Standard Treatment Guidelines and Essential Drugs List
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of New Drugs Approved in India from 1991 to 2000
LIST OF NEW DRUGS APPROVED IN INDIA FROM 1991 TO 2000 S. No Name of Drug Pharmacological action/ Date of Indication Approval 1 Ciprofloxacin 0.3% w/v Eye Indicated in the treatment of February-1991 Drops/Eye Ointment/Ear Drop external ocular infection of the eye. 2 Diclofenac Sodium 1gm Gel March-1991 3 i)Cefaclor Monohydrate Antibiotic- In respiratory April-1991 250mg/500mg Capsule. infections, ENT infection, UT ii)Cefaclor Monohydrate infections, Skin and skin 125mg/5ml & 250mg/5ml structure infections. Suspension. iii)Cefaclor Monohydrate 100mg/ml Drops. iv)Cefaclor 187mg/5ml Suspension (For paediatric use). 4 Sheep Pox Vaccine (For April-1991 Veterinary) 5 Omeprazole 10mg/20mg Short term treatment of April-1991 Enteric Coated Granules duodenal ulcer, gastric ulcer, Capsule reflux oesophagitis, management of Zollinger- Ellison syndrome. 6 i)Nefopam Hydrochloride Non narcotic analgesic- Acute April-1991 30mg Tablet. and chronic pain, including ii)Nefopam Hydrochloride post-operative pain, dental 20mg/ml Injection. pain, musculo-skeletal pain, acute traumatic pain and cancer pain. 7 Buparvaquone 5% w/v Indicated in the treatment of April-1991 Solution for Injection (For bovine theileriosis. Veterinary) 8 i)Kitotifen Fumerate 1mg Anti asthmatic drug- Indicated May-1991 Tablet in prophylactic treatment of ii)Kitotifen Fumerate Syrup bronchial asthma, symptomatic iii)Ketotifen Fumerate Nasal improvement of allergic Drops conditions including rhinitis and conjunctivitis. 9 i)Pefloxacin Mesylate Antibacterial- In the treatment May-1991 Dihydrate 400mg Film Coated of severe infection in adults Tablet caused by sensitive ii)Pefloxacin Mesylate microorganism (gram -ve Dihydrate 400mg/5ml Injection pathogens and staphylococci). iii)Pefloxacin Mesylate Dihydrate 400mg I.V Bottles of 100ml/200ml 10 Ofloxacin 100mg/50ml & Indicated in RTI, UTI, May-1991 200mg/100ml vial Infusion gynaecological infection, skin/soft lesion infection. -
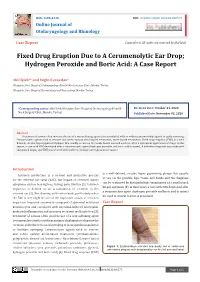
Fixed Drug Eruption Due to a Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: a Case Report
ISSN: 2688-8238 DOI: 10.33552/OJOR.2020.04.000577 Online Journal of Otolaryngology and Rhinology Case Report Copyright © All rights are reserved by Akif İşlek Fixed Drug Eruption Due to A Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: A Case Report Akif İşlek1* and Engin Karaaslan2 1Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey 2Nusaybin State Hospital, Dermatology and Venereology, Mardin, Turkey *Corresponding author: Received Date: October 24, 2020 Published Date: November 03, 2020 Akif İşlek, Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey. Abstract Treatment of earwax often involves the use of a wax softening agent (cerumenolytic) with or without antimicrobial agents to easily removing. Cerumenolytic agents used to remove and soften earwax areoil-based treatments, water-based treatments. Fixed drug eruption (FDE) is a well- defined, circular, hyperpigmented plaque that usually occurs on the trunk, hands mucosal surfaces, after a systemical application of drugs. In this report, a case with FDE developed after a cerumenolytic agent (hydrogen peroxide and boric acid in water). A definitive diagnosis was made with skin punch biopsy and FDE was treated with oral levocetirizine and topical mometasone. Introduction is a well-defined, circular, hyper pigmenting plaque that usually Cerumen production is a normal and protective process occurs on the genitals, lips, trunk, and hands and the diagnosis for the external ear canal (EAC), but impact of cerumen causes can be confirmed by histopathologic examination of a small punch symptoms such as hearing loss, itching, pain, tinnitus [1]. Cerumen biopsy specimen [5]. In this report, a case with FDE developed after impaction is defined as an accumulation of cerumen in the a cerumenolytic agent (hydrogen peroxide and boric acid in water) external ear [2]. -

Adansonia Digitata L
Veterinary World, EISSN: 2231-0916 RESEARCH ARTICLE Available at www.veterinaryworld.org/Vol.7/July-2014/10.pdf Open Access Antidiarrhoeal effect of the crude methanol extract of the dried fruit of Adansonia digitata L. (Malvaceae) Mohammed Musa Suleiman1111 , Mohammed Mamman , Ibrahim Hassan , Shamsu Garba , Mohammed Umaru Kawu21 and Patricia Ishaku Kobo 1. Department of Pharmacology and Toxicology, Faculty of Veterinary Medicine, Ahmadu Bello University, Zaria, Nigeria; 2. Department of Physiology, Faculty of Veterinary Medicine, Ahmadu Bello University, Zaria, Nigeria. Corresponding author: Mohammed Musa Suleiman, email:[email protected] MM: [email protected], IH: [email protected], SG: [email protected], MUK: [email protected], PIK: [email protected] Received:06-04-2014, Revised: 12-06-2014, Accepted: 14-06-2014, Published online: 19-07-2014 doi: 10.14202/vetworld.2014.495-500 How to cite this article: Suleiman MM, Mamman M, Hassan I, Garba S, Kawu MUand Kobo PI (2014) Antidiarrhoeal effect of the crude methanol extract of the dried fruit ofAdansonia digitata L. (Malvaceae), Veterinary World 7(7): 495-500. Abstract Aim: The study was designed to evaluate the antidiarrhoeal property of the methanol extract of the fruit of Adansonia digitata using laboratory animal models. Materials and Methods : The acute oral toxicity (LD50 ) of the extract was determined in mice, while the antidiarrhoeal effect of different doses of the extract was evaluated in both mice and rats. The effect of the extract at doses of 300, 700 and 1000 mg/kg were tested against intestinal transit time, magnesium sulphate-induced gastrointestinal motility test and castor oil- induced diarrhoea in mice. -

In Vivo Evaluation of Antidiarrhoeal Activity of the Leaves of Azima Tetracantha Linn
Vol.5(8), pp. 140-144, December, 2013 DOI: 10.5897/IJNAM2013.0152 International Journal of Nutrition and ISSN 2141-2340 ©2013 Academic Journals http://www.academicjournals.org/IJNAM Metabolism Full Length Research Paper In vivo evaluation of antidiarrhoeal activity of the leaves of Azima tetracantha Linn V. Hazeena Begum*, M. Dhanalakshmi and P. Muthukumaran Department of Siddha Medicine, Faculty of Science, Tamil University, Vakaiyur, Thanjavur 613 010, Tamilnadu, India. Accepted 3 October, 2013 The aqueous crude extract of the leaves of Azima tetracantha was studied for its phytochemical constituents and antidiarrhoeal activity using castor oil-induced diarrhoea and castor oil-induced enteropooling in rats. The phytochemical studies of the aqueous extract revealed the presence of alkaloids, flavonoids, tannins and saponins. The extract showed significant (p < 0.001) protection against castor oil-induced diarrhoea and castor oil-induced enteropooling at (100 mg/kg). The presence of some of the phytochemicals in the root extract may be responsible for the observed effects, and also the basis for its use in traditional medicine as antidiarrhoeal drug. Key words: Azima tetracantha, enteropooling, anti-diarrhoeal. INTRODUCTION Diarrhoea is characterized by increased frequency of powerful diuretic given in rheumatism, dropsy, dyspepsia bowel movement, wet stool and abdominal pain and chronic diarrhoea and as a stimulant tonic after (Ezekwesili et al., 2004). It is a leading cause of confinement (Nadkarni, 1976). A. tetracantha as efficient malnutrition and death among children in the developing acute phase anti-inflammatory drug is traditionally used countries of the world today (Victoria et al., 2000). Many by Indian medical practitioners (Ismail et al., 1997). -

Priority for Everyone, and Even More So for Those with Chronic Illnesses
Mouth Care: Patient/Caregiver Training Hospice of Cincinnati Mouth Care is a high priority for everyone, and even more so for those with chronic illnesses. Proper mouth care has many benefits including: 1. Increasing appetite 2. Maintaining comfort 3. Clearer speech 4. Easier swallowing 5. Preventing sores and infection. General tips: Mouth care should be performed a minimum of twice daily and more frequently for dry mouth, if breathing through the mouth, or if you are not eating. Mouth care should always be performed after using an inhaler/nebulizer to prevent thrush. Thrush is slightly raised white patches or a rash typically seen on the tongue or inner cheeks. There may be pain with swallowing. Contact your hospice nurse immediately if you suspect thrush. Dentures may no longer fit well. You may consider using them only when eating or when visiting with friends and family. Questions or concerns? Call a hospice nurse at 513-891-7700. Training: Mouth Care. ©2017 Hospice of Cincinnati Hospice of Cincinnati Relieving dry mouth: 1. Increase frequency of mouth care. 2. Encourage sucking on candy, ice chips, popsicles or taking small sips of water to increase saliva. 3. Use of a mouthwash can increase dryness. Talk to your nurse about a proper mouth moisturizer/artificial saliva product. For those with difficulty swallowing: • Raise the head of the bed and support the head with pillows, turn head to one side. • Cover the upper body with a towel to keep the area clean and dry. • Remove dentures prior to mouth care and brush separately. • Use a toothette, which is a sponge-tipped oral swab, to clean the mouth and teeth using a small amount of toothpaste. -

Treatment of Equine Gastric Impaction by Gastrotomy R
EQUINE VETERINARY EDUCATION / AE / april 2011 169 Case Reporteve_165 169..173 Treatment of equine gastric impaction by gastrotomy R. A. Parker*, E. D. Barr† and P. M. Dixon Dick Vet Equine Hospital, University of Edinburgh, Easter Bush Veterinary Centre, Midlothian; and †Bell Equine Veterinary Clinic, Mereworth, UK. Keywords: horse; colic; gastric impaction; gastrotomy Summary Edinburgh with a deep traumatic shoulder wound of 24 h duration. Examination showed a mildly contaminated, A 6-year-old Warmblood gelding was referred for treatment of 15 cm long wound over the cranial aspect of the left a traumatic shoulder wound and while hospitalised developed scapula that transected the brachiocephalicus muscle a large gastric impaction which was unresponsive to and extended to the jugular groove. The horse was sound medical management. Gastrotomy as a treatment for gastric at the walk and ultrasonography showed no abnormalities impactions is rarely attempted in adult horses due to the of the bicipital bursa. limited surgical access to the stomach. This report describes The wound was debrided and lavaged under standing the successful surgical treatment of the impaction by sedation and partially closed with 2 layers of 3 metric gastrotomy and management of the post operative polyglactin 910 (Vicryl)1 sutures in the musculature and complications encountered. simple interrupted polypropylene (Prolene)1 skin sutures, leaving some ventral wound drainage. Sodium benzyl Introduction penicillin/Crystapen)2 (6 g i.v. q. 8 h), gentamicin (Gentaject)3 (6.6 mg/kg bwt i.v. q. 24 h), flunixin 4 Gastric impactions are rare in horses but, when meglumine (Flunixin) (1.1 mg/kg bwt i.v. -

OVESTIN PESSARY (0.5Mg)
NEW ZEALAND DATA SHEET 1. OVESTIN PESSARY (0.5mg) 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each pessary contains 0.5 mg Estriol. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Pessary 0.5 mg - white, torpedo formed pessary. One pessary (2.5 g weight) contains 0.5 mg oestriol. Length 26.5 mm; largest diameter 14 mm. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Atrophy of the lower urogenital tract related to oestrogen deficiency, notably • for the treatment of vaginal complaints such as dyspareunia, dryness and itching. • for the prevention of recurrent infections of the vagina and lower urinary tract. • in the management of micturition complaints (such as frequency and dysuria) and mild urinary incontinence. Pre- and postoperative therapy in postmenopausal women undergoing vaginal surgery. A diagnostic aid in case of a doubtful atrophic cervical smear. 4.2 Dose and method of administration Dosage OVESTIN is an oestrogen-only product that may be given to women with or without a uterus. Atrophy of the lower urogenital tract 1 pessary per day for the first weeks, followed by a gradual reduction, based on relief of symptoms, until a maintenance dosage (e.g. 1 pessary twice a week) is reached. Pre- and post-operative therapy in postmenopausal women undergoing vaginal surgery 1 pessary per day in the 2 weeks before surgery; 1 pessary twice a week in the 2 weeks after surgery. A diagnostic aid in case of a doubtful atrophic cervical smear 1 pessary on alternate days in the week before taking the next smear. Administration OVESTIN pessaries should be inserted intravaginally before retiring at night. -

Hydrogen Peroxide, and This Is the Same Substance That Can Be Purchased in a 32-Ounce Plastic Bottle at Walmart, for 88 Cents, Or at Walgreens for Under a $1.00
An At-Home Treatment That Can Cure Any Virus, Including Coronavirus Originally Conceptualized, circa 1990, by Charles Farr, MD Subsequently Researched and Prescribed by Frank Shallenberger, MD Current Protocol Created by Thomas Levy, MD, JD Although COVID-19, aka coronavirus, is deadly in some select cases, and it can spread rapidly, there is a simple, very inexpensive, and highly effective treatment that can treat and rapidly resolve coronavirus and virtually any other respiratory virus. While different individuals can be expected to have variable degrees of positive response, this intervention can be anticipated to eliminate eventual fatal disease outcomes in all but the most advanced cases. As I hope you will eventually experience, the treatment works for all acute viral infections, and especially well for flu viruses of any variety. In fact, although we are constantly conditioned to not believe in anything “too good to be true,” you will never have to worry about getting a cold or the flu again because you can cure it on your own. The key ingredient in this treatment is common household 3% hydrogen peroxide, and this is the same substance that can be purchased in a 32-ounce plastic bottle at Walmart, for 88 cents, or at Walgreens for under a $1.00. Perhaps you have never heard of hydrogen peroxide therapy, but since the treatment was first championed by Dr. Charles Farr in about 1990, thousands of doctors have used this therapy for decades to conquer infections in many thousands of patients throughout the world. How and Why Hydrogen Peroxide Works Because hydrogen peroxide consists of a water molecule (H2O) with an extra oxygen atom (H2O2), it is this extra oxygen atom that makes it so deadly for viruses. -

UK Clinical Guideline for Best Practice in the Use of Vaginal Pessaries for Pelvic Organ Prolapse
UK Clinical Guideline for best practice in the use of vaginal pessaries for pelvic organ prolapse March 2021 Developed by members of the UK Clinical Guideline Group for the use of pessaries in vaginal prolapse representing: the United Kingdom Continence Society (UKCS); the Pelvic Obstetric and Gynaecological Physiotherapy (POGP); the British Society of Urogynaecology (BSUG); the Association for Continence Advice (ACA); the Scottish Pelvic Floor Network (SPFN); The Pelvic Floor Society (TPFS); the Royal College of Obstetricians and Gynaecologists (RCOG); the Royal College of Nursing (RCN); and pessary users. Funded by grants awarded by UKCS and the Chartered Society of Physiotherapy (CSP). This guideline was completed in December 2020, and following stakeholder review, has been given official endorsement and approval by: • British Association of Urological Nurses (BAUN) • International Urogynecological Association (IUGA) • Pelvic Obstetric and Gynaecological Physiotherapy (POGP) • Scottish Pelvic Floor Network (SPFN) • The Association of Continence Advice (ACA) • The British Society of Urogynaecology (BSUG) • The Pelvic Floor Society (TPFS) • The Royal College of Nursing (RCN) • The Royal College of Obstetricians and Gynaecologists (RCOG) • The United Kingdom Continence Society (UKCS) Review This guideline will be due for full review in 2024. All comments received on the POGP and UKCS websites or submitted here: [email protected] will be included in the review process. 2 Table of Contents Table of Contents ................................................................................................................................ -

Pessary for Management of Pelvic Organ Prolapse
Pessary for management of Pelvic Organ Prolapse Cathy Davis Clinical Nurse Specialist Department of Urogynaecology King’s College Hospital, London Definition of Prolapse The descent of one or more of the anterior vaginal wall, posterior vaginal wall, uterus (cervix) or vaginal vault (cuff scar after hysterectomy). The presence of any such sign should be correlated with relevant POP symptoms. (Haylen et al 2016) Risk Factors • Increased intra-abdominal pressure • Chronic cough • Chronic constipation • Weight lifting • Presence of abdominal tumours - fibroids & ovarian cysts • High impact exercise • Age/ Menopause • Obesity Risk Factors contd.... • Smoking • Multiparity • Congenital weakness – rare; due to deficiency in collagen metabolism • Injury to pelvic floor muscles • Iatrogenic/ pelvic surgery - hysterectomy Symptoms of POP • May be asymptomatic – a small amount of prolapse can often be normal • Sensation of a lump or bulge " coming down" - most common • Backache • Heaviness • Dragging or discomfort inside the vagina – often worse on standing /sitting for prolonged periods • Seeing a lump or bulge Symptoms of POP contd.... • Bladder / Urinary symptoms -Frequency -Difficulty initiating voids, low-flow, incomplete bladder emptying -Leakage on certain movements or when lifting heavy objects -Recurrent urinary tract infections • Bowel symptoms -Constipation - Incomplete bowel emptying - May have to digitate to defecate/use aides • Symptoms related to Sex – uncomfortable, lack of sensation Diagnosis of Prolapse • Vaginal examination • -

Most Common Robotic Bariatric Procedures: Review and Technical Aspects Pablo A
Acquafresca et al. Ann Surg Innov Res (2015) 9:9 DOI 10.1186/s13022-015-0019-9 REVIEW Open Access Most common robotic bariatric procedures: review and technical aspects Pablo A. Acquafresca1, Mariano Palermo1*, Tomasz Rogula2, Guillermo E. Duza1 and Edgardo Serra1 Abstract Since its appear in the year 1997, when Drs. Cadiere and Himpens did the first robotic cholecystectomy in Brus- sels, not long after the first cholecystectomy, they performed the first robotic bariatric procedure. It is believed that robotically-assisted surgery’s most notable contributions are reflected in its ability to extend the benefits of minimally invasive surgery to procedures not routinely performed using minimal access techniques. We describe the 3 most common bariatric procedures done by robot. The main advantages of the robotic system applied to the gastric bypass appear to be better control of stoma size, avoidance of stapler costs, elimination of the potential for oro- pharyngeal and esophageal trauma, and a potential decrease in wound infection. While in the sleeve gastrectomy and adjustable gastric banding its utility is more debatable, giving a bigger advantage during surgery on patients with a very large BMI or revisional cases. Keywords: Bariatric surgery, Robotic surgery, Gastric by pass, Sleeve gastrectomy, Gastric band Background laparoscopy and robotic laparoscopy is now a controver- Since its appear in the year 1997, when Drs. Cadiere and sial topic that concerns patients and surgeons alike. Himpens did the first robotic cholecystectomy in Brussels To date, the robotic technique is reported to be at least [1], the da Vinci™ Robotic Surgical System from Intuitive as safe and effective as the conventional approach for sev- Surgical, Inc., Sunny Vale, California (Fig. -

1: Gastro-Intestinal System
1 1: GASTRO-INTESTINAL SYSTEM Antacids .......................................................... 1 Stimulant laxatives ...................................46 Compound alginate products .................. 3 Docuate sodium .......................................49 Simeticone ................................................... 4 Lactulose ....................................................50 Antimuscarinics .......................................... 5 Macrogols (polyethylene glycols) ..........51 Glycopyrronium .......................................13 Magnesium salts ........................................53 Hyoscine butylbromide ...........................16 Rectal products for constipation ..........55 Hyoscine hydrobromide .........................19 Products for haemorrhoids .................56 Propantheline ............................................21 Pancreatin ...................................................58 Orphenadrine ...........................................23 Prokinetics ..................................................24 Quick Clinical Guides: H2-receptor antagonists .......................27 Death rattle (noisy rattling breathing) 12 Proton pump inhibitors ........................30 Opioid-induced constipation .................42 Loperamide ................................................35 Bowel management in paraplegia Laxatives ......................................................38 and tetraplegia .....................................44 Ispaghula (Psyllium husk) ........................45 ANTACIDS Indications: