Does Viloxazine Have Epileptogenic Properties?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WELLBUTRIN SR Safely and Effectively
HIGHLIGHTS OF PRESCRIBING INFORMATION psychosis, hallucinations, paranoia, delusions, homicidal ideation, These highlights do not include all the information needed to use aggression, hostility, agitation, anxiety, and panic, as well as suicidal WELLBUTRIN SR safely and effectively. See full prescribing ideation, suicide attempt, and completed suicide. Observe patients information for WELLBUTRIN SR. attempting to quit smoking with bupropion for the occurrence of such symptoms and instruct them to discontinue bupropion and contact a WELLBUTRIN SR (bupropion hydrochloride) sustained-release tablets, healthcare provider if they experience such adverse events. (5.2) for oral use • Initial U.S. Approval: 1985 Seizure risk: The risk is dose-related. Can minimize risk by gradually increasing the dose and limiting daily dose to 400 mg. Discontinue if WARNING: SUICIDAL THOUGHTS AND BEHAVIORS seizure occurs. (4, 5.3, 7.3) See full prescribing information for complete boxed warning. • Hypertension: WELLBUTRIN SR can increase blood pressure. Monitor blood pressure before initiating treatment and periodically during • Increased risk of suicidal thinking and behavior in children, treatment. (5.4) adolescents and young adults taking antidepressants. (5.1) • Activation of mania/hypomania: Screen patients for bipolar disorder and • Monitor for worsening and emergence of suicidal thoughts and monitor for these symptoms. (5.5) behaviors. (5.1) • Psychosis and other neuropsychiatric reactions: Instruct patients to contact a healthcare professional if such reactions occur. (5.6) --------------------------- INDICATIONS AND USAGE ---------------------------- • Angle-closure glaucoma: Angle-closure glaucoma has occurred in WELLBUTRIN SR is an aminoketone antidepressant, indicated for the patients with untreated anatomically narrow angles treated with treatment of major depressive disorder (MDD). (1) antidepressants. -

Concomitant Drugs Associated with Increased Mortality for MDMA Users Reported in a Drug Safety Surveillance Database Isaac V
www.nature.com/scientificreports OPEN Concomitant drugs associated with increased mortality for MDMA users reported in a drug safety surveillance database Isaac V. Cohen1, Tigran Makunts2,3, Ruben Abagyan2* & Kelan Thomas4 3,4-Methylenedioxymethamphetamine (MDMA) is currently being evaluated by the Food and Drug Administration (FDA) for the treatment of post-traumatic stress disorder (PTSD). If MDMA is FDA-approved it will be important to understand what medications may pose a risk of drug– drug interactions. The goal of this study was to evaluate the risks due to MDMA ingestion alone or in combination with other common medications and drugs of abuse using the FDA drug safety surveillance data. To date, nearly one thousand reports of MDMA use have been reported to the FDA. The majority of these reports include covariates such as co-ingested substances and demographic parameters. Univariate and multivariate logistic regression was employed to uncover the contributing factors to the reported risk of death among MDMA users. Several drug classes (MDMA metabolites or analogs, anesthetics, muscle relaxants, amphetamines and stimulants, benzodiazepines, ethanol, opioids), four antidepressants (bupropion, sertraline, venlafaxine and citalopram) and olanzapine demonstrated increased odds ratios for the reported risk of death. Future drug–drug interaction clinical trials should evaluate if any of the other drug–drug interactions described in our results actually pose a risk of morbidity or mortality in controlled medical settings. 3,4-Methylenedioxymethamphetamine (MDMA) is currently being evaluated by the Food and Drug Adminis- tration (FDA) for the treatment of posttraumatic stress disorder (PTSD). During the past two decades, “ecstasy” was illegally distributed and is purported to contain MDMA, but because the market is unregulated this “ecstasy” may actually contain adulterants or no MDMA at all1. -

(12) Patent Application Publication (10) Pub. No.: US 2013/0203752 A1 Blough Et Al
US 201302O3752A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0203752 A1 Blough et al. (43) Pub. Date: Aug. 8, 2013 (54) PHENYLMORPHOLINES AND ANALOGUES Publication Classification THEREOF (51) Int. Cl. (76) Inventors: Bruce E. Blough, Raleigh, NC (US); C07D 265/30 (2006.01) Richard Rothman, Ellicott City, MD (52) U.S. Cl. (US); Antonio Landavazo, Raleigh, NC CPC .................................... C07D 265/30 (2013.01) (US); Kevin M. Page, Willow Spring, USPC ......... 514/231.2: 544/106; 544/174: 544/163 NC (US); Ann Marie Decker, Durham, NC (US) (57) ABSTRACT (21) Appl. No.: 13/698,892 Provided herein are compounds and prodrugs and methods of (22) PCT Filed: May 20, 2011 preparation of compounds and prodrugs that are capable of functioning as releasers and/or uptake inhibitors of one or (86). PCT No.: PCT/US2011/037361 more monoamine neurotransmitters, including dopamine, serotonin, and norepinephrine. Also provided are pharmaceu S371 (c)(1), tical compositipos1u1ons compris1ng one or more OIf uneseth com (2), (4) Date: Mar. 4, 2013 pounds or prodrugs, which may further comprise one or more Related U.S. Application Data additional therapeutic agents. Also provided are methods of treatment of various conditions that may be responsive to (60) Provisional application No. 61/347,259, filed on May modification of monoamine neutrotransmitter levels, such as 21, 2010. pre-obesity, obesity, addiction, and depression. US 2013/0203752 A1 Aug. 8, 2013 PHENYLMORPHOLINES AND ANALOGUES 0006 Another anorectic, which was prescribed for the THEREOF short-term treatment of obesity, is phenmetrazine Phenmetra Zine is reportedly a potent Substrate for norephinephrine and FEDERALLY SPONSORED RESEARCHOR dopamine transporters and displays stimulant properties DEVELOPMENT similar to those of amphetamines. -

The Use of Boron-Doped Diamond Electrode for the Determination of Selected Biocides in Water Samples
water Article The Use of Boron-Doped Diamond Electrode for the Determination of Selected Biocides in Water Samples Katarzyna Mielech-Łukasiewicz * and Barbara Starczewska Institute of Chemistry, University of Białystok, Ciołkowskiego 1 K, 15-245 Białystok, Poland * Correspondence: [email protected]; Tel.: +48-85-738-80-65 Received: 24 June 2019; Accepted: 30 July 2019; Published: 31 July 2019 Abstract: In recent years, the remains of chemical substances in water environments, referred to as emerging organic contaminations, have been more and more often studied by analysts. This work shows the possibility of using a boron-doped diamond electrode to determine low concentration levels of remains of pharmaceuticals in environmental samples. The study focused on selected biocides from the group of azole fungicides (itraconazole and posaconazole) and was performed using quick and sensitive electrochemical methods. The cyclic voltammetry method was used in order to determine the properties of these compounds, whereas analytical characterization was performed using square wave voltammetry. The work involved the specification of the optimum electrooxidation conditions of the selected fungicides, their comparative characterization, and the development of a new, sensitive methods of itraconazole and posaconazole assay. The proposed procedures allowed us to determine itraconazole in the range from 7.9 10 8 to 1.2 10 6 moL L 1 and posaconazole in the range from × − × − · − 5.7 10 8 to 8.44 10 7 moL L 1. The relative standard deviation of the measurements did not × − × − · − exceed 5.85%. The developed procedures were successfully used to determine itraconazole and posaconazole concentration in water samples and the assay recovery was between 93.5% and 102.8%. -

Compositions and Methods for Selective Delivery of Oligonucleotide Molecules to Specific Neuron Types
(19) TZZ ¥Z_T (11) EP 2 380 595 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 26.10.2011 Bulletin 2011/43 A61K 47/48 (2006.01) C12N 15/11 (2006.01) A61P 25/00 (2006.01) A61K 49/00 (2006.01) (2006.01) (21) Application number: 10382087.4 A61K 51/00 (22) Date of filing: 19.04.2010 (84) Designated Contracting States: • Alvarado Urbina, Gabriel AT BE BG CH CY CZ DE DK EE ES FI FR GB GR Nepean Ontario K2G 4Z1 (CA) HR HU IE IS IT LI LT LU LV MC MK MT NL NO PL • Bortolozzi Biassoni, Analia Alejandra PT RO SE SI SK SM TR E-08036, Barcelona (ES) Designated Extension States: • Artigas Perez, Francesc AL BA ME RS E-08036, Barcelona (ES) • Vila Bover, Miquel (71) Applicant: Nlife Therapeutics S.L. 15006 La Coruna (ES) E-08035, Barcelona (ES) (72) Inventors: (74) Representative: ABG Patentes, S.L. • Montefeltro, Andrés Pablo Avenida de Burgos 16D E-08014, Barcelon (ES) Edificio Euromor 28036 Madrid (ES) (54) Compositions and methods for selective delivery of oligonucleotide molecules to specific neuron types (57) The invention provides a conjugate comprising nucleuc acid toi cell of interests and thus, for the treat- (i) a nucleic acid which is complementary to a target nu- ment of diseases which require a down-regulation of the cleic acid sequence and which expression prevents or protein encoded by the target nucleic acid as well as for reduces expression of the target nucleic acid and (ii) a the delivery of contrast agents to the cells for diagnostic selectivity agent which is capable of binding with high purposes. -

MEDICATION GUIDE WELLBUTRIN® (WELL Byu-Trin) (Bupropion Hydrochloride) Tablets
NDA 018644/S-041 NDA 020358/S-048 Page 6 MEDICATION GUIDE WELLBUTRIN® (WELL byu-trin) (bupropion hydrochloride) Tablets Read this Medication Guide carefully before you start using WELLBUTRIN and each time you get a refill. There may be new information. This information does not take the place of talking with your doctor about your medical condition or your treatment. If you have any questions about WELLBUTRIN, ask your doctor or pharmacist. IMPORTANT: Be sure to read the three sections of this Medication Guide. The first section is about the risk of suicidal thoughts and actions with antidepressant medicines; the second section is about the risk of changes in thinking and behavior, depression and suicidal thoughts or actions with medicines used to quit smoking; and the third section is entitled “What Other Important Information Should I Know About WELLBUTRIN?” Antidepressant Medicines, Depression and Other Serious Mental Illnesses, and Suicidal Thoughts or Actions This section of the Medication Guide is only about the risk of suicidal thoughts and actions with antidepressant medicines. Talk to your, or your family member’s, healthcare provider about: • all risks and benefits of treatment with antidepressant medicines • all treatment choices for depression or other serious mental illness What is the most important information I should know about antidepressant medicines, depression and other serious mental illnesses, and suicidal thoughts or actions? 1. Antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, and young adults within the first few months of treatment. 2. Depression and other serious mental illnesses are the most important causes of suicidal thoughts and actions. -
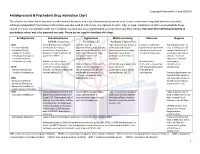
Antidepressant & Psychedelic Drug Interaction Chart
Copyright Psychedelic School 8/2020 Antidepressant & Psychedelic Drug Interaction Chart This chart is not intended to be used to make medical decisions and is for informational purposes only. It was constructed using data whenever possible, although extrapolation from known information was also used to inform risk. Any decision to start, stop, or taper medication and/or use psychedelic drugs should be made in conjunction with your healthcare provider(s). It is recommended to not perform any illicit activity. This chart the intellectual property of psychedelic school and is for personal use only. Please do not copy or distribute this chart. Antidepressant Phenethylamines Tryptamines MAOI-containing Ketamine Ibogaine -MDMA, mescaline -Psilocybin, LSD -Ayahuasca, Syrian Rue SSRIs Taper & discontinue at least 2 Consider taper & Taper & discontinue at least 2 Has been studied and Taper & discontinue at · Paroxetine (Paxil) weeks prior (all except discontinuation at least 2 weeks weeks prior (all except found effective both with least 2 weeks prior (all · Sertraline (Zoloft) fluoxetine) or 6 weeks prior prior (all except fluoxetine) or 6 fluoxetine) or 6 weeks prior and without concurrent except fluoxetine) or 6 · Citalopram (Celexa) (fluoxetine only) due to loss of weeks prior (fluoxetine only) (fluoxetine only) due to use of antidepressants weeks prior (fluoxetine · Escitalopram (Lexapro) psychedelic effect due to potential loss of potential risk of serotonin only) due to risk of · Fluxoetine (Prozac) psychedelic effect syndrome additive QTc interval · Fluvoxamine (Luvox) MDMA is unable to cause Recommended prolongation, release of serotonin when the Chronic antidepressant use may Life threatening toxicities can to be used in conjunction arrhythmias, or SPARI serotonin reuptake pump is result in down-regulation of occur with these with oral antidepressants cardiotoxicity · Vibryyd (Vilazodone) blocked. -

DRUGS and DRIVING: January 1978 a SELECTED BIBLIOGRAPHY 6
Technical Report Pocumtotim Pago 1. Rmrr He I. krrmmt Acce#r~mMe. (<izi19 ----- -- J. Ropott Oete DRUGS AND DRIVING: January 1978 A SELECTED BIBLIOGRAPHY 6. Pr~orn~ng~~gan~gotion code ----- . 8. Pmrfomrng Organctat~onUrnport NO. Alan C. Donelson UM-HSRI-78-3 10 Woh Un~tNo (TRAIS) I I. Conttect or Grant No. DOT-HS-7-01530 13. Type of Repoft and Petlod Covmrd ---------- '1 dministration , July 1975 - November 1976 14. Sponsoring Agency Codr This report presents a first supplement to Drugs and Driving: A Selected Bibliography (HS - 802 188), a bibliography of literature dealing with the relationship between drug use (other than alcohol alone) and highway safety. This supplement both updates the parent volume and expands coverage in certafn research areas related to the field of drugs and highway safety. In particular, 1i terature pertaining to drug usage patterns and drug analytical methodology has been included. A detailed description of the 1i terature scope and document selection process is provided. I I The bi bliography consists of four appendices, including a Topical Index, an Author Index, a Title Index, and Abstracts of nearly 400 i articles. A revised topical index was developed to improve user access to document abstracts. Within the topical index are cross-referenced lists of drugs by name and by usage. - ----&* 17. KO? Words 18. Dimhhtion Stotrmmnt Drugs, Drug Impaired Driving, Drug Avai labil ity is unlimited. Document Effect\, Drug Analytical Method01 ogy, may be re1eased to PIational Technical Drug Concentration-Effect Relation- 1 Information Service, Springfield, VA ships, Countermeasures 22161 for sale to public. -

Phenylmorpholines and Analogues Thereof Phenylmorpholine Und Analoge Davon Phenylmorpholines Et Analogues De Celles-Ci
(19) TZZ __T (11) EP 2 571 858 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: C07D 265/30 (2006.01) A61K 31/5375 (2006.01) 20.06.2018 Bulletin 2018/25 A61P 25/24 (2006.01) A61P 25/16 (2006.01) A61P 25/18 (2006.01) (21) Application number: 11723158.9 (86) International application number: (22) Date of filing: 20.05.2011 PCT/US2011/037361 (87) International publication number: WO 2011/146850 (24.11.2011 Gazette 2011/47) (54) PHENYLMORPHOLINES AND ANALOGUES THEREOF PHENYLMORPHOLINE UND ANALOGE DAVON PHENYLMORPHOLINES ET ANALOGUES DE CELLES-CI (84) Designated Contracting States: • DECKER, Ann Marie AL AT BE BG CH CY CZ DE DK EE ES FI FR GB Durham, North Carolina 27713 (US) GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO PL PT RO RS SE SI SK SM TR (74) Representative: Hoeger, Stellrecht & Partner Patentanwälte mbB (30) Priority: 21.05.2010 US 347259 P Uhlandstrasse 14c 70182 Stuttgart (DE) (43) Date of publication of application: 27.03.2013 Bulletin 2013/13 (56) References cited: WO-A1-2004/052372 WO-A1-2008/026046 (73) Proprietors: WO-A1-2008/087512 DE-B- 1 135 464 • Research Triangle Institute FR-A- 1 397 563 GB-A- 883 220 Research Triangle Park, North Carolina 27709 GB-A- 899 386 US-A1- 2005 267 096 (US) • United States of America, as represented by • R.A. GLENNON ET AL.: "Beta-Oxygenated The Secretary, Department of Health and Human Analogues of the 5-HT2A Serotonin Receptor Services Agonist Bethesda, Maryland 20892-7660 (US) 1-(4-Bromo-2,5-dimethoxyphenyl)-2-aminopro pane", JOURNAL OF MEDICINAL CHEMISTRY, (72) Inventors: vol. -

Phd Thesis Project: Pharmacological and Toxicological Investigations of New Psychoactive Substances, Supervised by Prof
PHARMACOLOGICAL AND TOXICOLOGICAL INVESTIGATIONS OF NEW PSYCHOACTIVE SUBSTANCES Inauguraldissertation zur Erlangung der Würde eines Doktors der Philosophie vorgelegt der Philosophisch-Naturwissenschaftlichen Fakultät der Universität Basel von Dino Lüthi aus Rüderswil, Bern Basel, 2018 Originaldokument gespeichert auf dem Dokumentenserver der Universität Basel edoc.unibas.ch Dieses Werk ist lizenziert unter einer Creative Commons Namensnennung-Nicht kommerziell 4.0 International Lizenz (https://creativecommons.org/licenses/by-nc-sa/4.0/deed.de). Genehmigt von der Philosophisch-Naturwissenschaftlichen Fakultät auf Antrag von Prof. Stephan Krähenbühl, Prof. Matthias E. Liechti und Prof. Anne Eckert. Basel, den 26.06.2018 Prof. Martin Spiess Dekan der Philosophisch- Naturwissenschaftlichen Fakultät PHARMACOLOGICAL AND TOXICOLOGICAL INVESTIGATIONS OF NEW PSYCHOACTIVE SUBSTANCES “An adult must make his own decision as to whether or not he should expose himself to a specific drug, be it available by prescription or proscribed by law, by measuring the potential good and bad with his own personal yardstick.” ― Alexander Shulgin, Pihkal: A Chemical Love Story. PREFACE This thesis is split into a pharmacology part and a toxicology part. The pharmacology part consists of investigations on the monoamine transporter and receptor interactions of traditional and newly emerged drugs, mainly stimulants and psychedelics; the toxicology part consists of investigations on mechanisms of hepatocellular toxicity of synthetic cathinones. All research described in this thesis has been published in peer-reviewed journals, and was performed between October 2014 and June 2018 in the Division of Clinical Pharmacology and Toxicology at the Department of Biomedicine of the University Hospital Basel and University of Basel, and partly at the pRED Roche Innovation Center Basel at F. -

Screening of 300 Drugs in Blood Utilizing Second Generation
Forensic Screening of 300 Drugs in Blood Utilizing Exactive Plus High-Resolution Accurate Mass Spectrometer and ExactFinder Software Kristine Van Natta, Marta Kozak, Xiang He Forensic Toxicology use Only Drugs analyzed Compound Compound Compound Atazanavir Efavirenz Pyrilamine Chlorpropamide Haloperidol Tolbutamide 1-(3-Chlorophenyl)piperazine Des(2-hydroxyethyl)opipramol Pentazocine Atenolol EMDP Quinidine Chlorprothixene Hydrocodone Tramadol 10-hydroxycarbazepine Desalkylflurazepam Perimetazine Atropine Ephedrine Quinine Cilazapril Hydromorphone Trazodone 5-(p-Methylphenyl)-5-phenylhydantoin Desipramine Phenacetin Benperidol Escitalopram Quinupramine Cinchonine Hydroquinine Triazolam 6-Acetylcodeine Desmethylcitalopram Phenazone Benzoylecgonine Esmolol Ranitidine Cinnarizine Hydroxychloroquine Trifluoperazine Bepridil Estazolam Reserpine 6-Monoacetylmorphine Desmethylcitalopram Phencyclidine Cisapride HydroxyItraconazole Trifluperidol Betaxolol Ethyl Loflazepate Risperidone 7(2,3dihydroxypropyl)Theophylline Desmethylclozapine Phenylbutazone Clenbuterol Hydroxyzine Triflupromazine Bezafibrate Ethylamphetamine Ritonavir 7-Aminoclonazepam Desmethyldoxepin Pholcodine Clobazam Ibogaine Trihexyphenidyl Biperiden Etifoxine Ropivacaine 7-Aminoflunitrazepam Desmethylmirtazapine Pimozide Clofibrate Imatinib Trimeprazine Bisoprolol Etodolac Rufinamide 9-hydroxy-risperidone Desmethylnefopam Pindolol Clomethiazole Imipramine Trimetazidine Bromazepam Felbamate Secobarbital Clomipramine Indalpine Trimethoprim Acepromazine Desmethyltramadol Pipamperone -

MEDICATION GUIDE Bupropion Hydrochloride Extended-Release
MEDICATION GUIDE BuPROPion Hydrochloride Extended-Release Tablets, USP (SR) (byoo-PROE-pee-on) Read this Medication Guide carefully before you start taking bupropion hydrochloride extended-release tablets (SR) and each time you get a refill. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or your treatment. If you have any questions about bupropion hydrochloride extended-release tablets (SR), ask your healthcare provider or pharmacist. IMPORTANT: Be sure to read the three sections of this Medication Guide. The first section is about the risk of suicidal thoughts and actions with antidepressant medicines; the second section is about the risk of changes in thinking and behavior, depression and suicidal thoughts or actions with medicines used to quit smoking; and the third section is entitled “What Other Important Information Should I Know About Bupropion Hydrochloride Extended-Release Tablets (SR)?” Antidepressant Medicines, Depression and Other Serious Mental Illnesses, and Suicidal Thoughts or Actions This section of the Medication Guide is only about the risk of suicidal thoughts and actions with antidepressant medicines. Talk to your healthcare provider or your family member’s healthcare provider about: • all risks and benefits of treatment with antidepressant medicines • all treatment choices for depression or other serious mental illness What is the most important information I should know about antidepressant medicines, depression and other serious mental illnesses, and suicidal thoughts or actions? 1. Antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, or young adults within the first few months of treatment.