The Nightmare of Litigation: a Survivor’S True Story After Being Sued, David Dreaded Seeing Patients and Felt Always on Guard
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

In This Issue
July 2020 NEWS Post-Traumatic Stress Disorder (PTSD) Assessment and Treatment In this Issue: Guidelines for Pediatric Primary Upcoming Clinical Care Conversations 5 Clinical Conversation: May 26, 2020 Presented by Sylvia Krinsky, MD, Tufts Medical Center For some children, childhood is far from a carefree time; they Leadership: experience trauma which can disrupt development and lead John Straus, MD to post-traumatic stress disorder (PTSD). At the May Clinical Founding Director Conversation, Sylvia Krinsky, MD, MCPAP site director at Tufts Barry Sarvet, MD Medical Center, discussed how to address PTSD in the primary Medical Director care setting. Beth McGinn Types of trauma Program Manager There are three major types of trauma: Elaine Gottlieb • Discrete Trauma – examples include a car accident, injury, Contributing Writer medical procedure, or a single episode of physical or sexual assault, when life is filled with otherwise helpful and supportive people • Complex Trauma – series of repeated traumas usually in close interpersonal contexts, such as childhood abuse or neglect, witnessing domestic or community violence, or racism and chronic social adversities • Adverse Childhood Event – a term from the Adverse Childhood Experiences (ACE) study, referring to potentially traumatic events that can have an impact on physical and psychological health Discrete trauma is most recognized in the DSM-5, while ACE is more familiar to the medical community, says Dr. Krinsky. 1000 Washington St., Suite 310 One study reported in the Journal of the American Medical Boston, MA 02118 Association (JAMA) found that more than 90 percent of pediatric Email: [email protected] patients seen in a primary care pediatric clinic had experienced a traumatic exposure, and 25 percent met full or partial criteria for www.mcpap.org PTSD. -

Acute Stress Disorder
Trauma and Stress-Related Disorders: Developments for ICD-11 Andreas Maercker, MD PhD Professor of Psychopathology, University of Zurich and materials prepared and provided by Geoffrey Reed, PhD, WHO Department of Mental Health and Substance Abuse Connuing Medical Educaon Commercial Disclosure Requirement • I, Andreas Maercker, have the following commercial relaonships to disclose: – Aardorf Private Psychiatric Hospital, Switzerland, advisory board – Springer, book royales Members of the Working Group • Christopher Brewin (UK) Organizational representatives • Richard Bryant (AU) • Mark van Ommeren (WHO) • Marylene Cloitre (US) • Augusto E. Llosa (Médecins Sans Frontières) • Asma Humayun (PA) • Renato Olivero Souza (ICRC) • Lynne Myfanwy Jones (UK/KE) • Inka Weissbecker (Intern. Medical Corps) • Ashraf Kagee (ZA) • Andreas Maercker (chair) (CH) • Cecile Rousseau (CA) WHO scientists and consultant • Dayanandan Somasundaram (LK) • Geoffrey Reed • Yuriko Suzuki (JP) • Mark van Ommeren • Simon Wessely (UK) • Michael B. First WHO Constuencies 1. Member Countries – Required to report health stascs to WHO according to ICD – ICD categories used as basis for eligibility and payment of health care, social, and disability benefits and services 2. Health Workers – Mulple mental health professions – ICD must be useful for front-line providers of care in idenfying and treang mental disorders 3. Service Users – ‘Nothing about us without us!’ – Must provide opportunies for substanve, early, and connuing input ICD Revision Orienting Principles 1. Highest goal is to help WHO member countries reduce disease burden of mental and behavioural disorders: relevance of ICD to public health 2. Focus on clinical utility: facilitate identification and treatment by global front-line health workers 3. Must be undertaken in collaboration with stakeholders: countries, health professionals, service users/consumers and families 4. -

The Relationship Between Dispositional Empathy, Psychological Distress, and Posttraumatic Stress Responses Among Japanese Unifor
Nagamine et al. BMC Psychiatry (2018) 18:328 https://doi.org/10.1186/s12888-018-1915-4 RESEARCH ARTICLE Open Access The relationship between dispositional empathy, psychological distress, and posttraumatic stress responses among Japanese uniformed disaster workers: a cross-sectional study Masanori Nagamine1* , Jun Shigemura2, Toshimichi Fujiwara3, Fumiko Waki3, Masaaki Tanichi2, Taku Saito2, Hiroyuki Toda2, Aihide Yoshino2 and Kunio Shimizu1 Abstract Background: Disaster workers suffer from psychological distress not only through the direct experience of traumatic situations but also through the indirect process of aiding disaster victims. This distress, called secondary traumatic stress, is linked to dispositional empathy, which is the tendency for individuals to imagine and experience the feelings and experiences of others. However, the association between secondary traumatic stress and dispositional empathy remains understudied. Methods: To examine the relationship between dispositional empathy and mental health among disaster workers, we collected data from 227 Japan Ground Self-Defense Force personnel who engaged in international disaster relief activities in the Philippines following Typhoon Yolanda in 2013. The Impact of Event Scale-Revised and the Kessler Psychological Distress Scale were used to evaluate posttraumatic stress responses (PTSR) and general psychological distress (GPD), respectively. Dispositional empathy was evaluated through the Interpersonal Reactivity Index, which consists of four subscales: Perspective Taking, Fantasy, Empathic Concern, and Personal Distress. Hierarchial linear regression analyses were performed to identify the variables related to PTSR and GPD. Results: High PTSR was significantly associated with high Fantasy (identification tendency, β =0.21,p < .01), high Personal Distress (the self-oriented emotional disposition of empathy, β =0.18,p <.05),andnoexperienceofdisaster relief activities (β =0.15,p < .05). -
Acute Stress Responses in Chinese Soldiers Performing Various Military Tasks Peng Huang1, Tengxiao Zhang2, Danmin Miao1* and Xia Zhu1*
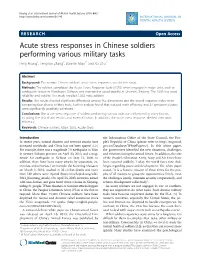
Huang et al. International Journal of Mental Health Systems 2014, 8:45 http://www.ijmhs.com/content/8/1/45 RESEARCH Open Access Acute stress responses in Chinese soldiers performing various military tasks Peng Huang1, Tengxiao Zhang2, Danmin Miao1* and Xia Zhu1* Abstract Background: To examine Chinese soldiers’ acute stress responses, we did this study. Methods: The soldiers completed the Acute Stress Response Scale (ASRS) when engaged in major tasks, such as earthquake rescue in Wenchuan, Sichuan, and maintaining social stability in Urumchi, Xinjiang. The ASRS has good reliability and validity. The study enrolled 1,832 male soldiers. Results: The results showed significant differences among five dimensions and the overall response index when comparing four diverse military tasks. Further analysis found that reduced work efficiency and 24 symptom clusters were significantly positively correlated. Conclusions: The acute stress response of soldiers performing various tasks was influenced by many factors, including the task characteristics and external factors. In addition, the acute stress response affected their work efficiency. Keywords: Chinese soldiers, Major tasks, Acute stress Introduction the Information Office of the State Council, the Peo- In recent years, natural disasters and terrorist attacks have ple’s Republic of China (please refer to http://eng.mod. increased worldwide, and China has not been spared [1,2]. gov.cn/Database/WhitePapers/). In this white paper, For example, there was a magnitude 7.0 earthquake in Ya’an the government identified the new situations, challenges, in western Sichuan province on April 20, 2013, and a mag- and missions facing the armed forces. In addition, the size nitude 8.0 earthquake in Sichuan on May 12, 2008. -

Medical Treatment Guidelines (MTG)
Post-Traumatic Stress Disorder and Acute Stress Disorder Effective: November 1, 2021 Adapted by NYS Workers’ Compensation Board (“WCB”) from MDGuidelines® with permission of Reed Group, Ltd. (“ReedGroup”), which is not responsible for WCB’s modifications. MDGuidelines® are Copyright 2019 Reed Group, Ltd. All Rights Reserved. No part of this publication may be reproduced, displayed, disseminated, modified, or incorporated in any form without prior written permission from ReedGroup and WCB. Notwithstanding the foregoing, this publication may be viewed and printed solely for internal use as a reference, including to assist in compliance with WCL Sec. 13-0 and 12 NYCRR Part 44[0], provided that (i) users shall not sell or distribute, display, or otherwise provide such copies to others or otherwise commercially exploit the material. Commercial licenses, which provide access to the online text-searchable version of MDGuidelines®, are available from ReedGroup at www.mdguidelines.com. Contributors The NYS Workers’ Compensation Board would like to thank the members of the New York Workers’ Compensation Board Medical Advisory Committee (MAC). The MAC served as the Board’s advisory body to adapt the American College of Occupational and Environmental Medicine (ACOEM) Practice Guidelines to a New York version of the Medical Treatment Guidelines (MTG). In this capacity, the MAC provided valuable input and made recommendations to help guide the final version of these Guidelines. With full consensus reached on many topics, and a careful review of any dissenting opinions on others, the Board established the final product. New York State Workers’ Compensation Board Medical Advisory Committee Christopher A. Burke, MD , FAPM Attending Physician, Long Island Jewish Medical Center, Northwell Health Assistant Clinical Professor, Hofstra Medical School Joseph Canovas, Esq. -

Pregnancy Loss and Infant Death: Understanding Grief and Trauma
Pregnancy Loss and Infant Death: Understanding Grief and Trauma by Cynthia Good, MS, LMHCA, IBCLC, CATSM www.lifecirclecc.com The loss of a baby during pregnancy, during birth, or after birth can be an indescribably painful and devastating experience. In the beginning, parents may feel a sense of disbelief, numbness, and shock. They may feel like their dreams for the future have been cruelly wrenched from them. They may experience guilt and ask unanswerable questions: Why my baby? Why me? Their arms and hearts may ache with emptiness. The reactions of friends and family, co- workers, and strangers may reflect ignorant insensitivity or the deepest compassion. Unfortunately, many societies do not fully recognize pregnancy loss and infant death as real losses, often leaving bereaved parents feeling invalidated and alone in their grief. Parents may feel great pressure to act as though they have “moved on” when they are actually still grieving and they have been changed forever by the living and the dying of their baby. They may quickly realize that few people are able to listen to them and to support them in their grief. Learning about the normalcy and healthiness of grief can be a critical step in finding ways to grieve well. Grief is the normal, healthy, healing, and painful process through which we learn how to continue living after a loss. Its emotional symptoms include sadness, anger, loneliness, guilt, anxiety, helplessness, shock, numbness, and yearning.1 When death brings freedom from an unbearable situation, such as watching a baby suffer, grief can also include feelings of relief— often accompanied by guilt about feeling that relief.1 Feelings of guilt can be intense when a parent has not yet had the chance to resolve ambivalent feelings, such as about a poorly-timed pregnancy or parenting a child with a congenital disorder, before the loss occurred. -

The Physician's Role in Managing Acute Stress Disorder
The Physician’s Role in Managing Acute Stress Disorder MICHAEL G. KAVAN, PhD; GARY N. ELSASSER, PharmD; and EUGENE J. BARONE, MD Creighton University School of Medicine, Omaha, Nebraska Acute stress disorder is a psychiatric diagnosis that may occur in patients within four weeks of a traumatic event. Features include anxiety, intense fear or helplessness, dissociative symptoms, reexperiencing the event, and avoidance behaviors. Persons with this disorder are at increased risk of developing posttraumatic stress disorder. Other risk factors for posttraumatic stress disorder include current or family history of anxiety or mood disorders, a history of sexual or physical abuse, lower cognitive ability, engaging in excessive safety behaviors, and greater symptom severity one to two weeks after the trauma. Common reactions to trauma include physical, mental, and emotional symptoms. Persistent psychological distress that is severe enough to interfere with psychological or social functioning may war- rant further evaluation and intervention. Patients experiencing acute stress disorder may benefit from psychological first aid, which includes ensuring the patient’s safety; providing information about the event, stress reactions, and how to cope; offering practical assistance; and helping the patient to connect with social support and other services. Cogni- tive behavior therapy is effective in reducing symptoms and decreasing the future incidence of posttraumatic stress disorder. Critical Incident Stress Debriefing aims to mitigate emotional distress through sharing emotions about the traumatic event, providing education and tips on coping, and attempting to normalize reactions to trauma. However, this method may actually impede natural recovery by overwhelming victims. There is insufficient evidence to recom- mend the routine use of drugs in the treatment of acute stress disorder. -
Transforming Trauma: Resilience and Healing Through Our Connections with Animals Philip Tedeschi University of Denver
Purdue University Purdue e-Pubs Purdue University Press Books Purdue University Press Summer 7-15-2019 Transforming Trauma: Resilience and Healing Through Our Connections With Animals Philip Tedeschi University of Denver Molly Anne Jenkins University of Denver Follow this and additional works at: https://docs.lib.purdue.edu/purduepress_ebooks Part of the Health Psychology Commons, and the Veterinary Medicine Commons Recommended Citation Tedeschi, Philip, and Jenkins, Molly Anne, Transforming Trauma: Resilience and Healing Through Our Connections With Animals. (2019). Purdue University Press. (Knowledge Unlatched Open Access Edition.) This document has been made available through Purdue e-Pubs, a service of the Purdue University Libraries. Please contact [email protected] for additional information. NEW DIRECTIONS IN THE HUMAN-ANIMAL BOND Series editors: Alan M. Beck and Marguerite E. O’Haire, Purdue University A dynamic relationship has always existed between people and animals. Each influences the psychological and physiological state of the other. This series of scholarly publications, in collaboration with Purdue University’s College of Veterinary Medicine, expands our knowledge of the interrelationships between people, animals, and their environment. Manuscripts are welcomed on all aspects of human-animal interaction and welfare, including therapy applications, public policy, and the application of humane ethics in managing our living resources. Other titles in this series: A Reason to Live: HIV and Animal Companions Vicki Hutton That Sheep May Safely Graze: Rebuilding Animal Health Care in War-Torn Afghanistan David M. Sherman Animal-Assisted Interventions in Health Care Settings: A Best Practices Manual for Establishing New Programs Sandra B. Barker, Rebcca A. Vokes, and Randolph T. -

Rodent Models of Post-Traumatic Stress Disorder: Behavioral Assessment Alexander Verbitsky 1, David Dopfel 2 and Nanyin Zhang 2,3
Verbitsky et al. Translational Psychiatry (2020) 10:132 https://doi.org/10.1038/s41398-020-0806-x Translational Psychiatry REVIEW ARTICLE Open Access Rodent models of post-traumatic stress disorder: behavioral assessment Alexander Verbitsky 1, David Dopfel 2 and Nanyin Zhang 2,3 Abstract Although the etiology and expression of psychiatric disorders are complex, mammals show biologically preserved behavioral and neurobiological responses to valent stimuli which underlie the use of rodent models of post-traumatic stress disorder (PTSD). PTSD is a complex phenotype that is difficult to model in rodents because it is diagnosed by patient interview and influenced by both environmental and genetic factors. However, given that PTSD results from traumatic experiences, rodent models can simulate stress induction and disorder development. By manipulating stress type, intensity, duration, and frequency, preclinical models reflect core PTSD phenotypes, measured through various behavioral assays. Paradigms precipitate the disorder by applying physical, social, and psychological stressors individually or in combination. This review discusses the methods used to trigger and evaluate PTSD-like phenotypes. It highlights studies employing each stress model and evaluates their translational efficacies against DSM-5, validity criteria, and criteria proposed by Yehuda and Antelman’s commentary in 1993. This is intended to aid in paradigm selection by informing readers about rodent models, their benefits to the clinical community, challenges associated with the translational models, and opportunities for future work. To inform PTSD model validity and relevance to human psychopathology, we propose that models incorporate behavioral test batteries, individual differences, sex differences, strain and stock differences, early life stress effects, biomarkers, stringent success criteria for drug development, Research Domain Criteria, technological advances, and cross-species comparisons. -

Classification of Trauma and Stressor-Related Disorders in Dsm-5
DEPRESSION AND ANXIETY 28: 737-749 (2011) Review CLASSIFICATION OF TRAUMA AND STRESSOR-RELATED DISORDERS IN DSM-5 Matthew J. Friedman, M.D. Ph.D., 1,2 Patricia A. Resick, Ph.D.,3,4 Richard A. Bryant, Ph.D.,5 James Strain, M.D.,6 Mardi Horowitz, M.D.,7 and David Spiegel, M.D.8,* This review examines the question of whether there should be a cluster of disorders, including the adjustment disorders (ADs), acute stress disorder (ASD), posttraumatic stress disorder (PTSD), and the dissociative disorders (DDs), in a section devoted to abnormal responses to stress and trauma in the DSM-5. Environmental risk factors, including the individual's developmental experience, would thus become a major diagnostic consideration. The relation ship of these disorders to one another is examined and also their relationship to other anxiety disorders to determine whether they are better grouped with anxiety disorders or a new specific grouping of trauma and stressor-related disorders. First how stress responses have been classified since DSM-III is reviewed. The major focus is on PTSD because it has received the most attention, regarding its proper placement among the psychiatric diagnoses. It is discussed whether PTSD should be considered an anxiety disorder, a stress induced fear circuitry disorder, an internalizing disorder, or a trauma and stressor-related disorder. Then, ASD, AD, and DD are considered from a similar perspective. Evidence is examined pro and con, and a conclusion is offered recommending inclusion of this cluster of disorders in a section entitled "Trauma and Stressor-Related Disorders." The recommendation to shift ASD and PTSD out of the anxiety disorders section reflects increased recognition of trauma as a precipitant, emphasizing common etiology over common phenomenology. -

Acute Stress Disorder & Posttraumatic Stress Disorder
Promoting recovery after trauma Australian Guidelines for the Treatment of Acute Stress Disorder & Posttraumatic Stress Disorder © Phoenix Australia - Centre for Posttraumatic Mental Health, 2013 ISBN Print: 978-0-9752246-0-1 ISBN Online: 978-0-9752246-1-8 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from Phoenix Australia - Centre for Posttraumatic Mental Health. Requests and inquiries concerning reproduction and rights should be addressed to Phoenix Australia - Centre for Posttraumatic Mental Health ([email protected]). Copies of the full guidelines, and brief guides for practitioners and the public are available online: www.phoenixaustralia.org www.clinicalguidelines.gov.au The suggested citation for this document is: Phoenix Australia - Centre for Posttraumatic Mental Health. Australian Guidelines for the Treatment of Acute Stress Disorder and Posttraumatic Stress Disorder. Phoenix Australia, Melbourne, Victoria. Legal disclaimer This document is a general guide to appropriate practice, to be followed only subject to the practitioner’s judgement in each individual case. The guidelines are designed to provide information to assist decision making and are based on the best information available at the date of publication. In recognition of the pace of advances in the field, it is recommended that the guidelines be reviewed and updated in five years’ time. Publication Approval These guidelines were approved by the Chief Executive Officer of the National Health and Medical Research Council (NHMRC) on 4 July 2013, under Section 14A of the National Health and Medical Research Council Act 1992. -

Evidence-Based Management for Acute Stress Disorder (ASD)
Center for the Study of Traumatic Stress Understanding the Effects of Trauma and Traumatic Events to Help Prevent, Mitigate and Foster Recovery for Individuals, Organizations and Communities A Program of Uniformed Services University, Our Nation’s Federal Medical School, Bethesda, Maryland • www. usuhs.mil/csts/ Evidence-Based Management for Acute Stress Disorder (ASD) Acute Stress Disorder (ASD) is characterized by dissociative ongoing assessment of safety and psychiatric status, symptoms (e.g. detachment, derealization, or amnesia) addressing co-morbid disorders, and increasing the during or after exposure to a traumatic event followed patient’s understanding of and coping with the effects of promptly by symptoms of re-experiencing, avoidance/ exposure to traumatic events through specific treatment numbing, and hyperarousal from two days to a maximum strategies (e.g. psycho-education, psychotherapy and/or of four weeks after the traumatic exposure. While not the pharmacotherapy) for ASD. only disorder seen acutely after exposure to traumatic events, ASD is quite common. The American Psychiatric PSYCHOTHERAPY—Early supportive psycho-education Association and the U.S. Department of Veterans Affairs and case management facilitate entry into other evidence- Office of Quality and Performance have published Practice based treatments. Cognitive Behavior Therapy (CBT) Guidelines for the treatment of ASD. For details see: may be helpful relatively acutely after traumatic exposure although heightened arousal and anxiety states may http://www.psych.org/psych_pract/treatg/pg/PTSD-PG- preclude some patients from absorbing information or PartsA-B-C-New.pdf and acquiring new coping skills in the immediate aftermath http://www.oqp.med.va.gov/cpg/PTSD/PTSD_cpg/ of trauma.