Palindromic Rheumatism (PR), and the Drome (1)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Is Palindromic Rheumatism Amongst Children a Benign Disease? Yonatan Butbul-Aviel1,2,3, Yosef Uziel4,5, Nofar Hezkelo4, Riva Brik1,2,3,4 and Gil Amarilyo4,6*
Butbul-Aviel et al. Pediatric Rheumatology (2018) 16:12 https://doi.org/10.1186/s12969-018-0227-z RESEARCHARTICLE Open Access Is palindromic rheumatism amongst children a benign disease? Yonatan Butbul-Aviel1,2,3, Yosef Uziel4,5, Nofar Hezkelo4, Riva Brik1,2,3,4 and Gil Amarilyo4,6* Abstract Background: Palindromic rheumatism is an idiopathic, periodic arthritis characterized by multiple, transient, recurring episodes. Palindromic rheumatism is well-characterized in adults, but has never been reported in pediatric populations. The aim of this study was to characterize the clinical features and outcomes of a series of pediatric patients with palindromic rheumatism. Methods: We defined clinical criteria for palindromic rheumatism and reviewed all clinical visits in three Pediatric Rheumatology centers in Israel from 2006through 2015, to identify patients with the disease. We collected retrospective clinical and laboratory data on patients who fulfilled the criteria, and reviewed their medical records in order to determine the proportion of patients who had developed juvenile idiopathic arthritis. Results: Overall, 10 patients were identified. Their mean age at diagnosis was 8.3 ± 4.5 years and the average follow-up was 3.8 ± 2.7 years. The mean duration of attacks was 12.2 ± 8.4 days. The most frequently involved joints were knees. Patients tested positive for rheumatoid factor in 20% of cases. One patient developed polyarticular juvenile idiopathic arthritis after three years of follow-up, six patients (60%) continued to have attacks at their last follow-up and only three children (30%) achieved long-term remission. Conclusions: Progression to juvenile idiopathic arthritis is rare amongst children with palindromic rheumatism and most patients continued to have attacks at their last follow-up. -

Arthritis and Coeliac Disease
Ann Rheum Dis: first published as 10.1136/ard.44.9.592 on 1 September 1985. Downloaded from Annals of the Rheumatic Diseases 1985, 44, 592-598 Arthritis and coeliac disease J T BOURNE,' P KUMAR,2 E C HUSKISSON,' R MAGEED 3 D J UNSWORTH,3 AND J A WOJTULEWSKI4 From the Departments of 'Rheumatology and 2Gastroenterology, St Bartholomew's Hospital, West Smithfield, London ECIA 7BE; the 3Bone and Joint Research Unit, London Hospital Medical College, London El; and 4St Mary's Hospital, Eastbourne SUMMARY We report six patients with coeliac disease in whom arthritis was prominent at diagnosis and who improved with dietary therapy. Joint pain preceded diagnosis by up to three years in five patients and 15 years in one patient. Joints most commonly involved were lumbar spine, hips, and knees (four cases). In three cases there were no bowel symptoms. All were seronegative. X-rays were abnormal in two cases. HLA-type Al, B8, DR3 was present in five and B27 in two patients. Circulating immune complexes showed no consistent pattern before or after treatment. Coeliac disease was diagnosed in all patients by jejunal biopsy, and joint symptoms in all responded to a gluten-free diet. Gluten challenge (for up to three weeks) failed to provoke arthritis in three patients tested. In a separate study of 160 treated coeliac patients attending regular follow up no arthritis attributable to coeliac disease and no ankylosing was in a group spondylitis identified, though control of 100 patients with Crohn's disease thecopyright. expected incidence of seronegative polyarthritis (23%) and ankylosing spondylitis (5%) was found (p<0.01). -

Palindromic Rheumatism Or When Do You Decide to Treat an Asymptomatic Seropositive RA Patient? What Is This?
Palindromic Rheumatism or When do you decide to treat an asymptomatic seropositive RA patient? What Is This? • 11.15.15 • 56 yo man comes for 2nd opinion for bouts of severe large joint monoarthritis lasting 24 hours or longer. • Vague about duration “10-15 years.” Had wrist synovectomy 2005 after “trauma.” • Saw rheumatologist 2012: ACPA>500, RF 60. • Loss of shoulder motion in all planes. • At the conclusion of this presentation, the participant should be able to: – Appreciate the relationship of Palindromic Rheumatism (PR) and progression to RA – Understand the biology of intercritical PR – Define the utility of prevention strategies – Comprehend the yield of imaging in PR and how it informs PR pathophysiology • Should we try to prevent? How? Annual transition to RA is greater than 15% in which of the following ACPA+ pts? A. Arthralgia B. Arthralgia + Imaging + CRP C. Palindromic Rheumatism D. Asymptomatic Twin E. Interstitial Lung Disease Rheumatoid Arthritis Pathogenesis Tolerance broken-AutoAb appear Adaptive Immune Response Locus and Trigger? Systemic Nature? “Amplification” Synovial Targeting with variable kinetics? Innate vs Adaptive Immunity? Joint Targeting ACPA-IC deposit or are formed de novo in joint? Or something else? Tissue Injury Rheumatoid Arthritis Persistence of the Systemic Trigger? Systemic autoimmunity & inflammation T cells/B Cells Immune Complexes TNF, IL-6, GM-CSF No treatment shown to eliminate systemic process Where does MTX work? Joint Inflammation MF, FLS, Cartilage, Bone RA Centers in Synovium, Destroying All Around It? Why Is Palindromic Rheumatism Palindromic? Systemic inflammation Followed by resolution? e.g. like gout? Why does it resolve? Why does it stop resolving? Single Joint Inflammation Palindromic Rheumatism (PR) • How frequent is PR as an initial presentation of RA? • What is the mechanism of PR? • Is synovitis present during its intercritical phase? • What is the frequency of progression to RA in 5 years? Treatment? Is Palindromic Rheumatism a Common Presentation? Frequency relative to new onset RA is: A. -

Conditions Related to Inflammatory Arthritis
Conditions Related to Inflammatory Arthritis There are many conditions related to inflammatory arthritis. Some exhibit symptoms similar to those of inflammatory arthritis, some are autoimmune disorders that result from inflammatory arthritis, and some occur in conjunction with inflammatory arthritis. Related conditions are listed for information purposes only. • Adhesive capsulitis – also known as “frozen shoulder,” the connective tissue surrounding the joint becomes stiff and inflamed causing extreme pain and greatly restricting movement. • Adult onset Still’s disease – a form of arthritis characterized by high spiking fevers and a salmon- colored rash. Still’s disease is more common in children. • Caplan’s syndrome – an inflammation and scarring of the lungs in people with rheumatoid arthritis who have exposure to coal dust, as in a mine. • Celiac disease – an autoimmune disorder of the small intestine that causes malabsorption of nutrients and can eventually cause osteopenia or osteoporosis. • Dermatomyositis – a connective tissue disease characterized by inflammation of the muscles and the skin. The condition is believed to be caused either by viral infection or an autoimmune reaction. • Diabetic finger sclerosis – a complication of diabetes, causing a hardening of the skin and connective tissue in the fingers, thus causing stiffness. • Duchenne muscular dystrophy – one of the most prevalent types of muscular dystrophy, characterized by rapid muscle degeneration. • Dupuytren’s contracture – an abnormal thickening of tissues in the palm and fingers that can cause the fingers to curl. • Eosinophilic fasciitis (Shulman’s syndrome) – a condition in which the muscle tissue underneath the skin becomes swollen and thick. People with eosinophilic fasciitis have a buildup of eosinophils—a type of white blood cell—in the affected tissue. -

Hypersensitivity Reactions (Types I, II, III, IV)
Hypersensitivity Reactions (Types I, II, III, IV) April 15, 2009 Inflammatory response - local, eliminates antigen without extensively damaging the host’s tissue. Hypersensitivity - immune & inflammatory responses that are harmful to the host (von Pirquet, 1906) - Type I Produce effector molecules Capable of ingesting foreign Particles Association with parasite infection Modified from Abbas, Lichtman & Pillai, Table 19-1 Type I hypersensitivity response IgE VH V L Cε1 CL Binds to mast cell Normal serum level = 0.0003 mg/ml Binds Fc region of IgE Link Intracellular signal trans. Initiation of degranulation Larche et al. Nat. Rev. Immunol 6:761-771, 2006 Abbas, Lichtman & Pillai,19-8 Factors in the development of allergic diseases • Geographical distribution • Environmental factors - climate, air pollution, socioeconomic status • Genetic risk factors • “Hygiene hypothesis” – Older siblings, day care – Exposure to certain foods, farm animals – Exposure to antibiotics during infancy • Cytokine milieu Adapted from Bach, JF. N Engl J Med 347:911, 2002. Upham & Holt. Curr Opin Allergy Clin Immunol 5:167, 2005 Also: Papadopoulos and Kalobatsou. Curr Op Allergy Clin Immunol 7:91-95, 2007 IgE-mediated diseases in humans • Systemic (anaphylactic shock) •Asthma – Classification by immunopathological phenotype can be used to determine management strategies • Hay fever (allergic rhinitis) • Allergic conjunctivitis • Skin reactions • Food allergies Diseases in Humans (I) • Systemic anaphylaxis - potentially fatal - due to food ingestion (eggs, shellfish, -

Palindromic Rheumatism Clinical and Immunological Studies
Ann. rheum. Dis. (1971), 30, 375 Ann Rheum Dis: first published as 10.1136/ard.30.4.375 on 1 July 1971. Downloaded from Palindromic rheumatism Clinical and immunological studies M. H. WILLIAMS,* P. J. H. S. SHELDON,t G. TORRIGIANI, V. EISEN, AND S. MATTINGLY Departments of Rheumatology Research, Rheumatology and Physical Medicine, and Immunology, Middlesex Hospital Medical School and Middlesex Hospital, London Hench and Rosenberg (1944) described 34 patients tions were less frequent, and the finger pads were not with recurring episodes of arthritis and periarthritis involved. The duration of attacks was longer, usually lasting less than a week and named by them intervals between attacks tended to be shorter, and 'palindromio rheumatism'. The features they empha- there were often symptoms between attacks. The sized may be summarized as follows: erythrooyte sedimentation rate was increased, and (1) Recurrent attacks ofjoint pain and swelling at x rays andjoint biopsy showed changes characteristic variable and irregular intervals lasting a few of rheumatoid arthritis. Nevertheless, some authors hours or a few days. have expressed the view that palindromic rheuma- (2) Any joint affected but especially fingers, tism is a variant of episodic rheumatoid arthritis or a wrists, shoulders and knees. stage in its development (Ansell and Bywaters, 1959; (3) Para-artioular attacks and transient nodules. Robinson, 1963; Mattingly, 1966). (4) Good health: normal blood tests and x-rays. copyright. (5) Good prognosis-no effective treatment. Present investigations Several case reports have appeared since then, though few series of patients have been followed up In an attempt to differentiate palindromic rheuma- (Ward and Okihiro, 1959; Rotes Querol and Lience, tism from rheumatoid arthritis on an immunological 1959; Dames and Zuckner, 1961; Ansell and basis, leucocyte migration inhibition and anti-IgG Bywaters, 1959). -

Reactive Arthritis Information Booklet
Reactive arthritis Reactive arthritis information booklet Contents What is reactive arthritis? 4 Causes 5 Symptoms 6 Diagnosis 9 Treatment 10 Daily living 16 Diet 18 Complementary treatments 18 How will reactive arthritis affect my future? 19 Research and new developments 20 Glossary 20 We’re the 10 million people living with arthritis. We’re the carers, researchers, health professionals, friends and parents all united in Useful addresses 25 our ambition to ensure that one day, no one will have to live with Where can I find out more? 26 the pain, fatigue and isolation that arthritis causes. Talk to us 27 We understand that every day is different. We know that what works for one person may not help someone else. Our information is a collaboration of experiences, research and facts. We aim to give you everything you need to know about your condition, the treatments available and the many options you can try, so you can make the best and most informed choices for your lifestyle. We’re always happy to hear from you whether it’s with feedback on our information, to share your story, or just to find out more about the work of Versus Arthritis. Contact us at [email protected] Registered office: Versus Arthritis, Copeman House, St Mary’s Gate, Chesterfield S41 7TD Words shown in bold are explained in the glossary on p.20. Registered Charity England and Wales No. 207711, Scotland No. SC041156. Page 2 of 28 Page 3 of 28 Reactive arthritis information booklet What is reactive arthritis? However, some people find it lasts longer and can have random flare-ups years after they first get it. -

Rheumatoid Arthritis Initiating As Palindromic Rheumatism: a Distinct Clinical Phenotype? Raul Castellanos-Moreira , Sebastian C
Rheumatoid Arthritis Initiating as Palindromic Rheumatism: A Distinct Clinical Phenotype? Raul Castellanos-Moreira , Sebastian C. Rodriguez-Garcia , José A. Gómez-Puerta , Virginia Ruiz-Esquide , Oscar Camacho , Julio Ramírez , Andrea Cuervo , Rosa Morlà , Juan D. Cañete , Isabel Haro , and Raimon Sanmarti ABSTRACT. Objective. To analyze the prevalence of preexisting palindromic rheumatism (PR) in patients with established rheumatoid arthritis (RA) and to evaluate whether these patients have a distinctive clinical and serological phenotype. Methods. Cross-sectional study in patients with established RA. Preexisting PR was determined using a structured protocol and confirmed by retrospective review of medical records. Demographic, clinical, radiological, immunological, and therapeutic features were compared in patients with and without PR. Results. Included were 158 patients with established RA (78% female) with a mean disease duration since RA onset of 5.1 ± 2.7 years. Preexisting PR was recorded in 29 patients (18%). The median time from the onset of PR to progression to RA was 1.2 years. No between-group differences in demographic features, current disease activity, radiographic erosive disease, or disability were observed. Patients with PR had a higher prevalence of smoking (72% vs 40%). Positive rheumatoid factor, anticitrullinated peptide antibodies, and anticarbamylated protein antibodies were numerically higher in patients with PR. No differences in treatment were observed except for greater hydroxy- chloroquine (HCQ) use in patients with PR (38% vs 6%). Palindromic flares persisted in a significant proportion of patients during the RA course, including patients in clinical remission or receiving biological disease-modifying antirheumatic drugs. Conclusion. Eighteen percent of patients with RA had a history compatible with PR previous to RA onset. -

Joint Pain and Sjögren’S Syndrome
Joint Pain and Sjögren’s Syndrome Alan N. Baer, MD, FACP Alan N. Baer, MD, FACP Associate Professor of Medicine Division of Rheumatology Johns Hopkins University School of Medicine Director, Jerome Greene Sjogren's Syndrome Clinic 5200 Eastern Avenue Mason F. Lord Bldg. Center Tower Suite 4100, Room 413 Baltimore MD 21224 Phone (410) 550-1887 Fax (410) 550-6255 In 1930, Henrik Sjögren, a Swedish ophthalmologist, examined a woman with rheumatoid arthritis who had extreme dryness of her eyes and mouth and filamentary keratitis, an eye condition related to her lack of tears (1). He became fascinated by this unusual debilitating condition and subsequently evaluated 18 additional women with the same combination of findings. He described this new syndrome as “keratoconjunctivitis sicca” in his postdoctoral thesis. Thirteen of the 19 women had chronic inflammatory arthritis. We would now classify these 13 women as having secondary Sjögren’s syndrome (SS), occurring in the context of rheumatoid arthritis. However, joint pain constitutes one of the most common symptoms of the primary form of SS, defined as SS occurring in the absence of an underlying rheumatic disease. In a recent survey of SS patients belonging to the French Sjögren’s Syndrome Society (Association Française du Gougerot-Sjögren et des Syndromes Secs), 81% reported significant joint and muscle pain (2). In this article, the joint manifestations of primary SS will be reviewed. A few definitions are needed for the reader. Although the term “arthritis” was originally applied to conditions causing joint inflammation, it now includes disorders in which the joint has become damaged by degenerative, metabolic, or traumatic processes. -
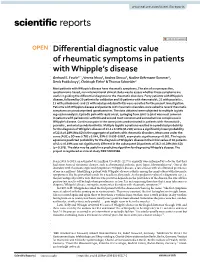
Differential Diagnostic Value of Rheumatic Symptoms in Patients
www.nature.com/scientificreports OPEN Diferential diagnostic value of rheumatic symptoms in patients with Whipple’s disease Gerhard E. Feurle1*, Verena Moos2, Andrea Stroux3, Nadine Gehrmann‑Sommer2, Denis Poddubnyy2, Christoph Fiehn4 & Thomas Schneider2 Most patients with Whipple’s disease have rheumatic symptoms. The aim of our prospective, questionnaire‑based, non‑interventional clinical study was to assess whether these symptoms are useful in guiding the diferential diagnosis to the rheumatic disorders. Forty patients with Whipple’s disease, followed by 20 patients for validation and 30 patients with rheumatoid‑, 21 with psoriatic‑, 15 with palindromic‑ and 25 with axial spondyloarthritis were recruited for the present investigation. Patients with Whipple’s disease and patients with rheumatic disorders were asked to record rheumatic symptoms on pseudonymized questionnaires. The data obtained were subjected to multiple logistic regression analysis. Episodic pain with rapid onset, springing from joint to joint was most common in patients with palindromic arthritis and second most common and somewhat less conspicuous in Whipple’s disease. Continuous pain in the same joints predominated in patients with rheumatoid‑, psoriatic‑, and axial spondyloarthritis. Multiple logistic equations resulted in a predicted probability for the diagnosis of Whipple’s disease of 43.4 ± 0.19% (M ± SD) versus a signifcantly lower probability of 23.8 ± 0.19% (M ± SD) in the aggregate of patients with rheumatic disorders. Mean area under the curve (AUC) ± SD was 0.781 ± 0.044, 95% CI 0.695–0.867, asymptotic signifcance p < 0.001. The logistic equations predicted probability for the diagnosis of Whipple’s disease in the initial series of 40 patients of 43.4 ± 0.19% was not signifcantly diferent in the subsequent 20 patients of 38.2 ± 0.28% (M ± SD) (p = 0.376). -

PALINDROMIC RHEUMATISM by STEPHEN MATTINGLY Department of Rheumatology and Physical Medicine, the Middlesex Hospital
Ann Rheum Dis: first published as 10.1136/ard.25.4.307 on 1 July 1966. Downloaded from Ann. rheum. Dis. (1966), 25, 307. PALINDROMIC RHEUMATISM BY STEPHEN MATTINGLY Department of Rheumatology and Physical Medicine, The Middlesex Hospital Palindromic rheumatism was first described by Painful non-pitting tender swellings an inch or more Hench and Rosenberg in 1941, and three years later a in diameter, and occasionally much larger, appeared detailed account of their 34 cases appeared in the over the forearms, back of wrist, or heel. Some- Archives of Internal Medicine (Hench and Rosen- times the finger tips became swollen and transient berg, 1944). A number of individual case reports intra-cutaneous or subcutaneous nodules were subsequently appeared in the literature (Ameen, observed on the hands, but usually disappeared 1954; Cain, 1944; Ferry, 1943; Ginsburg, 1948; within a few days. Grego and Harkins, 1944; Gryboski, 1948; Hopkins Patients suffering from palindromic rheumatism and Richmond, 1947; Lewitus, 1954; Mazer, 1942; remained well and did not lose weight. Attacks were Neligan, 1946; Paul and Logan, 1944; Paul and usually afebrile. Radiographs were normal in most Carr, 1945; Perl, 1947; Rotes Querol, 1956; Salo- cases or showed coincidental degenerative changes. mon, 1946; Scheinberg, 1947; Thompson, 1942; Laboratory investigations usually gave normal Parkes Weber, 1946; Wingfield, 1945; Wirtschafter, results, although there was sometimes a transient Williams, and Gaulden, 1955; Wolfson and Alter, rise in the erythrocyte sedimentation rate during an 1948; Wassmann, 1950; Zentner, 1953). However, attack, the white cell count might show a relative there have been few reports of series of patients with lymphocytosis, and the serum fatty acids were in- this syndrome (Ansell and Bywaters, 1959; Dames creased in some patients. -
Palindromic Rheumatism Information Booklet (PDF)
Palindromic rheumatism Palindromic rheumatism information booklet Contents Zoe’s story 4 What is palindromic rheumatism? 6 Symptoms 6 Causes 8 Diagnosis 10 How will palindromic rheumatism affect me? 11 Treatment 13 Managing symptoms 16 Living with palindromic rheumatism 20 Research and new developments 22 Glossary 22 We’re the 10 million people living with arthritis. We’re the carers, researchers, health professionals, friends and parents all united Useful addresses 25 in our ambition to ensure that one day, no one will have to live Where can I find out more? 26 with the pain, fatigue and isolation that arthritis causes. Talk to us 27 We understand that every day is different. We know that what works for one person may not help someone else. Our information is a collaboration of experiences, research and facts. We aim to give you everything you need to know about your condition, the treatments available and the many options you can try, so you can make the best and most informed choices for your lifestyle. We’re always happy to hear from you whether it’s with feedback on our information, to share your story, or just to find out more about the work of Versus Arthritis. Contact us at [email protected] Registered office: Versus Arthritis, Copeman House, St Mary’s Gate, Chesterfield S41 7TD Words shown in bold are explained in the glossary on p.22. Registered Charity England and Wales No. 207711, Scotland No. SC041156. Page 2 of 28 Page 3 of 28 When I went back after being on naproxen and hydroxychloroquine for four weeks, I felt the best I’d ever felt, and I thought perhaps he was going to discharge me.