Vitamin • a Vitamin Is an Organic Compound Required As a Nutrient in Tiny Amounts by an Organism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Product List 2
Zoic Healthcare Pvt.Ltd (A GMP , ISO 9001:2015 , WRG CERTIFICATIONS CERTIFIED COMPANY AN ISO 22000:2015 (FSMS) OFFICE : PLOT.No.195, INDL. AREA, SEC-82, JLPL MOHALI.(P.B) PLOT.No 236, INDL, AREA, PHASE-9, MOHALI. (P.B.) Email : [email protected] Mobile :78143 70634 NUTRACEUTICALS PRODUCTS 1 LIQUIDS (SYRUPS & SUSPENSIONS) PACKING 1 OMEGA-3 600MG + DHA 300MG + EPA 150MG + VITAMIN A 400 IU + VITAMIN D 200 IU + VITAMIN E 200 ML/ 100 ML 3MCG + VITAMIN C 50 MG SYRUP 2 CHOLECAICIFEROL 200IU + PYRIDOXINE HYDROCHIORIDE 1 MG + NIACINAMIDE 15MG + CYANOCOBALAMIN 1 MCG + ZINC 3 MG + B- CAROTENE DISPERSION 38 MG + MANGANESE 0.8MG + MOLYBDENUM 8MCG + SELENIUM 10 200 ML/ 100 ML MCG + LYSINE HYDROCHIORIDE 30MG + IODINE 50 MCG + BIOTIN 10 MCG + CHROMIUM 10 MCG + INOSITOL 10 MG SYP 3 VITAMIN A 2500 IU + CHOLRCALCIFEROL 100 IU + VITAMIN E 25 IU + THIAMINE HYDROCHLORIDE 0.75MG + RIBOFLAVIN SODIUM PHOSPHATE EQ. TO RIBOFLAVIN 0.75MG + PYIDOXINE HYDROCHLORIDE 0.5 MG + CYANOCOBALAMIN 0.5 MG + NICOTINAMIDE 7.5 MG + D-PANTHENOL 2.5 MG + ZINC SULPHATE 22.2 MG + POTASSIUM IODIDE 50 MCG + COPPER SULPHATE 100 200 ML/ 100 ML MCG + LYSINE HYDROCHLORIDE SYP 4 ZINC 5MG + VITAMIN A 1250 IU + LYCOPENE 2000 MCG + FOLIC ACID 1.5 MG + VITAMIN B6 1.5 MG + VITAMIN B2 1.3 MG + VITAMIN B1 1.1 MG + MANGANESE 0.8 MG + MECOBALAMIN 500 MCG + IODINE 90 MCG + CHROMIUM 70MCG EACH 200 ML/ 100 ML ML 5 CALCIUM CARBONATE 250 MG.(EQ TO ELEMENTAL IRON) + VITAMIN D3 125 I.U. + L-LYSINE 325 MG 200 ML/ 100 ML SUSPENSION 6 ANTIOXIDANTS, MULTIVITAMINS AND MULTI-MINERALS SYRUP 200 ML/ 100 -

Vitamin Project
Vitamin A Type Fat Soluable Names: Retinol, Rentinal, Retinoic Acid RDA 5-15 mg (eyes) System Deficiency Overdose Sources Interactions Integumentary *keratin based *Yellow skin! Fruit: ! Beta Caroteen = (hair, nails, skin) *weak cells! red & orange! precursor Vit A so = ! *abnormalities of mango! *break, bend skin! apricot! nails! *hair loss! apple! *brittle breaking *yellowing of skin! prune hair! *cracking of lips *rough skin Sensory *night blindness! *blurry vision! Beta Caroteen = *flash of light with *bloody nose can be converted very slow to Vit A in fatty recovery to tissue normal vision! *not see in the dark! *childhood blindness! *ear infections! *dry eye Nervous *headaches! Vegetable:! Protein status *insomnia! red & orange! affects Vit A *injure nervous Dk Leafy Greens! transport system or brain Yellow Veggies! Carrots! Digestive *keratinization - *low appetite! Corn Flakes! Healthy Liver goblet cells in *vomiting! Spinach! affects Vit A intestines = *anorexia! Broccoili! availability ⬇mucus = *weight loss! Sweet Potato! Tomato Juice! *diarrhea remove less Butternut Squash! nutrients from Turnip Greens! food = Avocado! malnutrition = weak muscles & weak immunity! *GI infection! *weakened teeth/ cavities Respiratory Zinc is needed to transport Vitamin A Type Fat Soluable Names: Retinol, Rentinal, Retinoic Acid RDA 5-15 mg (eyes) System Deficiency Overdose Sources Interactions Skeletal *slow bone *abnormalities of Dairy:! Zinc needed to growth! bone! mozz cheese! convert retinol to *slow break *fracture of bone! milk! retinal repair -

Dimethylglycine (DMG) Transported by the Circulatory System to Various Tissues in the DESCRIPTION Body
186/ DHEA (DEHYDROEPIANDROSTERONE) PDR FOR NUTRITIONAL SUPPLEMENTS Strous RD, Gibel A, Maayan R, et al. Hormonal response to ACTIONS AND PHARMACOLOGY dehydroepiandrosterone administration in schizophrenia: findings ACTIONS from a randomized, double-blind, placebo-controlled, crossover There are no known actions of supplemental DMG. study. J Clin Psychopharmacol.2008;28(4):456-459. Van Vollenhaven RF, Morabito LM, Engleman EG, et al. PHARMACOKINETICS Treatment of systemic lupus erythematosus with DMG is absorbed from the small intestine and from there dehydroepiandrosterone: 50 patients treated up to 12 months. J transported by the portal circulation to the liver. DMG is Rheumatol. 1998;25:285-289. metabolized in the liver to monomethylglycine or sarcosine which, in turn, is converted to glycine. Dimethylglycine Yen SS. Dehydroepiandrosterone sulfate and longevity: new dehydrogenase, a flavoprotein, is the enzyme that catalyzes clues for an old friend. Proc Natl Acad Sci USA. 200;98( 15):8167-8169. the oxidative demethylation of DMG to sarcosine. The methyl group produced in this reaction returns to the one carbon pool at the level of NIO_hydroxymethyl-tetrahydrofo- lic acid. DMG itself is formed from trimethylglycine or betaine. DMG that is not metabolized in the liver is Dimethylglycine (DMG) transported by the circulatory system to various tissues in the DESCRIPTION body. Dimethylglycine or DMG is a non-protein amino acid found naturally in animal and plant cells. DMG is produced in cells INDICATIONS AND USAGE It is too early to say whether DMG might eventually be as an intermediate in the metabolism of choline to glycine. indicated as an immune enhancer or in the management of There has been much confusion surrounding the history of autism. -

Pharmacology
STATE ESTABLISHMENT «DNIPROPETROVSK MEDICAL ACADEMY OF HEALTH MINISTRY OF UKRAINE» V.I. MAMCHUR, V.I. OPRYSHKO, А.А. NEFEDOV, A.E. LIEVYKH, E.V.KHOMIAK PHARMACOLOGY WORKBOOK FOR PRACTICAL CLASSES FOR FOREIGN STUDENTS STOMATOLOGY DEPARTMENT DNEPROPETROVSK - 2016 2 UDC: 378.180.6:61:615(075.5) Pharmacology. Workbook for practical classes for foreign stomatology students / V.Y. Mamchur, V.I. Opryshko, A.A. Nefedov. - Dnepropetrovsk, 2016. – 186 p. Reviewed by: N.I. Voloshchuk - MD, Professor of Pharmacology "Vinnitsa N.I. Pirogov National Medical University.‖ L.V. Savchenkova – Doctor of Medicine, Professor, Head of the Department of Clinical Pharmacology, State Establishment ―Lugansk state medical university‖ E.A. Podpletnyaya – Doctor of Pharmacy, Professor, Head of the Department of General and Clinical Pharmacy, State Establishment ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ Approved and recommended for publication by the CMC of State Establishment ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ (protocol №3 from 25.12.2012). The educational tutorial contains materials for practical classes and final module control on Pharmacology. The tutorial was prepared to improve self-learning of Pharmacology and optimization of practical classes. It contains questions for self-study for practical classes and final module control, prescription tasks, pharmacological terms that students must know in a particular topic, medical forms of main drugs, multiple choice questions (tests) for self- control, basic and additional references. This tutorial is also a student workbook that provides the entire scope of student’s work during Pharmacology course according to the credit-modular system. The tutorial was drawn up in accordance with the working program on Pharmacology approved by CMC of SE ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ on the basis of the standard program on Pharmacology for stomatology students of III - IV levels of accreditation in the specialties Stomatology – 7.110105, Kiev 2011. -

Quality Services with Smile…
Quality Services with Smile… We are among the notable names that are engaged in the Manufacturer, Exporter, Supplier, Distributor, Wholesaler, Trader & Importer of optimum quality Supplements, Nutraceuticals, Pharmaceuticals Medicines that are known for their optimum formulation. SYRUP SACHET ALU-ALU BLISTER AN FSSAI GMP ISO HALAL KOSHER CERTIFIED COMPANY Established in 2011 , Medicare Remedies Private Limited has secured a conspicuous position among the Exporter, Supplier, Distributor, Manufacturer, Wholesaler, Trader & Importer of utmost quality Nutraceuticals Dietary Supplement, Pharmaceutical Medicines and Cancer Drugs. Offered drugs are formulated in compliance with the FDA norms under strict supervision of qualified professionals as per WHO guideline. Known for their quick and long lasting results, these drugs & supplements are extremely demanded around the globe. For safe and hygienic formulation of offered drugs & supplements, we have established a spacious infrastructure, which is further segregated into several departments. These departments are equipped with advanced machines, which are upgraded in accordance to the current market needs. A well- maintained warehouse ensures effective storage of the offered products. Depending on our vast and trustworthy logistic partners, we deliver our products at the customer’s end within the stipulated time frame. Apart from this, our offered drugs are made available at reasonable market prices. Our revered mentors, Mr. Gaukaran Tripathi and Mr. Devidayal Tripathi, inspire the team with their rich industry experience and knowledge. Their emphasis on providing a smooth and pressure- free work environment for the employees has helped them give their best. Further, they have enabled the organization in gaining a strong foothold among the manufacturers and suppliers of superlative quality pharmaceutical medicines and cancer drugs. -
Conditions Template
Learn the Art of Healing with Plant Medicine [email protected] 1-888-WLD-ROSE (953-7673) wildrosecollege.com Conditions: Angina Pectoris This condition, which can feel similar to a heart attack, lasts only a few minutes. It is characterized by chest pains that may be felt as a mild tightness or pressure, or may be so extreme as to produce intense aching. Sometimes pain radiates from the chest to the shoulder and down the left arm. These pains are a result of the heart tissue not receiving enough oxygen (due to a diminished blood supply from the coronary arteries) and are often quickly relieved by rest. This is known as myocardial ischemia and is generally caused by arteriosclerosis of the coronary arteries. (Refer to section on Arteriosclerosis) For a first-time sufferer, the distinct resemblance to a heart attack will generally result in great anxiety. Once aware of the condition, the individual can easily deal with it, lessening the overall anxiety experienced. Recommended Action The person should immediately attempt to relax both mentally and physically. This will help put an end to the pain as the relaxed heart muscle will cause the blood vessels to dilate (open), decreasing the need for oxygen while increasing the heart’s ability to pump blood and deliver oxygen. Adopting a diet low in sodium and high in potassium and adding fresh fruits and vegetables to the diet are essential for long-term relief. Muscle tone and blood vessel flexibility are improved through the use of vitamin E and lecithin, while the entire circulatory system is strengthened by the use of Vitamin C and natural B complex vitamins. -

Vitamins, Minerals, Supplements.Cdr
3rd party manufacturing PRODUCT LIST Category : MULTI-VITAMINS, MULTI-MINERALS, IRON SUPPLEMENTS & CALCIUM SUPPLEMENTS MULTI-VITAMINS,MULTI-MINERALS & IRON SUPPLEMENTS SR.NO. COMPOSTION DRUG/FOOD DOSAGE PACKING 1 Beta Carotene 10% Dispersion 10Mg -Eq. To Vitamin A 5000 I.U.Vitamin E (As Acetate) 25 I.U.+ Vitamin C (As Coated) 100Mg+ Copper Sulphate Eq. To Elemental Copper 1.5Mg+ Manganese Sulphate Eq. To Elemental Manganese 1.5Mg+ Zinc Sulphate Eq. To Elemental Zinc 7.5Mg +Sodium Selenite Eq. To Elemental Selenium 150Mcg FOOD CAPSULE 10X10 ALU ALU/BLISTER 2 Antioxidants With Multivitamins & Minerals FOOD CAPSULE 10X10 ALU ALU/BLISTER 3 Antioxidants+Vitamins & Minerals FOOD SYP/SUSP 200 ML/100 ML M.CAR. 4 B-Comlex SyrupEach 10 Ml Contains:-Vitamin B1 2Mg+V itaminB2 2Mg+Vitamin B6 1Mg+Vitamin B12 0.5 Mcg+ Niacinamide10Mg+Protein 5 % 500Mg+Zinc Sulphate 5Mg+L-Lysin Hcl 15Mg+Folic Acid 1.5Mg +Colour: Caramel+Flavour: Strawberry FOOD SYRUP 200 ML/100 ML/M. CAR. 5 B-Complex With L-Lysine FOOD SYP/SUSP 200 ML/100 ML M.CAR. 6 B-Complex With Multivitamin And Zinc FOOD SYP/SUSP 200 ML/100 ML M.CAR. 7 Bioactive Collagen Peptide FOOD SACHET 10 GM 10 SACHETS CAR. 8 Bioactive Collagen Peptide+Calcitriol & Calcium Citrate FOOD SACHET12.5 GM 10 SACHETS CAR. 9 Biotin+ Amino Acids+ Vitamins+ Minerals & Natural Extracts FOOD TABLET 10X10 ALU-ALU 10 Biotin+ Minerals And Amino Acid FOOD CAPSULE 10X10 ALU ALU/BLISTER 11 Boswellia Extract 8.1% 50Mg+Collagen Peptide Type 2 50Mg+Diacerein 50Mg+Glucosamine Sulphate Potassium Chloride 750Mg+Hyaluronic Acid 5Mg+ Methyl Sulphonyl Methane 200Mg Tablets FOOD TABLET 10x10 ALU-ALU 12 Calcium Citrate 1 Gm+Vit. -

MINERALS – the SPARKS of LIFE! Karen Urbanek CEO Holistic Health Educators
MINERALS – THE SPARKS OF LIFE! Karen Urbanek CEO Holistic Health Educators Please enjoy my Mineral Chart for your personal use or with your clients. For MUCH more information on how the cells of our bodies use minerals and vitamins, please check out the courses created to put YOU back in charge of your amazing health! I have worked with THOUSANDS of individuals helping them eliminate dis-ease, gain energy, reverse cancers, lose weight and rebuild their health and all I have learned I share in my programs. Visit www.HolisticHealthEducators.com to enroll in our 10-Step Program, become EMPOWERED in my seven hour EMPOWERED series, check out the BLOG, enjoy my free Cell-Talk Series and sign up for weekly emails that are loaded with great info! (AND recipes!) – YOUR CELL HEALTH MATTERS! All the best – Karen We have listed some trace and macro minerals below. If your body requires over 100 mg of a particular element, that element is called a Macro Mineral. If you require less than 100 mg, it’s considered a Trace Element. Both Macro and Trace Minerals are important for good and lasting health. The body needs far greater amounts of Macro Minerals than Trace Minerals, but both types of minerals are needed daily for optimum health, energy, and the ability and capacity for the body to repair itself and maintain new health! Mineral & Food Sources Why We Need It Herb Sources Daily Need Calcium Sources rich in calcium: dark leafy 99% of the body’s calcium is in the bones and Valerian root, MACRO green vegetables, kale, kelp, teeth. -

Nambudripad's Allergy Elimination Technique (Naet)
NAMBUDRIPAD’S ALLERGY ELIMINATION TECHNIQUE (NAET) Kevin L. Terry D.C. Puyallup Chiropractic Clinic (253) 845-0543 111 Stewart Avenue East Puyallup, WA 98372 BASIC TREATMENTS What are the basic treatments, and why should you treat them? Almost every one asks these questions. The basic treatments include treatment for the essential nutrients, essential vitamins, essential minerals, those that are needed for the normal physical, physiological and emotional functions of the human body. These nutrients are absorbed from the regular food we are eating every day. When anyone is allergic to the food or the nutrients in the food, they cannot absorb or assimilate these nutrients. The nutrients are absolutely necessary for the normal body functions, for growth and development, to repair the wear and tear in the body, to fight infections and diseases, to prevent invasion of foreign energies or bacteria entering the body and for proper maintenance of the functions. When someone is allergic to eggs, milk, fruits, vegetables, or grains, etc., they are also allergic to the nutrients contained in them like protein, calcium, vitamin C, sugar, B-Complex, etc. Allergy to proteins (eggs) can make you more susceptible to frequent colds, flu-like symptoms, bronchitis, sinusitis, pneumonia, asthma, skin problems, hair problems like poor growth, falling hair, premature gray, breathing problems, digestive disorders, muscle and joint pains, fatigue and weakness of the muscles, poor blood circulation, high cholesterol, high blood pressure, water retention in the tissues, mental disorders like manic disorders, poor memory, poor concentration, headaches, sleep problems, irritability, hyperactivity and many other infections. Allergy to each nutrient like calcium (milk), vitamin C, B-complex, etc., prevents normal body functions and causes damage to the body tissue. -

Third Party Manufacturing LIST COMPANY PROFILE
Working For Quality Medicine at affordable price Third party Manufacturing LIST COMPANY PROFILE Glimpse of METAFORE HEALTHCARE Pvt Ltd. “Work hard in silence; let the quality of your work make the noise.” Abided by the norms of extending uncompromised quality products, we at Metafore Healthcare, have raised the standards of the industry time and again. Direct from Director METAFORE HEALTHCARE establish as a result of the dedicated efforts put in by a team of committed professional with strong determination to serve the people, We Fight to become a knowledge driven with Quality products at affordable price MEDICINE for patient. Welcome to Metafore Healcare Pvt Ltd ! Making specialty medicines accessible to all. We manufacture and market affordable medicines that comply with global standards and strive to achieve market leadership in domestic and international markets. We have been assessed and found to be in compliance with the requirements of the standard GMP (Good Manufacturing practices) ISO 9001:2015, GMP and CE Certified Metafore Healthcare Pvt. Ltd.'s rapid growth is a result of quality services, network, and time bound deliverables, and most importantly transparency with the clients. Our Core Principles Ethical Conduct Honesty and integrity lie at the core of Metafore Healthcare business values. Our operational review Committee, which reports to the Company Board of Directors, oversees all ethical issues. We expect all Metafore employees to meet the highest of ethical standards in business conduct, and we entrust each and every member of our team to endorse and abide by our Code of Conduct. Employment Practices We value our employees as our most important asset, and we aim to be recognized as the market leader in recruiting and retaining the most distinguished of individuals. -

FDAV Consumer, June 1980
koto., zo. i^/s June 1980 Blue Language And The Jakewalk Blues %: Patricia Roberts Harris Secretary, U.S. Department of ':-! Health and Human Services I..-. ^ DIVISION Julius B. Richmond, M.I). GOVERNMENT PUBLICATIONS" jrrcr.Y Assistant Secretary for Health JU.S. DEPCJITCr.Y iDO0C:.'.£NT. VOL. 14 NO. t D-295 June 1980 Jere E. Goyan, Ph.D. Commissioner of Food and Drugs Blue Language and the Jakewalk Blues 6 Wayne L. Pines was a drink also Associate Commissioner Jake popular illegal during prohibition. It for Public Affairs caused paralysis. Our writer recalls what happened to his jake-drinking father and reconstructs how FDA helped solve the jake contamination case. Roger W. Miller/Editor Harold C. Hopkins/Editorial Director Letter to a Young Saccharin User 12 Commissioner Jere E. Goyan responds to a young Jesse R. Nichols/Art Director letterwriter who drinks diet soda and worries about the con sequences. FDA Consumer (436210) is the official magazine of the Food and Drug Administration, Rock- A Peek Into America's Shopping Bag 14 ville, Md. 20857, and is monthly, ex published Food-buying habits the American public are constantly cept for combined issues for July-August and of Here's the latest on a those habits. December-January. Subscriptions should be changing. survey of ordered from and made payable to SUPERIN TENDENT OF DOCUMENTS, Government Keeping an Eye on Glaucoma 16 Printing Office, Washington, D.C. 20402, at A silent disease of the eye, glaucoma can ruin the optic $12.00 a year ($15.00 foreign mailing). Second- nerve cause blindness. -
Gist Life Pharmaceuticals
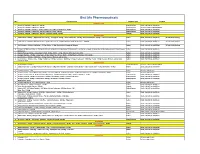
Gist Life Pharmaceuticals S.NO FORMULATIONS PRODUCT TYPE PACKING UROLOGY (UTIS) 1 Cranberry - 300 Mg + D-Mannose - 600 Mg Tablet/Capsule 10x10, 10x1x10 Alu-Alu/Blister 2 Cranberry - 180 Mg + D-Mannose - 300 Mg Sachet/Capsule 10 Sachet, 10x1x10 Alu-Alu/Blister 3 Cranberry - 300 Mg + Vitamin C - 40 Mg + Vitamin 135 - 5 Mg + L-Methionine - 22 Mg Tablet/Capsule 10x10, 10x1x10 Alu-Alu/Blister 4 Cranberry - 200 Mg + D-Mannose - 200 Mg + Hibiscus Extract - 100 Mg Tablet/Capsule 10x10, 10x1x10 Alu-Alu/Blister 5 Cranberry - 200 Mg + D-Mannose - 300 Mg + Potassium Citrate - 978 Mg Capsule 10x10, 10x1x10 Alu-Alu/Blister DERMATOLOGY 1 L-Glutathione - 100 Mg + Alpha Lipoic Acid - 50 Mg + Pycnogenol - 30 Mg + Green Tea Extract - 100 Mg + Grape Seed Extract - 50 Mg + Vitamins & Amino Acids Tablet 10x10, 10x1x10 Alu-Alu/Blister, 30 Tab. Bottle Packing 2 L-Glutathione - 500 Mg + Alpha Lipoic Acid - 50 Mg + Grape Seed - 50 Mg & Vitamins Bottle B: Vitamin C - 1000 Mg Tablet 10x10, 10x1x10 Alu-Alu/Blister, 30 Tab. Bottle Packing 3 Saw Palmetto - 100 Mg + Nettle Leaf - 50 Mg + Biotin - 10 Mg, Amino Acids, Vitamins & Minerals Tablet 10x10, 10x1x10 Alu-Alu/Blister, 30 Tab. Bottle Packing 4 Collagen- 50 Mg, Saw Palmetto-160 Mg, Nettle Leaf-50 Mg, Paba-50 Mg, Biotin-10 Mg, Green Tea-50 Mg, Green Apple-50 Mg + Msm-50 Mg, Ginkgo Biloba-I 0 Mg, Vitamins Tablet 10x10, 10x1x10 Alu-Alu/Blister & Minerals. 5 Soya lsoflavones - 50 Mg + Grape Seed Extract - 20 Mg + Biotin - 10 Mg, Vitamins, Minerals, Amino Acids Tablet 10x10, 10x1x10 Alu-Alu/Blister 6 Collagen Peptides - 175 Mg + Grape Seed - 10 Mg + Green Tea - 10 Mg + Biotin - 10 Mg Vitamins, Minerals, Amino Acids Tablet 10x10, 10x1x10 Alu-Alu/Blister 7 Saw Palmetto - 100 Mg + Nettle Leaf - 50 Mg, Vitamins, Minerals, Amino Acids Tablet 10x10, 10x1x10 Alu-Alu/Blister 8 Saw Palmetto - 100 Mg + Paba - 50 Mg + Nettle Leaf - 50 Mg + Lycopene - 4000 Mcg + Omega-3 Fatty Acid - 1000 Mcg + Biotin - 10 Mg Vitamins, Minerals.