCP, BRC, GMP and GTP. CUC is accredited by the Dutch Council of Accreditation (RVA) on the European quality standard EN 45011 for the inspection and certification of CUC Organic program (according to the EU regulation 2092/91) and GLOBALGAP program. When requested a copy of the accreditation certificate can be obtained from CUC. RSPO Membership Number 8-0025-06-000-00 RSPO Approval Date 12/01/2006 Affiliate Membership http://www.rspo.org/en/member/339 RSPOPC-SUM-REPORT.F01 JULY2013 Page 1 of 41 Control Union (Malaysia) Sdn. Bhd. 150-A, 1st Floor, Persiaran Raja Muda Musa, Off Jalan Sg Bertih, Teluk Gadong, 41100, Klang, Selangor. Malaysia. Tel: +603-3377 1600 / 1700 RSPO Principles & Criteria Annual Surveillance Assessment Report Report Number CU821295 Table of Contents PART 1: SCOPE OF THE CERTIFICATION ASSESSMENT AUDIT .............................................................. 4 1.1 COMPANY AND CONTACT DETAILS ..................................................................................................... -
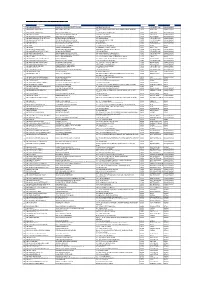
Shell Lebih Ekstra at Zalora Promotion Participating Stations List NO SITE
Shell Lebih Ekstra at Zalora Promotion Participating Stations List NO SITE NAME STATION NAME ADDRESS POSCODE CITY STATE 1 SH JALAN JELUTONG BAN LEONG SHELL PRODUCTS SDN BHD 347 JELUTONG ROAD 11600 GEORGETOWN PULAU PINANG 2 SH BANDAR AYER ITAM 2 BBAI SHELL SERVICES LOT 2499 JALAN THEAN TEIK, JALAN SHAIK MADAR BANDAR 11500 AYER ITAM PULAU PINANG BARU 3 SH BANDAR AYER ITAM 1 BBAI SALES & SERVICES 12 ANGSANA FARLIM ROAD 11500 AYER ITAM PULAU PINANG 4 SH BUKIT GELUGOR BUKIT GLUGOR SERVICE STATION 210 BUKIT GELUGOR 11700 GELUGOR PULAU PINANG 5 SH JLN MAYANG PASIR BAYAN BARU CERGAS SAUJANA SDN BHD JALAN MAYANG PASIR 11950 BAYAN BARU PULAU PINANG 6 SH JALAN BURMAH GEORGE TOWN ELITEBAY EXPRESS ENTERPRISE 378 JALAN BURMA 10350 GEORGETOWN PULAU PINANG 7 SH JALAN MESJID NEGERI GREEN ISLAND SERVICE STATION 4A JALAN MASJID NEGERI 11600 GEORGETOWN PULAU PINANG 8 SH BALIK PULAU KEAN YOON FATT FILLING STATION 315 GENTING 11000 BALIK PULAU PULAU PINANG 9 SH WELD QUAY LEAN HONG CO SDN BHD 30 WELD QUAY 10300 GEORGETOWN PULAU PINANG 10 SH GERIK MAESTRO ONE ENTERPRISE 122 JLN SULTAN ISKANDAR 33300 GERIK PERAK 11 SH LAWIN MEERA AAZ ENTERPRISE 2B KAMPUNG MALAU, LAWIN 33410 LENGGONG PERAK 12 SH JELUTONG EXPRESSWAY MILYAR MUTIARA ENTERPRISE LEBUHRAYA TUN DR LIM CHONG EU 11600 GEORGETOWN PULAU PINANG 13 SH JALAN PERAK GEORGE TOWN MS MASHA ENTERPRISE 190 JALAN PERAK 10150 GEORGETOWN PULAU PINANG 14 SH JALAN KELAWEI BIRCH MUKAH HEAD SERVICE STATION 2A JALAN KELEWAI / JALAN BIRCH 10250 GEORGETOWN PULAU PINANG 15 SH JALAN PAYA TERUBONG PAYA TERUBONG SERVICE STATION -
Rspo Principles & Criteria Public Summary Report
RSPO Principles & Criteria Annual Surveillance Assessment Report Report Number CU822632 RSPO PRINCIPLES & CRITERIA PUBLIC SUMMARY REPORT ANNUAL SURVEILLANCE ASSESSMENT 1 Malaysia TUAN MEE OIL MILL Kuala Lumpur-Kepong Berhad 2014 Report prepared by: Mahaswaran Maliyapan (Lead Assessor) Certification decision by: Gerben Stegeman (Certifier) Certifying Office Control Union (Malaysia) Sdn. Bhd. 150-A, 1st Floor, Persiaran Raja Muda Musa, Off Jalan Sg Bertih, Teluk Gadong, 41100 Klang, Selangor, Malaysia [email protected] Tel: +603 -3377 16 00 / 1700 Control Union Certifications Control Union Certifications is a member of the Control Union World Group - an international inspection and certification body. CUC performs assessments and certification in many agricultural based fields such as FSC, RSPO, and Organic production, Sustainable Textile Production, Organic Exchange, GLOBALGAP, HACCP, BRC, GMP and GTP. CUC is accredited by the Dutch Council of Accreditation (RVA) on the European quality standard EN 45011 for the inspection and certification of CUC Organic program (according to the EU regulation 2092/91) and GLOBALGAP program. When requested a copy of the accreditation certificate can be obtained from CUC. Control Union (Malaysia) Sdn Bhd is a registered affiliate member of RSPO and is a private limited company owned by the Control Union World Group based in Malaysia. Control Union (Malaysia) Sdn Bhd is authorized to conduct and issue certification on behalf of RSPO and Control Union Certifications. RSPO Membership Number 8-0025-06-000-00 RSPO Approval Date 12/01/2006 Affiliate Membership http://www.rspo.org/en/member/339 RSPOPC-SUM-REPORT.F01 JULY2013 Page 1 of 54 Control Union (Malaysia) Sdn. Bhd. -

Majlis Perbandaran Klang
HARGA DOKUMEN RM 40.00 MAJLIS PERBANDARAN KLANG DOKUMEN SEBUT HARGA KERJA UNTUK NO. SEBUT HARGA: MPK/JK 600-13/6/13 (2018) CADANGAN PENGGANTIAN TIANG LAMPU JENIS FIBER LELENGAN BERKEMBAR (DOUBLE ARM) KEPADA TIANG JENIS GALVANI (HOT DIPPED GALVANISED) DAN KERJA- KERJA MEMBAIKPULIH KESELURUHAN SISTEM KABEL DAN PENDAWAIAN DI PERSIARAN RAJA MUDA MUSA DARI SIMPANG JALAN KIM CHUAN HINGGA SIMPANG JALAN SUNGAI KELADI PELABUHAN KLANG. Pendaftaran : Sijil Perolehan Kerja Kerajaan (SSPK) oleh CIDB Unit Perancang Ekonomi Negeri Selangor (UPEN) E-Tender Negeri Selangor Gred : G2 Kategori / Pengkhususan : ME/ E11 & E04 Tarikh Iklan : 08.10.2018 Tarikh Lawatan : 12.10.2018 Tarikh Jualan : 16.10.2018 Tarikh Tutup S/harga : 22.10.2018 Tempoh Siap Kerja : 10 MINGGU Denda Lewat Siap Kerja : 0.5% daripada nilai kontrak bagi setiap hari kelewatan yang berlaku Penyata Bank : Julai 2018, Ogos 2018, September 2018 SENARAI SEMAKAN DOKUMEN TAWARAN SEBUT HARGA KERJA NO. FAIL : ........................................................................ Sila tandakan ( / ) bagi dokumen-dokumen yang disertakan. Bil. Perkara/Dokumen Untuk Di tanda Untuk Di tanda oleh Syarikat oleh Jawatankuasa Pembuka Sebut Harga 1 Salinan Resit Pembelian dokumen 2 Surat Akuan Pembida yang diisi lengkap – Lampiran A1 m/s 2/1/1 3 Borang Sebutharga Kerja yang diisi lengkap (termasuk nilai tawaran dan tempoh siap) serta ditandatangani dan bercop - m/s 5/1/1 4 Surat Pengakuan Kebenaran Maklumat Dan Keesahan Dokumen yang dikemukakan oleh penyebutharga telah diisi lengkap. – Borang A m/s A1 -

Senarai Semua Lokasi Hotspot Wifi Smart Selangor Adalah Seperti Berikut
Senarai semua lokasi hotspot WiFi Smart Selangor adalah seperti berikut:- No. Site Address Category 1 Masjid Nurul Yaqin Mosque Kampung Melayu Seri Kundang, 48050 Rawang, Selangor 2 Pusat Gerakan Khidmat Masyarakat (DUN Kuang) Government 6-1-A, Jalan 7A/2, Bandar Tasik Puteri, 48000 Rawang, Selangor 3 HOSPITAL SUNGAI BULOH_300014, 47000 Hospital Sungai Buloh Selangor 4 HOSPITAL SUNGAI BULOH_300014 Hospital 5 HOSPITAL SUNGAI BULOH_300014 Hospital 6 HOSPITAL SUNGAI BULOH_300014 Hospital 7 HOSPITAL SUNGAI BULOH_300014 Hospital 8 HOSPITAL SUNGAI BULOH_300014 Hospital 9 Perodua Service Centre Jln Sungai Pintas, No.14, Commercial Jalan TSB 10, Taman Industri Sg. Buloh 47000 Shah Alam selangor 10 TESCO RAWANG_300026, No.1, Jalan Rawang Mall 48000 Rawang Selangor 11 TM POINT RAWANG, TM Premises Lot 21, Jalan Maxwell 48000 Rawang 12 Stadium MPS, Jalan Persiaran 1, Bandar Baru Stadium Selayang, 68100 Batu Caves, Selangor 13 Pejabat Cawangan Rawang, Jalan Bandar Rawang Government 2, Bandar Baru Rawang, 48000 Rawang, Selangor 14 No. 309 Felda Sungai Buaya, 48010 Rawang, Residential Selangor area 15 Traffic Light Chicken Rice Sungai Choh, 48009 F&B outlet Rawang, Selangor 16 Pejabat Khidmat Rakyat (DUN Rawang) Government No.13, Jalan Bersatu 8 (Tingkat Bawah), Taman Bersatu, 48000 Rawang, Selangor 17 WTC Restoran F&B Outlet Rawang new town, 48000 Rawang, Selangor 18 Medan Selera MPS F&B Outlet Rawang Integrated Industrial Park, 45000 Rawang, Taman Tun Teja, Rawang, Selangor 19 Medan Selera F&B Outlet Bandar Country Homes, 48000 Rawang, Selangor 20 Kompleks JKKK, Selayang Baru, JKR 750C, Dewan Government Orang Ramai, Jalan Besar Selayang Baru, 68100 Batu Caves, Selangor 21 Pejabat Ahli Parlimen Selayang,12A, Jalan SJ 17, Government Taman Selayang Jaya, 68100 Batu Caves, Selangor No. -

Logistics Value Chain Key Points 1. This Chapter Has Identified
CHAPTER FOUR: Logistics value chain Contents: Introduction, Overview on Logistics Value Chain, Key Elements for Value Chain Analysis for RURB, The Seven-step Sea Freight Transportation Model, Logistics Value Chain Models, Sea Freight Logistics Stakeholder Analysis, Standard Industrial Classification of Freight Logistics, Logistics Trade Directory, Appendix Key Points 1. This chapter has identified the various conceptual frameworks that have been developed for logistics studies. The frameworks are generally process or activity-based, focusing on the chain of activities involved in import-export logistics. The number of different frameworks shows the complexity of logistics activities, as each framework focuses its own specific purpose. 2. This RURB study focuses on sea freight import-export logistics. It is using the process-based model that resembles the industry’s perspectives of logistics activities. As such the industry Seven-step Sea Freight Transportation framework provides clarity on the analysis of the logistics value chain. To support value chain analysis, consideration is made on the product-based perspective of logistics activities. 3. The WTO Trade Facilitation framework’s main purpose is to ensure a common understanding of trade rules between economies so that goods can move smoothly and efficiently between them. 4. The World Bank Trading Across Borders framework serves to benchmark between economies in the import-export sea freight logistics. This particular benchmark indicator is one of ten indicators to rank economies by the ease of doing business. 5. Another World Bank benchmarking framework is the Logistics Performance Indicators that measures and benchmarks logistics quality among economies. The measures are made from perception studies of freight forwarders in the import-export activities. -

Kod Perakaunan 2021 V.1 50580 Kuala Lumpur - 1
BAHAGIAN AKAUN KEMENTERIAN KERJA RAYA MALAYSIA TINGKAT 1, BLOK A, KOMPLEKS KERJA RAYA JALAN SULTAN SALAHUDDIN PANDUAN KOD PERAKAUNAN 2021 V.1 50580 KUALA LUMPUR - 1 - MALAYSIA V.1 K A N D U N G A N M/S - STRUKTUR KOD-KOD PERAKAUNAN 3-5 - KOD PEJABAT PERAKAUNAN 7-9 SENARAI VOT SEPERTI DI ANGGARAN - PERBELANJAAN PERSEKUTUAN 11-13 - KOD PEGAWAI PENGAWAL 15-17 - KOD VENDOR iGFMAS 19 - KOD KUMPULAN PTJ 21-24 - KOD PUSAT TANGGUNGJAWAB (PTJ) 26-28 KOD PUSAT TANGGUNGJAWAB (PTJ NEGERI / - DAERAH) 30-39 - KOD PROGRAM / AKTIVITI 41-47 - KOD CAA AMANAH/DEPOSIT/SUBSIDIARI 49-50 - KOD PROJEK KKR (P27) 52-78 - KOD CAA HASIL 80-82 - KOD CAA BELANJA 84-85 - KOD CAA ASET DIPERMODALKAN 87 - KOD DEPOSIT KERJA (P98) 89-99 - RUMUSAN 101 PANDUAN KOD PERAKAUNAN 2021 V.1 - 2 - STRUKTUR KOD-KOD PERAKAUNAN 1. PENGENALAN 1.1 Manual Prosedur Kod Perakaunan bertujuan untuk menerangkan penggunaan kod perakaunan yang diperlukan untuk merekodkan urusniaga kewangan dan perakaunan di 1GFMAS. 2. STRUKTUR KOD-KOD 2.1 Berikut adalah struktur kod-kod perakaunan yang berkaitan : Aksara Bil. Perihal Catatan / Digit i. Kod Vot 3 - Ditetapkan oleh Kementerian Kewangan. - Dimulai dengan huruf ‘B’ / ‘T’ untuk belanja mengurus, huruf ‘P’ untuk belanja pembangunan atau huruf ‘ S’ untuk ‘Private Finance Initiative (PFI)’. ii. Kod Pegawai Pengawal 2 - Mengikut turutan berdasarkan kedudukan Kementerian/Jabatan di dalam Anggaran Perbelanjaan Persekutuan Dicatatkan bersama kod PTJ akan menjadikan iii. Kod Kumpulan PTJ 2 - kod PTJ sesebuah Kementerian/Jabatan itu unik. iv. Kod Pusat Tanggungjawab/ 6 - Ditetapkan oleh Kementerian mengikut Pusat Kos (PTJ/PK) keperluan masing-masing. -

Marketing Brochure
2021 Megalift Malaysia The World’s Top Project Cargo Specialists Project Cargo Network (PCN) is an energy technology is providing a rapid organisation established to provide a increase in business opportunities for networking platform for the world’s top project cargo specialists who have the project cargo specialists. required capabilities in the supply chain Together with their fellow PCN overseas management of oversize plant and offices,Megalift Sdn Bhdcan handle the equipment, i.e. wind turbines. transportation of oversized and heavy items or shipments that consist of complex Because most PCN Member offices are By working in close components that must be disassembled, managed by privately-owned shipped and then re-assembled. independent companies, they can focus co-operation with Megalift Sdn Bhd can offer project cargo 100% on providing a personal service that their fellow PCN management for engineering, is tailored to client’s needs. Members, procurement and construction companies Some multinational transport companies servicing energy, mining, chemical, are restricted by inflexible policies and petrochemical, pipeline, infrastructure and Megalift Sdn Bhd other sectors. procedures. provide first class local These highly specialist shipments require Megalift Sdn Bhdand their fellow PCN individual transport planning from origin to Members can accommodate specific service on a truly destination. requests and make immediate decisions international scale. The current world trend for green energy and recommendations on each individual and the substantial investment in clean shipment. Megalift Sdn Bhd + Overseas Partners Megalift Sdn Bhd offer clients the personal local service and flexibility that only a privately-owned forwarder can, providing comprehensive logistics solutions through local people who have an in-depth understanding of their market. -

State Address Taman Desa 58100 Off Jalan Kelang Lama, 58000 KLSC
State Address Kuala Lumpur Taman Desa 58100 Off Jalan Kelang Lama, 58000 KLSC Wangsa Maju, 53300 Jalan Yap Kwan Seng, 50450 Taman Tun Dr Ismail, 60000 Jalan Segambut, 51200 Jalan Ampang, 50450 Berjaya Times Square, 55100 Taman Ehsan, Kepong, 52100 Taman Melawati, 53100 Jalan Tun Perak, 50050 Plaza Wangsa Maju, Seksyen 10, 53300 Bandar Sri Permaisuri,56000, Cheras Bandar Damai Perdana, 56000 Cheras Taman Usahawan Kepong, 52100 Overseas Union Garden, 58200 Off Jalan Genting Kelang, 53300 Taman Dahlia Cheras, 56000 Taman Cheras, 56100 Taman Maluri, Cheras, 55100 Taman Segar, 56100 Jalan Kerinchi, Bangsar South, 59200 Bandar Baru Sri Petaling, 57000 Bangsar Baru, 59100 Taman Bukit Anggerik, 56000 Desa Pandan 55100 Taman Bukit Cheras 56000 Jalan Kelang Lama, 58200 Jalan Sultan Ismail, 50450 Selangor Subang Jaya, 47500 Ampang Point, Ampang 68000 Taman Putra, 68000 Ampang Kota Damansara,Petaling Jaya, 47810 Damansara Perdana, Petaling Jaya 47820 Ara Damansara 47301 Off Jln Damansara 46350 Jalan Stesen Klang 41000 Persiaran Tasik, Shah Alam, 40000 Persiaran Raja Muda Musa, Port Klang, 42000 Jalan Sungai Bertek, Klang 41000 Main Road, Jenjarom, 42600 Selangor Jalan Besar Pandamaran, Port Klang 42000 Taman Ramal Indah, Kajang 43000 Seksyen 18 Shah Alam 40000 Taman Pelangi Semenyih, 43500 Semenyih Bandar Tasik Kesuma, Beranang, 43700 Bandar Sungai Long, Kajang 43200 Taman Connaught, Cheras, 56000 Seksyen U5, Shah Alam, 40150 Pusat Bandar Wangsa Maju, 53300 Ampang Waterfront, 68000 Jalan SS2, Petaling Jaya, 47300 Bandar Puteri, Puchong, 47100 Jalan