Addressing the Social Vulnerability of Mississippi Gulf Coast Vietnamese Community Through the Development of Community Health Advisors
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
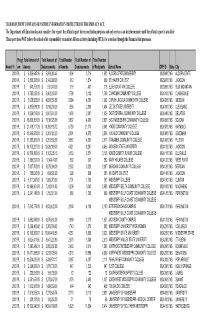
This Document Contains Sensitive Information Protected by the Privacy Act
THIS DOCUMENT CONTAINS SENSITIVE INFORMATION PROTECTED BY THE PRIVACY ACT. The Department of Education does not consider this report the official report for reconciliation purposes and only serves as an interim measure until the official report is available This report does NOT relieve the school of its responsibility to monitor all loan activity (including FFEL) for a student through the Financial Aid processes. Progr Total Amount of Total Amount of Total Number Total Number of Total Number Award Yr. am Awards Disbursements of Awards Disbursements of Recipients School Name OPE ID State City 2003 PL$ 6,326,645.96 $ 5,869,960.48 1,906 3,716 1,890 ALCORN STATE UNIVERSITY 00239600 MS ALCORN STATE 2003 PL$ 2,800,250.00 $ 2,142,998.00 912 1,574 909 BELHAVEN COLLEGE 00239700 MS JACKSON 2003 PL$ 543,551.00 $ 512,243.00 216 407 215 BLUE MOUNTAIN COLLEGE 00239800 MS BLUE MOUNTAIN 2003 PL$ 6,795,020.00 $ 5,463,803.00 1,799 3,132 1,799 COAHOMA COMMUNITY COLLEGE 00240100 MS CLARKSDALE 2003 PL$ 7,038,525.00 $ 4,820,750.58 2,024 4,780 1,992 COPIAH LINCOLN COMMUNITY COLLEGE 00240200 MS WESSON 2003 PL$ 4,835,689.38 $ 3,819,238.26 1,556 2,896 1,404 DELTA STATE UNIVERSITY 00240300 MS CLEVELAND 2003 PL$ 5,324,875.00 $ 3,987,661.00 1,539 2,687 1,536 EAST CENTRAL COMMUNITY COLLEGE 00240400 MS DECATUR 2003 PL$ 13,000,351.00 $ 7,015,325.00 3,837 4,981 2,637 EAST MISSISSIPPI COMMUNITY COLLEGE 00240500 MS SCOOBA 2003 PL$ 21,478,717.39 $ 14,390,815.72 6,759 21,771 5,943 HINDS COMMUNITY COLLEGE 00240700 MS RAYMOND 2003 PL$ 10,346,550.00 $ 6,391,020.20 2,901 4,572 -

The Marine and Brackish Water Mollusca of the State of Mississippi
Gulf and Caribbean Research Volume 1 Issue 1 January 1961 The Marine and Brackish Water Mollusca of the State of Mississippi Donald R. Moore Gulf Coast Research Laboratory Follow this and additional works at: https://aquila.usm.edu/gcr Recommended Citation Moore, D. R. 1961. The Marine and Brackish Water Mollusca of the State of Mississippi. Gulf Research Reports 1 (1): 1-58. Retrieved from https://aquila.usm.edu/gcr/vol1/iss1/1 DOI: https://doi.org/10.18785/grr.0101.01 This Article is brought to you for free and open access by The Aquila Digital Community. It has been accepted for inclusion in Gulf and Caribbean Research by an authorized editor of The Aquila Digital Community. For more information, please contact [email protected]. Gulf Research Reports Volume 1, Number 1 Ocean Springs, Mississippi April, 1961 A JOURNAL DEVOTED PRIMARILY TO PUBLICATION OF THE DATA OF THE MARINE SCIENCES, CHIEFLY OF THE GULF OF MEXICO AND ADJACENT WATERS. GORDON GUNTER, Editor Published by the GULF COAST RESEARCH LABORATORY Ocean Springs, Mississippi SHAUGHNESSY PRINTING CO.. EILOXI, MISS. 0 U c x 41 f 4 21 3 a THE MARINE AND BRACKISH WATER MOLLUSCA of the STATE OF MISSISSIPPI Donald R. Moore GULF COAST RESEARCH LABORATORY and DEPARTMENT OF BIOLOGY, MISSISSIPPI SOUTHERN COLLEGE I -1- TABLE OF CONTENTS Introduction ............................................... Page 3 Historical Account ........................................ Page 3 Procedure of Work ....................................... Page 4 Description of the Mississippi Coast ....................... Page 5 The Physical Environment ................................ Page '7 List of Mississippi Marine and Brackish Water Mollusca . Page 11 Discussion of Species ...................................... Page 17 Supplementary Note ..................................... -

Water-Resources Overview of the Mississippi Gulf Coast Area
WATER-RESOURCES OVERVIEW OF THE MISSISSIPPI GULF COAST AREA by B. E. Colson and E. H. doswell Hydrologists U. S. Geological Survey U. S. GEOLOGICAL SURVEY Open-File Report 85-94 Prepared in cooperation with the DEPARTMENT OF THE ARMY CORPS OF ENGINEERS MOBILE DISTRICT Jackson, Mississippi 1985 UNITED STATES DEPARTMENT OF THE INTERIOR WILLIAM P. CLARK, SECRETARY GEOLOGICAL SURVEY Dallas L. Peck, Director For additional Information write to: Copies of this report can be purchased from: District Chief Open-File Services Section U.S. Geological Survey Western Distribution Branch Water Resources Division U.S. Geological Survey 100 West Capital Street. Suite 710 Box 25425, Federal Center Jackson. Mississippi 39269 Lakewood. Colorado 80225 Telephone: (601) 960-4600 Telephone: (303) 234-5888 CONTENTS Page Abstract 1 Introduction - i 2 Purpose and scope 2 Physical setting 3 Water use -i__ - 7 Surface water ' ------------ 8 Principal drainage .r - 8 Pascagoula River t 8 Tchoutacabouffa River r 13 Biloxi River i 13 Wolf River r --- - 16 Jourdan River - 16 Pearl River 4 19 Surface-water quality ' 19 Floods 21 Tidal Records - 21 Ground water - 25 Aquifers - 25 Aquifer hydraulic characteristics 54 Water-level changes 56 Saltwater encroachment 56 Ground-water qual ity 61 Summary 63 Selected references 66 Appendix A-Index to surface-water quality data 69 Appendix B-Summary of ground-water quality data 109 ILLUSTRATIONS Figure 1. Map showing area of investigation, geographic features, and location of gaging and water-quality stations 4 2. Geologic map of a part of southern Mississippi 5 3. River basins and hydrologic units in Mississippi coastal area 9 Figures 4-9. -

Demolition of Historic Buildings on the Mississippi Gulf Coast
DEMOLITION OF HISTORIC BUILDINGS ON THE MISSISSIPPI GULF COAST IN THE WAKE OF HURRICANE KATRINA by GWEN K. JONES (Under the Direction of Wayde Brown) ABSTRACT This thesis examines the circumstances under which historic architectural resources were demolished in the aftermath of Hurricane Katrina on the Mississippi Gulf Coast. A brief history of three hurricane-related natural disasters in the United States addresses the political, economic, and social impacts post-disaster. Three case studies provide scenarios in which preservationists successfully, and unsuccessfully, collaborated in the aftermath of Hurricane Katrina to protect historic architectural resources on the Mississippi Gulf Coast. An analysis of factors that led to demolitions, the roles played by different levels of government and preservationists, and strategies that worked and did not work to prevent demolitions are also presented. INDEX WORDS: Historic preservation, Hurricane Katrina, Mississippi Gulf Coast, Demolition of historic architectural resources, Scenic Drive Historic District, Gulfport-Harrison County Public Library, East Ward School DEMOLITION OF HISTORIC BUILDINGS ON THE MISSISSIPPI GULF COAST IN THE WAKE OF HURRICANE KATRINA by Gwen K. Jones BA, University of Mississippi, 1995 A Thesis Submitted to the Graduate Faculty of the University of Georgia in Partial Fulfillment of the Requirements for the Degree MASTER OF HISTORIC PRESERVATION ATHENS, GEORGIA 2011 © 2011 Gwen K. Jones All Rights Reserved DEMOLITION OF HISTORIC BUILDINGS ON THE MISSISSIPPI GULF COAST IN THE WAKE OF HURRICANE KATRINA by GWEN K. JONES Major Professor: Wayde Brown / Mark Reinberger Committee: James Reap Judith Wasserman Ian Firth Electronic Version Approved: Maureen Grasso Dean of the Graduate School The University of Georgia August 2011 DEDICATION This thesis is dedicated to my mother and father. -

National Register of Historic Places Multiple Property Documentation Form
NPS Form 10-9OQ..b OMS No 1024-{)O '8 (Jan. \987) " United States Department of the Interior; National Park Service National Register of Historic Places Multiple Property Documentation Form This form is for use in documenting multiple property groups relating to one or several historic contexts. See instructions in Guidelines for Completing Narional Register Forms (National Register Bulletin 16). Complete each item by marking "x" in the appropriate box or by entering the requested information. For additional space use continuation sheets (Form 10-900-a). Type all entries. A. Name of Multiple Property Listing HISTORIC RESOURCES OF PASCAGOULA, MISSISSIPPI B. Associated Historic Contexts DEVELOPMENT IN PASCAGOULA, MISSISSIPPI - 1850-1941 ( a. ) Early Pascagollla to 1870 ( b. ) PascagollJa from 1870 to 1917 ( c. ) Pascagoula between the World Wars, 1917 - 1941. C. Geographical Data N0 See continuation sheet D. Certification As the designated authority under the National Historic Preservation Act of 1966, as amended, I hereby certify that this documentation form meets the National Register documentation standards and sets forth requirements for the listing of related properties consistent with the National Register criteria. This submission meets the procedural and professional requirements set forth in 36 CFR Part 60 and the Secretary of the Interior's Standards for Planning and Evaluation. ~ f-{. cp'V~ DCT. 24-, /9~1 Signature of certifying official Date Deputy State Historic Preservation Officer State or Federal agency and bureau I, hereby, certify that this multiple property documentation form has been approved by the National Register as a basis for evaluating related prope'rties for listing in the National Register. -

6 European Colonization in Mississippi
6 EUROPEAN COLONIZATION IN MISSISSIPPI1 JACK D. ELLIOTT, JR. INTRODUCTION The purpose of this report is to identify the cultural resources of Mississippi pertaining to the Period of European Colonization. The cultural resources include both sites and buildings. The term “sites” is the more inclusive of the two terms. Sites are the places at which past activities occurred and consequently include sites on which are located historic building, sites with archaeological remains, and even sites which were the scenes of past activities, yet at which there are no extant physical remains other than the physical landscape, associated with those events. The Period of European Colonization is separated from the preceding Period of European Exploration by the beginning of permanent European settlement. Permanent settlement is particularly important for the aspect of historic preservation programs that deal with Euro-American culture in that it marks the inception of a time period in which we first find significant numbers of sites and other remains of occupation. Prior to the beginning of permanent European settlement in Mississippi the European presence was confined to merely sporadic expeditions and wanderers that seldomed on the same site for more than a season at most. Such sites have typically been difficult if not impossible to identify. It has only been with the inception of permanent European settlement that we first have settlements that were sufficiently permanent that they can be identified through maps, written sources, and archaeological remains. Consequently, the distinction between the periods of exploration and colonization is more fundamental than that between the period of colonization and the succeeding periods under American jurisdiction. -

National Register of Historic Places Registration Form
NPS Form 10-900 OMB No. 1024-0018 (Expires 5/31/2012) United States Department of the Interior National Park Service National Register of Historic Places Registration Form 1. Name of Property historic name Moss Point Historic District other names/site number 2. Location Roughly bound by Dantzler, Davis, Griffin, Main, Payne and Weems Streets, street & number and Bellview, Ely, McInnis, Torres and Welch Avenues. _____ not for publication city or town Moss Point _____ vicinity state Mississippi code MS county Jackson code 059 zip code 39563 3. State/Federal Agency Certification As the designated authority under the National Historic Preservation Act, as amended, I hereby certify that this X nomination request for determination of eligibility meets the documentation standards for registering properties in the National Register of Historic Places and meets the procedural and professional requirements set forth in 36 CFR Part 60. In my opinion, the property X meets does not meet the National Register Criteria. I recommend that this property be considered significant at the following level(s) of significance: national statewide X local Signature of certifying official/Title Date State or Federal agency/bureau or Tribal Government In my opinion, the property ____meets ____does not meet the National Register criteria. Signature of commenting official Date Title State or Federal agency/bureau or Tribal Government 4. National Park Service Certification I hereby certify that this property is: _____ entered in the National Register _____ determined eligible for the National Register _____ determined not eligible for the National Register _____ removed from the National Register _____ other (explain) ________________________________________________________________________________________ Signature of the Keeper Date of Action 1 United States Department of the Interior National Park Service/National Register of Historic Places Registration Form NPS Form 10-900 OMB No. -

MIDDLEGATE JAPANESE GARDENS Japan on the Gulf of Mexico by Anne Legett
MIDDLEGATE JAPANESE GARDENS Japan on the Gulf of Mexico by Anne Legett Fig. 1. Rudolf Hecht, Middlegate Japanese Garden (courtesy of Harry Stegenga, grandson of John Dambrink, Pass Christian, MS) REMEMBERING A GARDEN nce there were the most enchanting gardens in Pass Christian on the OMississippi Gulf Coast about 70-miles east of New Orleans, Louisiana. Middlegate Japanese Gardens were almost a secret, not visible to the street, and many residents were not even aware of the gardens’ existence. Rudolf Hecht, wealthy New Orleans entrepreneur, and his wife, Lynne Watkins Hecht, created the gardens at their beach “cottage” to preserve fond memories of their travels in Japan.1 My interest in the story of Middlegate Japanese Gardens has been life long. At the age of 12, I first passed through the bamboo gate at the St. Louis Street entrance and walked under the blue tile roof leading into the garden. Like Alice stepping through the looking glass, I passed from the small Gulf Coast town of Pass Christian in the 1950s into a Japanese dreamscape unlike anything I had ever imagined. With the property facing the beach road of Pass Christian (US Highway 90), I could still hear automobile traffic and smell the sea breeze. Though seagulls called above, all that was familiar in my world melted away. I had not traveled. The center of my universe was the Mississippi Gulf Coast and my journeys were limited to the Louisiana and Mississippi waters of the Gulf of Mexico. My tour of Middlegate, though but a few miles from my home, was my first visit to a foreign place. -

24-453-410 MS Utilities
3 1 8 2 7 6 Itta Bena 4 6 MISSISSIPPI 7 4 5 2 3 5 13 9 9 12 8 14 LOUISIANA ALABAMA 1 Lorman 10 15 10 9 386 miles 3 To Memphis, TN 8 Four-Year Institutions 1 Two-Year Institutions 40.1 miles JACKSON Private Colleges & Universities COUNTY To Mobile, AL 110 Miles 6 2 11 4 To New Orleans. LA 5 11 7 Gulf of Mexico 3033 Pascagoula Street • P.O. Drawer 1558 • Pascagoula, MS 39568-1558 Southern MS Utilities Distric Map Phone: 228-769-6263 • Toll-Free: 1-800-362-0103 • Fax: 228-762-8431 Colleges and Universities FOUR-YEAR INSTITUTION 1 Alcorn State University Location: Lorman, MS 2 Delta State University Location: Cleveland, MS 3 Jackson State University Location: Jackson, MS 4 Mississippi State University (Main Campus) Location: Starkville, MS 5 Mississippi State University (Meridian Campus) Location: Meridian, MS 6 Mississippi University for Women Location: Columbus, MS 7 Mississippi Valley State University Location: Itta Bena, MS 8 University of Mississippi Location: Oxford, MS 9 University of Mississippi Medical Center Location: Jackson, MS 10 The University of Southern Mississippi (Main Campus) Location: Hattiesburg, MS 11 The University of Southern Mississippi (Long Beach) Location: Long Beach, MS 3033 Pascagoula Street • P. O. Drawer 1558 • Pascagoula, MS 39568-1558 • Phone: 228-769-6263 • Toll-Free: 1-800-362-0103 • Fax: 228-762-8431 Colleges and Universities TWO-YEAR INSTITUTION 1 Mississippi Gulf Coast Community College (Main Campus) Location: Perkinston, MS 2 Mississippi Gulf Coast Community College (Applied Technology and Development -

Community Health Needs Assessment 2018
2018 Community Health Needs Assessment Prepared By: Melissa Schnoor, Community Benefit Manager Community Benefit Department Adopted August 29, 2018 Report available at www.singingriverhealthsystem.com Adopted August 26, 2015 Report available at www.singingriverhealthsystem.com Table of Contents Executive Summary .................................................................................................................................................................... 5 Introduction .................................................................................................................................................................................. 7 About Singing River Health System ..................................................................................................................................... 7 Defined Community .......................................................................................................................................................... 9 Demographics ............................................................................................................................................................................ 10 Population ........................................................................................................................................................................... 10 Economy ............................................................................................................................................................................. -

Biloxi, Mississippi These Days
One blow after another Biloxi, Mississippi Biloxi-Gulfport and Mississippi’s entire 70-mile coastline have endured a traumatic seven years. First, Hurricane Katrina Biloxi-Gulfport wreaked havoc, temporarily costing Biloxi-Gulfport 25,000 jobs. Three years later came the recession and financial Economy Keeps crisis. In addition to the general economic slowdown, the financial crisis constrained investment needed to build the spectacu- Coming Back lar gaming resorts envisioned here after Katrina laid waste to the existing casinos. Finally, the BP oil spill fouled the 2010 summer tourist season, delivering the coastal economy a third body blow. Higher ife on the Mississippi Gulf Coast in gas prices haven’t helped either, as most of the 21st century compels one to take Biloxi-Gulfport’s visitors drive in. L the long view. “It’s tough right now, but it’ll pass,” For instance, “growth was stymied” said Dave Dennis, president of Specialty along the Mississippi coast during 2011, Contractors & Associates Inc. in Gulfport says a report from the Gulfport-based Gulf and former chairman of the Atlanta Fed’s Coast Business Council, a think tank and New Orleans Branch board of directors. economic development group. Sales tax Dennis’s optimism centers on the collections on the coast fell, and the Biloxi- area’s tourism prospects. The main draw Gulfport metropolitan area lost 500 jobs. remains what it’s been for the past 20 Activity dipped mainly for two rea- years: the slots, dice, cards, and stage sons, according to Scott King, director shows of coastal Mississippi’s casinos. of research and policy for the Business Since their inception in the early Council. -

Mississippi Tourism Ephemera
Mississippi Tourism Ephemera Collection Title: Mississippi Tourism Ephemera Manuscript No.: M026 Inclusive Dates: 1948 – 1976 Bulk Dates: 1960s Volume: .25 cu. Ft. Scope and Content This collection contains publications about some of the most popular tourist attractions in different areas of Mississippi such as Clarksdale, Natchez, Vicksburg, and the Gulf Coast during the 1940s through the 1970s and into the 1980s. These brochures provided tourists with information on where to dine, places to shop, and historical sites to visit. There are also several publications within this collection that pertain to the historical background and economic development of the cities mentioned above. Box Inventory Folder 1: Brochures Concerning the Mississippi Gulf Coast This folder contains brochures concerning the Mississippi Gulf Coast. Brochures of famous tourist attractions such as the Old Spanish Fort in Pascagoula, Mississippi and The Whistle Stop in Ocean Springs, Mississippi are included as well. 1960s – 1980s. Folder 2: Brochures Concerning Clarksdale and Oxford, Mississippi This folder contains a bi-monthly publication on Clarksdale, Mississippi that was printed as a guide to scenic and historical sites in and around Clarksdale. In this folder, there are also several brochures concerning Oxford, Mississippi and Mississippi in general. 1950s – 1980s. Folder 3: Brochures and Publications Concerning Natchez, Mississippi This folder contains a copy of Scenic South (1958), a publication about certain tourist attractions in Natchez. There are also brochures about the Natchez Pilgrimage (1948, 1953, 1956, 1957). Newspaper clippings and magazine articles concerning Natchez can be found in this folder as well. 1940s – 1970s. Folder 4: Brochures and Publications Concerning Jackson, Mississippi This folder contains several publications concerning Jackson (1964, 1968, and 1969).